Unilateral anomalous lateral branch of the abdominal aorta piercing the left renal vein – A case report
Surekha Devadasa Shetty, Ashwini Aithal Padur, Sapna Marpalli, Satheesha Badagabettu Nayak

TL;DR
This case report describes a rare anatomical variation of the abdominal aorta that could impact surgical and radiological procedures.
Contribution
The report presents a previously undocumented unilateral anomalous lateral branch of the abdominal aorta piercing the left renal vein.
Findings
The anomalous branch originated from the abdominal aorta behind the left renal vein and pierced it.
The artery supplied the posterior abdominal wall muscles and surrounding kidney tissues.
This variation poses risks for bleeding during surgery and potential misinterpretation in radiology.
Abstract
A sound knowledge of variations in the branching pattern of the abdominal aorta is crucial for operative, diagnostic, and endovascular procedures. We report a unilateral anomalous lateral branch of the abdominal aorta observed during dissection classes.This anomalous branch took origin from the anterior surface of the abdominal aorta behind the left renal vein and pierced the left renal vein. After piercing the left renal vein, it traced a tortuous course through the peri-renal fat pad in front of the lower part of the left kidney. The artery then ran downward and laterally, pierced the anterior layer of thoracolumbar fascia, and continued to the posterior abdominal wall to supply its muscles. It also supplied the fat and fasciae around the kidney. Such an anomalous lateral branch could bleed significantly during renal surgery. It could also mislead radiologists during the invasive…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
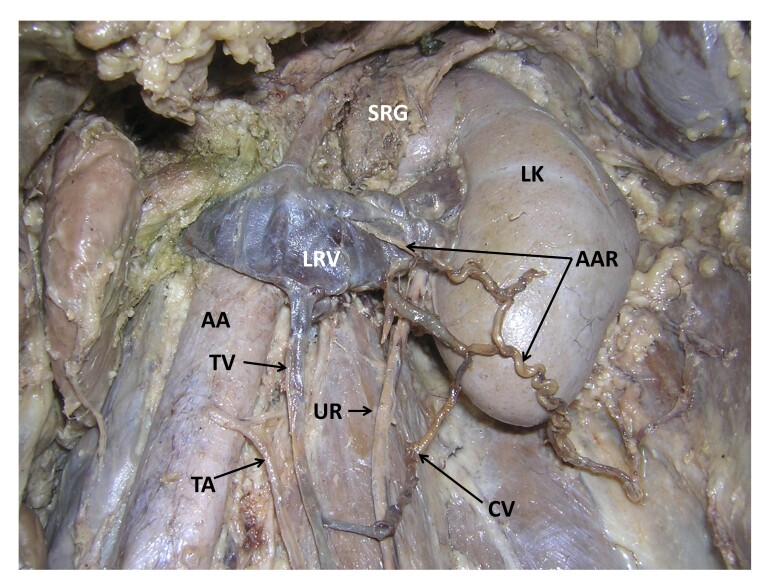 Figure 1
Figure 1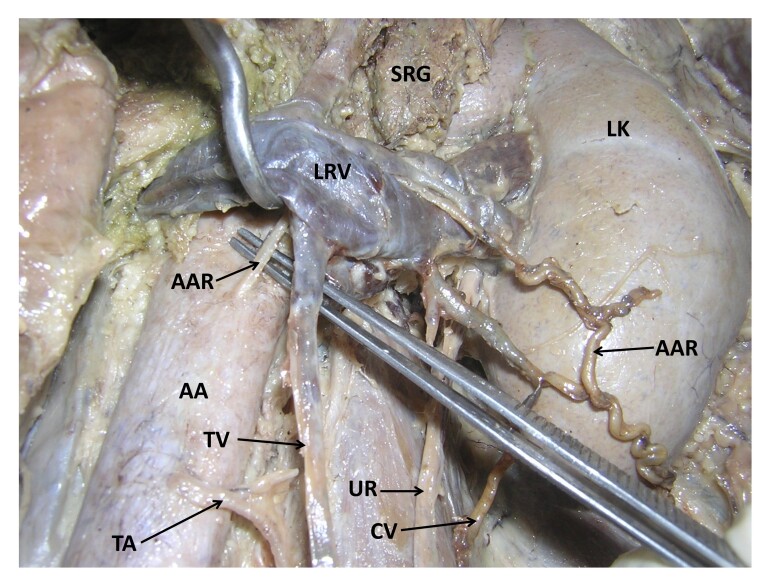 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTattoo and Body Piercing Complications
INTRODUCTION
The abdominal aorta is the continuation of the thoracic aorta. It extends from vertebrae T12 to L4, where it divides, forming the left and right common iliac arteries. It serves as the main arterial trunk that supplies all the abdominal organs, abdominal walls, lower limbs, and genital organs. The branches of the aorta exhibit a wide range of variations and these variations are well documented in the literature.^1,2^
Renal veins are the major tributaries of the inferior vena cava. The right renal vein drains the venous blood from the right kidney, whereas the left renal vein collects the venous blood from the left suprarenal gland, left gonad, and left kidney. The testicular arteries usually arise from the anterior aspect of the abdominal aorta at the level of the second lumbar vertebra, a little below the origin of the renal arteries. Each of them runs downwards behind the parietal peritoneum before entering the inguinal canal. The right testicular artery crosses the anterior surface of the inferior vena cava. As variants, the testicular artery may originate from the renal artery, suprarenal artery, or lumbar artery.^3^ The testicular arteries are accompanied by the testicular veins. These are formed by the pampiniform plexus, which is formed by the union of small veins from the testis and epididymis. The testicular arteries show variations in 4.7% of people. These variations are mainly described as high origin from the aorta or origin from the renal artery.^4^ This case reports presents a rare anomalous lateral branch of the abdominal aorta. We would like to alert radiologists, nephrologists, and surgeons in general about this artery, which could cause iatrogenic injuries or confusion during radiologic interpretation.
