Left Ventricular to Right Atrial Shunt in a Preterm Infant: A Case Report
Aimann Surak

TL;DR
A rare heart condition in a preterm infant was detected using targeted neonatal echocardiography, highlighting its importance in early diagnosis.
Contribution
Demonstrates the utility of targeted neonatal echocardiography in identifying a rare cardiac shunt in a preterm infant.
Findings
Left ventricular to right atrial shunt was diagnosed in a preterm infant using targeted neonatal echocardiography.
The case underscores the value of echocardiography in detecting rare cardiac anomalies in neonates.
Early detection enabled timely management and improved clinical outcomes for the infant.
Abstract
Background and Clinical Significance: Premature infants are at high risk of life-threatening complications due to the immaturity of multiple organ systems, and close monitoring in neonatal intensive care units is indispensable for their stabilization, survival, and morbidities. Despite major advances in perinatal care, cardiovascular pathology remains one of the most frequent morbidities in this population. Targeted neonatal echocardiography is implemented in many neonatal intensive care units around the world; it provides earlier and precise assessment during hemodynamic instability, allowing targeted management and follow-up. It can also detect red flags for anatomical heart defects. Left ventricular to right atrial shunt is a rare and presents a challenging diagnostic entity in very premature neonates. Case Presentation: We present a case of left ventricular to right atrial shunt in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1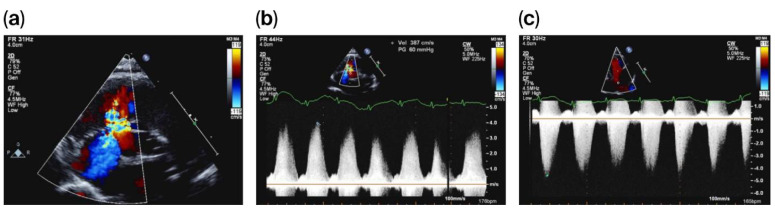 Figure 2
Figure 2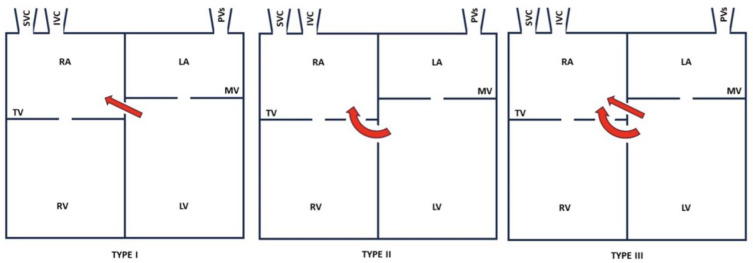 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Neonatal Respiratory Health Research · Cardiovascular and Diving-Related Complications
1. Introduction and Clinical Significance
Over the last decade, targeted neonatal echocardiography (TnECHO) has been increasingly used in neonatal intensive care units (NICUs) around the world [1]. In addition to its major role in diagnosing specific hemodynamic pathophysiologies, it is critical in recognizing red flags in abnormal cardiac anatomy [2]. Left ventricular to right atrial shunt (LVRAS) is uncommon in neonates with an anatomically normal heart; however, it has been increasingly recognized and reported [3].
In this report, we present a case of a preterm infant with LVRAS with a co-existing peri-membranous ventricular septal defect (PMVSD). This is the first case of LVRAS to be reported by a TnECHO team.
2. Case Presentation
We present a male preterm infant, born at 31 weeks’ gestation to a 33-year-old primigravida mother. Pregnancy was complicated by premature ruptured membranes, gestational diabetes, and placental abruption. The infant was delivered by cesarean section, indicated by breech presentation and fetal heart rate decelerations. Deferred cord clamping was not performed due to concerns about placental abruption. Resuscitation included positive-pressure ventilation, followed by a quick transition to non-invasive continuous positive airway pressure (CPAP). APGARs were 7 and 9 at 1 and 5 min, respectively. Birth weight was 1600 g. The infant was admitted to the NICU for ongoing care and management. A central umbilical venous catheter was inserted successfully.
Initially, the infant remained on CPAP with minimal oxygen and was trialed off on day 5 of life, which he tolerated well. A loading dose of caffeine was given after birth, and a daily maintenance dose continued. Trophic feeds were initiated shortly after delivery, and feeds progressed gradually. The infant remained in room air, with no increased work of breathing. Subsequently, intravenous parenteral nutrition was weaned off, and full feeding was achieved on day 10 of life.
On day 20 of life, and due to a heart murmur on auscultation, TnECHO was requested. At our center, we perform TnECHO using a Philips iE33 Ultrasound Machine with a high-frequency 12 MHz phased-array probe (Figure 1). Echocardiography findings revealed a large peri-membranous ventricular septal defect (PMVSD) measuring approximately 4 mm, with left-to-right restrictive flow, with a peak gradient of 4 m/s, as shown in Figure 2. Biventricular systolic function was normal. Echocardiographic markers of pulmonary hypertension were reassuring and revealed a rounded intraventricular septum during systole (systolic left ventricular eccentricity index of 1), demonstrating a parabolic mean pulmonary artery flow Doppler pattern, with a pulmonary artery acceleration time to right ventricular ejection time (PAAT/RVET) ratio of 0.35 and a right ventricular output of ~400 cc/k/min. Tricuspid annular plane systolic excursion (TAPSE) was 8.5 mm, right ventricular fraction area change (RVFAC) was 40%, and tricuspid valve S’ (TV S’) was 5 cm/s. However, there was a significant tricuspid regurgitation jet with a peak velocity of 4 m/s, estimating a right ventricular peak systolic pressure of 70 mmHg, which is at the systemic level. Of note, this regurgitation jet was eccentric, adjacent to the VSD jet, as shown in Figure 2.
