Improving continuity of care in Finnish primary health care: Insights from a nationwide qualitative study of primary care physicians
Ulla Mikkonen, Kadri Suija, Tuomas Koskela, Pekka Mäntyselkä, Nina Tusa

TL;DR
This study explores how primary care physicians in Finland suggest improving continuity of care through organizational, practice-level, and digital strategies.
Contribution
The study provides new insights from PCPs on systemic and practical approaches to enhance continuity of care in Finnish primary health care.
Findings
PCPs emphasized organizational factors like health center size and work arrangements as important for COC.
Practice-level autonomy and digital solutions, such as measuring COC data, were highlighted as key improvement areas.
Small, incremental changes can improve COC for individual patients while larger systemic efforts are also needed.
Abstract
Continuity of care (COC) is a core value in general practice. It has been deteriorating in Finnish primary health care, but there are now attempts to improve it. This study focused on gathering insights of primary care physicians (PCPs) on how COC can be improved within Finnish primary health care. We conducted a nationwide survey targeting all PCPs working in primary health care. A web-based questionnaire was sent to PCPs in Finland from May to October of 2023. The questionnaire included the question ‘How would you improve continuity of care in your workplace?’ Data were analysed using a descriptive approach that involved iterative and inductive thematic analysis. We received a total of 291 responses from PCPs across Finland (7% response rate). We identified themes related to organisation (e.g. arrangement of practical work including the size of a health centre), practice-level…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
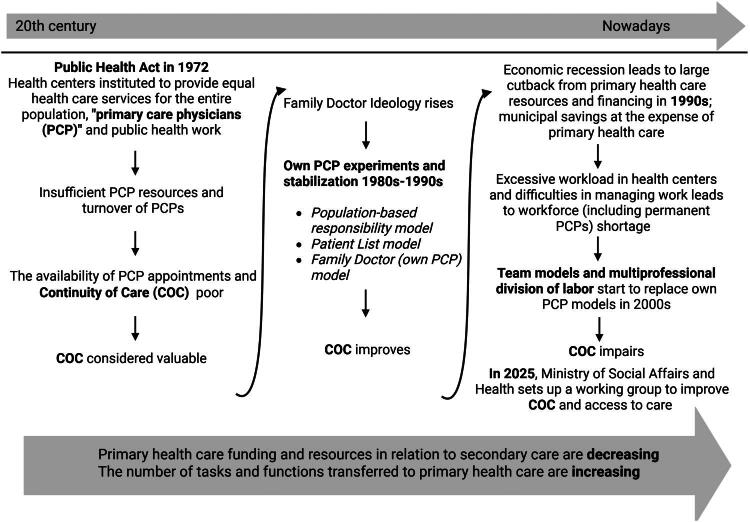 Figure 1
Figure 1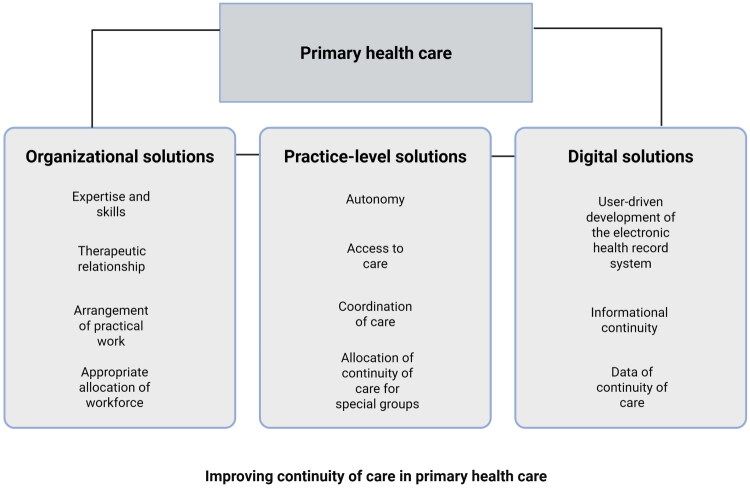 Figure 2
Figure 2| N (%) | |
|---|---|
|
| 291 (100) |
|
| |
| Less than 1 year | 6 (2) |
| 1–5 years | 60 (21) |
| Over 5 years | 225 (77) |
|
| |
| GP specialist | 189 (65) |
| GP trainee | 70 (24) |
| Specialist in other speciality | 6 (2) |
| Trainee in other speciality | 3 (1) |
| Physician in specific training phase | 12 (4) |
| Other physician | 11 (4) |
|
| |
| Southern-Finland | 76 (26) |
| Eastern-Finland | 87 (30) |
| Northern-Finland | 28 (10) |
| Inner-Finland | 56 (19) |
| Western-Finland | 39 (13) |
| Other | 5 (2) |
|
| |
| Less than four physicians | 37 (12) |
| 5–10 physicians | 57 (20) |
| More than 10 physicians | 196 (68) |
| Level | Main theme | Subthemes | Quotation examples |
|---|---|---|---|
| Organisational solutions | Therapeutic relationship |
Relational continuity is considered in policy making Enabling patient-centred care | |
| Expertise and skills |
Physicians’ level of training and professional experience is considered in the division of tasks Training for health care professionals of the assessment of patient’s need for services | ||
| Appropriate allocation of workforce |
Rational use of resources Supplementary services Collaborative and integrated services | ||
| Arrangement of practical work |
Different models to arrange patient care (team-based, own PCP etc.) Size of health centre | ||
| Practice-level solutions | Autonomy |
Opportunity to perform continuity of care in daily work Possibility to resolve practical issues locally | |
| Access to care |