Ethics committee clearance was obtained for this study. It complies with the Helsinki Declaration and with local ethical guidelines. We have obtained all appropriate consent forms and ethics committee clearance for the use of cadavers in this study. No patient data were used in the study.
CASE REPORT
During regular dissection classes, we found some vascular variations in relation to the left kidney in an adult male cadaver aged approximately 70 years. The left kidney was fed by renal vessels which had their normal origin, course, and termination. Moreover, the abdominal aorta gave off almost all of its branches at normal levels. However, an additional, anomalous artery took origin from the anterior surface of the aorta behind the left renal vein and pierced the left renal vein (Figures 1 and 2). After piercing the left renal vein, it traced a tortuous course through the peri-renal fat pad in front of the lower part of the left kidney. The artery then ran downward and laterally, pierced the anterior layer of thoracolumbar fascia, and continued to the posterior abdominal wall to supply its muscles. It also supplied the fat and fasciae around the kidney. This anomalous artery was accompanied by a vein, which opened into the left renal vein close to the hilum of the kidney. There was also a communicating vein, which connected the left testicular vein to the vein accompanying the anonymous artery. The left testicular artery had a slightly low origin from the anterior surface of the aorta, possibly because the anomalous artery took origin from the aorta at the level of the origin of the testicular artery. The upper four lumbar arteries had normal origins from the dorsal surface of the aorta. Their course and distribution were also normal.
Dissection of the upper left part of the abdomen showing the kidney and its vessels. SRG: left suprarenal gland; LK: left kidney; AAR: anomalous artery; LRV: left renal vein; AA: abdominal aorta; TV: testicular vein; TA: testicular artery; UR: left ureter; CV: communicating vein.
Closer view of the anomalous lateral branch of the abdominal aorta. SRG: left suprarenal gland; LK: left kidney; LRV: left renal vein; AAR: anomalous artery; AA: abdominal aorta; TV: testicular vein; TA: testicular artery; UR: left ureter; CV: communicating vein.
DISCUSSION
Knowledge of variations involving the blood vessels of the abdomen is important for surgeons during operative and endovascular procedures. Variations in the branches of the abdominal aorta are commonly observed during diagnostic angiography, surgeries, or cadaveric dissection. Among these, the most reported involve the hepatic artery, renal artery, celiac trunk and its branches, suprarenal arteries, or gonadal arteries. In the present case, we observed a novel anomalous lateral branch that arose from the abdominal aorta. Previous reports describing anomalous left testicular arteries include a rare case of a left testicular artery getting entrapped between the two divisions of the left renal vein.^5^ The point of origin of the anomalous lateral branch in the current case is almost the same as the above case, but the area of distribution and relationship to the renal veins are totally different.
