Successful Treatment of Median Nerve Mononeuropathy Occurring After Brachial Arterial Line Placement for a Prolonged Prone Spine Surgery With Ultrasound-Guided Peripheral Nerve Stimulation: A Case Report
Varun Channagiri

TL;DR
A patient with long-term nerve damage from a brachial artery line during surgery showed significant improvement using ultrasound-guided nerve stimulation.
Contribution
Demonstrates the effectiveness of ultrasound-guided peripheral nerve stimulation for treating chronic median nerve injury after arterial cannulation.
Findings
The patient experienced over 50% pain reduction and improved dexterity after PNS treatment.
Ultrasound-guided PNS provided continued benefit alongside medication and therapy.
The case supports PNS as a feasible option when conservative treatments fail for iatrogenic nerve injury.
Abstract
Median nerve injury after brachial arterial access is uncommon but clinically meaningful, typically related to direct needle trauma, hematoma, pseudoaneurysm, or ischemia from arterial compromise. We report a case of a 66-year-old man with persistent neuropathic pain and sensory loss in the thumb to middle fingers, with symptom onset after a 12-hour prone spine surgery during which a brachial arterial line was placed. Symptoms persisted for more than one year despite conservative therapy. Electrodiagnostic testing demonstrated a chronic focal mononeuropathy of the median nerve with superimposed sensory polyneuropathy. Under ultrasound guidance, a percutaneous 60-day peripheral nerve stimulation (PNS) lead (SPRINT®, SPR Therapeutics, Cleveland, OH) was placed adjacent to the proximal median nerve. At two-month follow-up, the patient reported greater than 50% pain reduction, improved…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
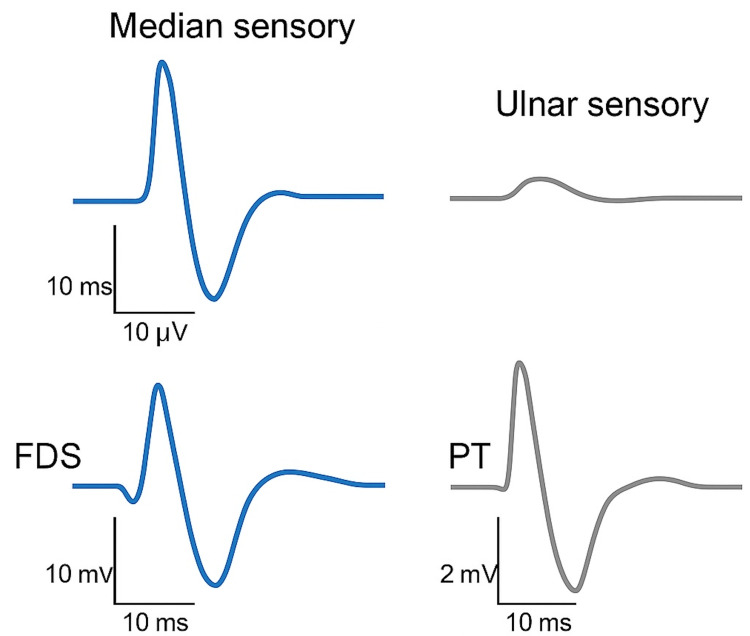 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPain Management and Treatment · Anesthesia and Pain Management · Intraoperative Neuromonitoring and Anesthetic Effects
Introduction
Median nerve mononeuropathy most commonly reflects distal compression at the wrist; however, proximal injury can occur after vascular access in the antecubital fossa, where the brachial artery and median nerve lie in close proximity. Reported median nerve complications after brachial artery catheterization are uncommon but may be underrecognized and can lead to persistent functional deficits if not recognized and addressed in a timely fashion [1]. Mechanisms include direct needle trauma, hematoma or pseudoaneurysm causing compression, and ischemic injury; the risk may be higher with axillary or brachial access than with more superficial radial access [2]. Prolonged prone positioning and difficult hemostasis may further predispose to nerve injury. We describe a delayed median neuropathy after brachial arterial line placement for a prolonged spine surgery, successfully managed with ultrasound-guided percutaneous 60-day peripheral nerve stimulation (PNS).
Case presentation
A 66-year-old man presented with chronic neuropathic pain and numbness in the thumb, index, and middle fingers of the left hand beginning after a prolonged (approximately 12-hour) prone spine procedure during which a brachial arterial line was placed for monitoring. Symptoms persisted for more than one year and were refractory to splinting, activity modification, physical and occupational therapy, and neuropathic agents.
Examination demonstrated sensory loss in the median distribution and impaired fine motor tasks. Electrodiagnostic testing (standard nerve conduction studies and needle electromyography) demonstrated a chronic focal median mononeuropathy localizing to the proximal forearm, consistent with axonal loss with demyelinating features. Background length-dependent sensory polyneuropathy was also present. Findings supported the clinical diagnosis and excluded radiculopathy or plexopathy (Figure 1).
Representative Electromyography and Nerve Conduction TracingFDS, flexor digitorum superficialis; PT, pronator teres.
Given persistent pain and functional limitation despite conservative therapy, the patient elected to trial percutaneous 60-day PNS lead (SPRINT^®^, SPR Therapeutics, Cleveland, OH) placement.
Intervention
Under sterile conditions, the proximal forearm to the elbow was prepared. Using ultrasound, the brachial artery and median nerve were identified, and a local anesthetic was administered to the skin and subcutaneous tissue overlying the target structures but outside the planned lead trajectory to avoid confounding stimulation testing. A 17-gauge insulated stimulating introducer was advanced in-plane to the median nerve (proximal to the cubital fossa), and test stimulation reproduced the patient’s typical paresthesia in the first three digits at comfortable amplitudes. A percutaneous 60-day PNS lead was deployed, then retested to confirm appropriate distribution. Post-procedure programming optimized frequency and pulse width, and the patient was instructed on device care and remote use.