Assessing the patient’s care needs by familiar professionals The patient’s own PCP helps to assess the care needs Patients are always referred to their own PCP PCP can book further consultations directly at themselves Using electronic invitation system to organise proactive and systematic care of/for chronic diseases | ||
| Allocation of continuity of care for special groups |
Identification of people who are multimorbid or overuse healthcare | ||
| Coordination of care |
Remote consultations are referred to the one’s own GP Care pathways and common practices support continuity of care | ||
| Digital solutions | User-driven development of the electronic health record system |
The same electronic health record system for all care providers Electronic health record systems support continuity of care | |
| Information continuity |
Conjointly updated medication lists, care plans, treatment goals and functional capacity recorded and available Digital tools serving and supporting continuity of care | ||
| Data of continuity of care |
Measuring continuity of care Shared information, goal and engagement to improve continuity of care |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPrimary Care and Health Outcomes · Chronic Disease Management Strategies · Diabetes Management and Education
Introduction
Continuity of care (COC) is a core value in general practice [1]. Furthermore, the scientific evidence supporting the implementation of COC in general practice is strong [2–7]. COC is commonly defined in terms of relational, informational, and management COC [8,9]. While the knowledge of the benefits of COC for patients, health care professionals, and health care system is well-established [3–6,10,11], COC has declined in the Finnish health care system. National statistics also indicate a marked decline in COC in recent years [12]. This may be due to the prioritisation of access to care and the reduction of resources at the expense of COC [13].
Changes are taking place in the provision of primary health care worldwide; the expectations of patients and employees are diverse; and digitalisation is expanding in various ways. Efforts to improve system productivity—such as enhancing digital infrastructure—coincide with patient-related factors like complex illnesses and diverse needs, as well as financial challenges. Together with cost-saving pressures, these factors make it increasingly demanding to deliver care that is accessible, patient-centered, and equitable. In a system struggling with burnout, it is challenging to carry out and maintain care in accordance with the core values of general practice that emphasise continuity of doctor-patient relationships as a central organising principle [14]. The primary health care system in Finland has undergone significant changes (Figure 1) that compromise the ability to maintain COC [13,15]. Finnish public health care is primarily tax-funded. The public sector both finances and provides most services. Adult patients pay service fees, but these are capped annually. Primary care physicians (PCPs) at a health centre typically receive either a fixed salary or a combination of base pay and performance-based compensation, but there are no specific incentives for ordering blood tests or other diagnostic procedures.
A rough description of the phases of continuity of care in Finnish primary health care. The figure is constructed based on [13].