Variations of the testicular arteries are common and have been well-documented. The testicular arteries may vary at their origin, they may be missing, or one or both arteries may arise from the renal artery, suprarenal artery, or lumbar artery. They may also arise from a common trunk or be doubled, tripled, or quadrupled.^6^ Ravery et al.^7^ reported an anomalous origin and described the surgical importance of a testicular artery emerging from the inferior polar artery of the kidney. A high origin of a testicular artery can be the cause of hemodynamic insufficiency involving kidney and testis. Decreased blood flow may lead to varicocele and testicular atrophy.^8^ Cases of high origin of testicular arteries have been reported previously. However, a low testicular artery origin is seldom reported in the literature. In the present case, the left testicular artery had a slightly low origin from the anterior surface of the aorta.
Various morphological anomalies of the testicular arteries hold tremendous clinical relevance due to their influence on normal functioning of the testis and development of many new surgical techniques within the abdominal cavity.^9^ The gonadal vessels must be preserved to avoid possible complications following damage to these vessels.
Variations of renal veins are common. Bandopadhyay and Saha have reported a case of the left renal vein receiving an additional tributary coming from the posterior abdominal wall. This tributary was hooking the left testicular artery.^10^ It is not uncommon for a lumbar vein to join the left renal vein. In a study by Baniel et al., a lumbar vein ending in the left renal vein was documented in 43% of cases.^11^
Variations involving testicular veins are also common. Incidents of variations of the left testicular vein are more common than those involving the right testicular vein. Asala et al.^12^, reported testicular vein variations in 21.3% of cadavers. In a study conducted by Favorito et al.^13^, variation of the number of right testicular veins was found in 15% of specimens and variations in the number of left testicular veins were observed in 18% of specimens. A case of low origin of the testicular artery with an arteriovenous communication between the left testicular artery and the left testicular vein has also been reported.^14^ Yılmaz et al.^15^ present a case of left renal vein fenestration in which a high origin testicular artery passed through it.
In the current case, an anomalous lateral branch was accompanied by a vein, which opened into the left renal vein. There was also a communicating vein, which connected the left testicular vein to the vein accompanying the anonymous artery.
Embryologically, the testis develops at the thoraco-abdominal junction, retroperitoneally, and later descends to the scrotum. At the same time, the kidney develops at the pelvic cavity and ascends to the upper abdomen. One main difference in the descent of the testis and ascent of the kidney is that the kidney is supplied by different arteries at different levels as it ascends. But the testis is supplied by one artery which is dragged all the way to the scrotum. In the current case, it is possible that the testis also had an artery which was supplying it when it was in the upper part of the abdomen and later was divorced when the testis descended to a lower level. The divorced upper testicular artery later would have crossed the kidney and supplied the abdominal muscles. Its origin and course passing through the renal vein make us think along these lines.
To the best of our knowledge, this is a unique variation, and a similar variation has not been reported previously. Functionally, these vessels might not have much significance as there are lumbar arteries to supply the posterior abdominal wall, but surgically they are of great significance. Knowledge of such cases has great importance in an abdominal operation or invasive arterial procedure. The anomalous lateral branch and the accompanying vein could bleed significantly in renal transplant surgeries or any other procedures in the perirenal area.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Minn RMH Last’s anatomy: regional and applied.8th London Churchill Livingstone 1990
- 2Murray A Meguid EA Anatomical variation in the branching pattern of the aortic arch: a literature review Ir J Med Sci 202319241807181710.1007/s 11845-022-03196-336272028 PMC 10390593 · doi ↗ · pubmed ↗
- 3Standring S Gray’s Anatomy: the anatomical basis of clinical practice.41th Philadelphia Elsevier 2016
- 4Pai MM Vadgaonkar R Rai R et al A cadaveric study of the testicular artery in the south Indian population Singapore Med J 200849755155518695863 · pubmed ↗
- 5Nayak SB Abnormal course of left testicular artery in relation to an abnormal left renal vein: A case report Kathmandu Univ Med J 20075110810918603997 · pubmed ↗
- 6Bergman RA Cassell MD Sahinoglu K Heidger PM Jr Human doubled renal and testicular arteries Anat Anz 1992174431331510.1016/S 0940-9602(11)80292-X 1416060 · doi ↗ · pubmed ↗
- 7Ravery V Cussenot O Desgrandchamps F et al Variations in arterial blood supply and the risk of hemorrhage during percutaneous treatment of lesions of the pelviureteral junction obstruction: report of a case of testicular artery arising from an inferior polar renal artery Surg Radiol Anat 199315435535910.1007/BF 016278928128346 · doi ↗ · pubmed ↗
- 8Notkovich H Variations of the testicular and ovarian arteries in relation to the renal pedicle Surg Gynecol Obstet 1956103448749513360658 · pubmed ↗