Outcomes
At two-month follow-up, the patient reported greater than 50% reduction in pain intensity (average daily pain score recorded in pain diary down to 3/10 by numeric rating scale (NRS) at follow-up versus 8/10 pre-procedure) and improved dexterity enabling fuller participation in therapy. Continuous low-level stimulation was well tolerated. The PNS leads were removed at this time. The patient continued venlafaxine and capsaicin 0.1% cream, with plans for tapering based on functional progress. At one-year follow-up, the patient reported sustained 50% reduction in pain intensity (average daily pain score of 4/10 by NRS in pain diary) and had stopped using the capsaicin 0.1% cream.
Discussion
Median nerve injury after brachial arterial instrumentation is rare but clinically important. Broader reviews of arterial interventions confirm that nerve injuries, while uncommon, are most frequently reported with axillary and brachial access because of tight neurovascular relationships and challenges in achieving hemostasis; hematoma and pseudoaneurysm formation are frequent contributors [2]. Case reports also describe median neuropathy after brachial or axillary catheterization due to pseudoaneurysm compression, direct trauma, or ischemia [1,3-5].
Unlike many previously reported cases, which typically manifest within days to weeks of vascular access, our patient developed symptoms more than a year after a prolonged prone spine procedure with a brachial arterial line in place. The delayed presentation distinguishes this case and suggests a possible mechanism of chronic low-grade compression or microvascular ischemia rather than acute trauma. Electrodiagnostic findings showing both axonal loss and demyelinating features support a mixed injury pattern, differing from the primarily demyelinating lesions described in acute compressive neuropathies [3,4].
Few reports have detailed management strategies once such chronic focal median mononeuropathies develop. Conservative measures, including neuropathic medications, splinting, and physical therapy, often provide incomplete relief. Surgical exploration or decompression may be considered when a structural lesion such as a pseudoaneurysm or fibrotic entrapment is identified, but outcomes are variable and frequently incomplete [5-7].
In contrast, ultrasound-guided PNS has emerged as a minimally invasive, motor-sparing option for focal neuropathic pain refractory to conservative care. Published experiences demonstrate meaningful and durable analgesia in upper-extremity neuropathic conditions, including brachial plexus, suprascapular, and median nerve distributions [8-10]. Compared with spinal cord stimulation or repeated local anesthetic injections, PNS enables focal targeting, preserves motor function, and avoids the need for permanent implants. In our case, a 60-day percutaneous system provided more than 50% pain reduction and functional improvement, allowing the patient to resume activities of daily living.
This case adds to the limited literature describing post-arterial-access median neuropathies and highlights that even delayed presentations can respond to PNS. Awareness of this potential iatrogenic etiology is important for clinicians evaluating otherwise unexplained median neuropathic pain, especially when there is a history of brachial or axillary vascular access.
Conclusions
Median nerve neuropathy can occur as a delayed complication of brachial arterial cannulation, even when the access event occurred months or years earlier. Clinicians should specifically ask about prior upper-extremity vascular lines and pursue focused electrodiagnostic testing when symptoms localize to the proximal median nerve.
For patients with persistent, medication-refractory focal neuropathic pain and no surgically correctable lesion, ultrasound-guided percutaneous PNS offers a practical, motor-sparing therapeutic option that can restore function and quality of life. Early recognition of this rare iatrogenic entity may facilitate timely referral for neuromodulation and improved outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Median nerve injury: An underrecognised complication of brachial artery cardiac catheterisation?J Neurol Neurosurg Psychiatry Kennedy AM Grocott M Schwartz MS Modarres H Scott M Schon F 542546631997934314310.1136/jnnp.63.4.542PMC 2169787 · doi ↗ · pubmed ↗
- 2Avoiding peripheral nerve injury in arterial interventions Diagn Interv Radiol Kuo F Park J Chow K Chen A Walsworth MK 3803912520193131024010.5152/dir.2019.18296 PMC 6727823 · doi ↗ · pubmed ↗
- 3High median nerve palsy caused by pseudoaneurysm after brachial catheterization: Two case reports J Med Cases Ochi M Iwase G Mizuno S 333582017
- 4[Two cases of median nerve palsy due to pseudoaneurysm after catheter manipulation from the brachial artery at the elbow]J Jpn Elbow Soc Noguchi R Teshima M 156158282021
- 5Brachial pseudoaneurysm associated with median nerve injury as a complication of peripherally inserted central catheter: A case report Arch Case Rep Kauffman P Helito AS Poltronieri MJA Garcia MR Viana PCC 91332019
- 6Brachial artery pseudoaneurysm presenting as median nerve neuropathy IJVES Case Rep Sai GN Venkat N Reddy KA 161832025
- 7Peripheral nerve stimulation of brachial plexus nerve roots and supra-scapular nerve for chronic refractory neuropathic pain of the upper limb Neuromodulation Bouche B Manfiotto M Rigoard P Lemarie J Dix-Neuf V Lanteri-Minet M Fontaine D 6846892020172816036410.1111/ner.12573 · doi ↗ · pubmed ↗
- 8Ultrasound-guided percutaneous peripheral nerve stimulation for the treatment of chronic intractable pain originating from a lipofibromatous hamartoma of the median nerve J Hand Surg Am Ferreira-Dos-Santos G Hurdle MF Gupta S Ghazi SM Trigg SD Clendenen SR 25025546202110.1016/j.jhsa.2020.06.00332698979 · doi ↗ · pubmed ↗