In consultation with pediatric cardiology, the diagnosis of pulmonary hypertension was deemed unlikely. This was due to the reassuring echocardiographic markers (other than tricuspid regurgitation) and clinically stable status. Chest X-ray was also reassuring and negative for pulmonary edema. A diagnosis of LVRAS was suspected by the pediatric cardiology team as an etiology for the tricuspid regurgitation jet. Conservative management was recommended. The infant remained in room air and hemodynamically stable. Subsequently, the infant was discharged home at approximately 36 weeks of corrected gestation. The infant was followed up as an outpatient at the local pediatric cardiology clinic; the tricuspid regurgitation was not observed and was likely to have subsequently resolved. The infant has been growing well with no clinical concerns.
3. Discussion
LVRAS was first described in 1958 by Gerbode et al. [4]. It can be either congenital (Gerbode defect) or acquired [5,6,7,8]. Normally, the tricuspid valve is located below the mitral valve. Hence, a part of the septum between these two chambers might become ruptured as a complication of cardiac surgery, endocarditis, trauma or myocardial infarction [9].
Anatomically, this may be above (type I), or below the tricuspid valve (type II) or both (type III), as shown in Figure 3 [4,10]. In the latter two cases, a PMVSD often exists in the tricuspid valve septal leaflet. The tricuspid valve may be abnormal (cleft, widened commissural space, or perforated) [11,12]. An abnormal case of tricuspid chordae causing regurgitation has also been reported [13].
The diagnosis of LVRAS is challenging due to the diagnostic accuracy of echocardiography. Therefore, it is important to always consider LVRAS when an unexplained turbulent flow is observed in the right cardiac chamber. Other modalities used for diagnosis include transesophageal echocardiography (TEE), cardiac magnetic resonance imaging (CMRI), and computed tomographic angiography [14]. As TnECHO is often the first modality used in many NICUs, it has become a crucial first step in the diagnosis (screening) of congenital heart defects, highlighting its diagnostic value and the prognostic implications.
In our case, the echocardiography findings were likely consistent with type II LVRAS with a co-existing PMVSD similar to what is described in the literature. Our case confirms the importance of integrating echocardiographic markers with components of a clinical exam to establish the diagnosis. Additionally, our TnECHO team recognized multiple other defects, providing an early diagnosis of a significant cardiac condition and allowing for earlier intervention. Guidelines on the use of TnECHO have been adopted to optimize monitoring in the NICU [15,16,17]. Additionally, in our case, the assessment occurred at day 20 of life due to the clinical concerns mentioned above; it is possible that an earlier TnECHO would have resulted in an earlier diagnosis. As the infant remained stable during the NICU course, an earlier assessment would probably not have resulted in a better outcome in this particular case. However, in other cases of pathological heart defects, an earlier diagnosis may impact the outcomes.
Implementation of this tool is associated with improved outcomes, refs. [18,19] and it facilitates “precision medicine” by detecting pathophysiological factors and continuously evaluating fluctuations in hemodynamics [20]. In conclusion, our case is a good example of the successful use of TnECHO in diagnosis, management, and follow-up in the NICU. Additionally, high suspicions of red flags for heart defects while performing TnECHO should always be followed; furthermore, collaboration and ongoing discussions with the pediatric cardiology team are also important.
4. Conclusions
TnECHO can detect red flags for rare congenital heart disease. Careful evaluation of every murmur is crucial, and TnECHO is beneficial in this regard.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alammary D. Narvey M. Soni R. Elsayed Y. Louis D. Targeted neonatal echocardiography service in neonatal intensive care in Manitoba, Canada J. Perinatol.20224265565910.1038/s 41372-021-01258-534716384 · doi ↗ · pubmed ↗
- 2Bischoff A.R. Giesinger R.E. Rios D.R. Mertens L. Ashwath R. Mc Namara P.J. Anatomic Concordance of Neonatologist-Performed Echocardiography as Part of Hemodynamics Consultation and Pediatric Cardiology J. Am. Soc. Echocardiogr.20213430130710.1016/j.echo.2020.11.00533220434 · doi ↗ · pubmed ↗
- 3Yuan S.M. Left ventricular to right atrial shunt (Gerbode defect): Congenital versus acquired Postep. Kardiol. Interwencyjnej.20141018519410.5114/pwki.2014.4514625489305 PMC 4252310 · doi ↗ · pubmed ↗
- 4Gerbode F. Hultgren H. Melrose D. Osborn J. Syndrome of left ventricular-right atrial shunt; successful surgical repair of defect in five cases, with observation of bradycardia on closure Ann. Surg.195814843310.1097/00000658-195809000-0001213571920 PMC 1450812 · doi ↗ · pubmed ↗
- 5Weinrich M. Graeter T.P. Langer F. Schäfers H.J. Left ventricular-right atrial fistula complicating redo mitral valve replacement Ann. Thorac. Surg.20017134334510.1016/S 0003-4975(00)02154-811216776 · doi ↗ · pubmed ↗
- 6Sun X. Yang C. Zhou G. Wang C. Acquired left ventricular-right atrial communication following mitral valve replacement J. Heart Valve Dis.20101980180221214110 · pubmed ↗
- 7Okamura T. Nagase Y. Mitsui F. Shibairi M. Left Ventricular-Right Atrial Communication Complicated by Aortic Regurgitation Asian Cardiovasc. Thorac Ann 200816 e 1e 310.1177/02184923080160012618245691 · doi ↗ · pubmed ↗
- 8Kelle A.M. Young L. Kaushal S. Elise Duffy C. Anderson R.H. Backer C.L. The gerbode defect: The significance of a left ventricular to right atrial shunt Cardiol. Young 200919969910.1017/S 104795110999168519857356 · doi ↗ · pubmed ↗