Only a limited number of studies have investigated the perspectives of PCPs on how to improve COC in current primary health care. In a qualitative study in the Netherlands, the staff and patients perceived relational COC as existing more between a patient and the entire general practice team than between the patient and their own PCP. Thus, improving COC was associated, for example, with effective team communication and staff stability [16]. In another qualitative study from the Netherlands, PCPs identified numerous areas for development in their daily practice, such as increasing time per consultations, supporting small-scale practices, or delegating tasks to allow regular PCPs more time for complex cases [17]. A qualitative study of patients in Spain described health-system-related (e.g. assignment to a personal PCP), organisation-related (e.g. size of a health centre) and doctor-related elements (e.g. commitment to patient care) that contributed to relational COC [18].
A gap remains in understanding health care professionals’ perspectives on actionable strategies to enhance COC. In this study, we aimed to explore the views of PCPs on ways to improve COC within Finnish primary health care.
Methods
This study was part of a research project titled Good Practices in Primary Health Care [19]. The aim of the project was to describe existing good practices in primary health care and views of PCPs on areas needing development. (Original questionnaire, Supplemental Material S1) The survey was conducted from May to October of 2023. The questionnaire (via Webropol) was targeted at PCPs working in primary health care settings in Finland. In Finnish primary health care, there are specialists in general practice, doctors in residency training, and other non-specialist physicians working in health centres. The invitation was sent by e-mail to the professors of general practice in the universities of Finland and chief physicians across Finland. They disseminated the invitation to PCPs working within their assigned service areas. An invitation and link to the online questionnaire were also shared on a social media platform (Facebook group) used by PCPs. Participation was voluntary.
The survey was completed without identifiable personal data. We collected quantitative data of the respondents as follows: working area, work experience in primary health care, specialist training phase, and number of PCPs in their health centre. We described these as counts and percentages. This study focused on responses to the open-ended question: ‘How would you improve COC in your workplace?’
Data analysis
We used a qualitative descriptive approach employing inductive, thematic analysis [20] as the method for analysing the data. The researchers (n = 5) independently familiarised themselves with the data. All of them identified codes independently (manually/Atlas.ti) without a previously defined codebook or theoretical framework. Then the codes were discussed together. Next, two researchers (UM, NT) grouped the codes that shared the same meaning and drafted an initial thematic map of themes. The study group had several meetings in which the initial thematic map was discussed with the entire research group. During the process, themes were repeatedly compared to the original material to ensure that they reflected it. We found that the main themes discovered in the answers given by PCPs fall under the following categories: organisational, practice-level, and digital solutions. All the researchers involved agreed on the themes. Finally, we revisited the original material using the codes and compared the emerging themes with the overall message of the data. Some selected responses from the original material were then chosen as illustrative quotations. The study was reported in accordance with the Standards for reporting qualitative research [21]. During the analysis, the members of the group included a doctoral researcher (UM), educational chief physician and researcher (NT), associate professors of general practice (KS, TK) and professor of general practice (PM). All were PCPs and had expertise in qualitative research. Having regular discussions with our team of researchers helped to increase reflexivity and reduce unconscious bias.
Results
Study sample
We received a total of 291 responses (ranging from short to long answers with various examples, with the data consisting of 6,035 words in total) to the question on improving COC from PCPs across primary health care centres in Finland (Table 1). There are approximately 4,000 vacancies in public primary health care centres across Finland, with an average response rate of 7%.
The themes are illustrated in Figure 2 under organisational, practice-level, and digital solutions. Table 2 presents the main themes (n = 11) and subthemes (n = 25) with some illustrative quotes. Every quotation is followed by an indication of whether the respondent was a specialist in general practice (S), resident doctor (R), or other PCP (A) as well as years of working experience in primary health care. The following sections describe the results of each main theme.
Main themes (n = 11) and categories (organisational, practice-level and digital) of improving continuity of care as reported by primary care physicians in Finland.
Therapeutic relationship
PCPs mentioned that policymakers should understand the importance of COC in decision-making and its importance for patients’ treatment results. Preserving patients’ ability to choose their own PCP was considered important.
Expertise and skills
PCPs stated that a physician’s level of training and work experience should be considered when allocating tasks and responsibilities. The number of experienced PCPs performing patient work was seen as important, and the respondents felt that it is not reasonable to assign a patient population to a physician who is doing a brief period of work. Instead, they should jointly take care of the same population with a specialist in general practice. COC was seen as producing valuable information for resident doctors regarding their work quality and learning.
Appropriate allocation of workforce
For PCPs, the rational use of resources means that each professional group performs tasks aligned with its specific expertise and level of education. The workforce of experienced PCPs was seen as important for maintaining longitudinal care relationships in clinical practice.
Health services that complement public health care (supplementary services), such as occupational health care or outsourcing service providers, should take care of the patient’s entire care process without fragmentation of care. Similarly, remote consultations should support COC.
Collaboration between different occupational groups and care providers, as well as between social welfare and health care, should be promoted. Organisational structures should enable the comprehensive, rather than siloed, care of the patient.
Arrangement of practical work
PCPs called for sufficient resources. The respondents identified different models to organise longitudinal therapeutic relationships, such as the patient’s own PCP-based model, a team-based model, or a model involving a pair of an experienced PCP (specialist in general practice) and a resident doctor. The small size of a health centre was seen as a factor that promoted familiarity between patients and health centre staff. They also proposed that a substitute should be appointed during PCPs’ holidays.
Autonomy
Autonomy was described by PCPs as managing one’s own schedule and having enough discretionary time to provide consultations based on the needs of their own population. Autonomy also included the opportunity for those engaged in practical work to participate in planning and organising their daily tasks. Furthermore, they should have assigned work time for development tasks.
Access to care
PCPs stated that the assessment of care needs should be carried out by professionals who are already familiar with the patients and population. To assess whether an appointment is required for the patient, or whether the problem can be resolved in an alternative manner, consultation with the patient’s own PCP is recommended. An electronic invitation system could be used to organise the treatment of long-term diseases timely and to refer patients to their own PCP.
Allocation of COC for special groups
PCPs recognised that at least multimorbid patients and high health care utilisers should have their own PCP or case manager. However, patient allocation should be coordinated in order to prevent excessive workload on individual PCPs. Respondents also felt that more knowledge is still needed regarding patients who do not benefit from continuity.
Coordination of care
Interprofessional consultation in patient care should be easy to implement and seamlessly integrated into daily practice. Remote and digital consultations, like other forms of patient care, should be applied appropriately to ensure quality and effectiveness. Common care paths and practices support the smoothest possible care.
User-driven development of the electronic health record system (EHRS)
PCPs proposed an EHRS that could identify and recommend a PCP/responsible employee when the patient schedules an appointment. When a patient renews a prescription, the system would alert them if annual check-ups have not been completed. The system should send an alert if the patient has poor control of long-term conditions or risks identified in the course of primary prevention.
Informational continuity
PCPs considered important that primary and secondary care staff update patients’ medication lists, care plans and treatment goals, along with a description of their functional capacity in the EHRS so that these data are available for all involved in the care process. PCPs suggested that digital tools could be used for supporting relational COC and collecting preliminary data before an appointment (questionnaires, health behaviours etc.).
Data of COC
Respondents considered it important that COC be set as a shared goal in health care. COC should be measured regularly, and information should be available to employees to get feedback on the quality of their work.
Discussion
Main findings
PCPs identified several elements that support COC in primary health care. Enhancing COC for a broad patient population requires a systemic perspective and structured, goal-oriented development efforts such as enhancing sufficient resources in primary health care, using the workforce appropriately, preserving PCPs’ autonomy in managing their daily work, and improving collaborative and integrated services. However, multiple small, discrete actions such as updating medication lists, referring patients to their own PCP or using an electronic invitation system to organise follow-up care for long-term conditions could also improve COC for individual patients.
Comparison with existing literature
Based on our results, it is crucial to maintain sufficient resources in primary health care, taking into account holiday and training periods of permanent staff. A recent analysis considered organisational aspects in implementing COC in the UK. The authors stated that to increase COC, the whole practice should be committed to the project. A shared goal should be targeted and measured. As a result, health care professionals and patients receive feedback on the potential benefits. If not properly managed, responsibility may shift to individual professionals, leading to a decline in COC [22]. PCPs in our study also perceived that COC should be measured and this information utilised in day-to-day management.
In our study, solutions to improve access to care such as the centralisation of services into large-scale units and the implementation of team-based models—both of which have been proposed to address the shortage of health care personnel in Finland—were found to pose challenges for COC. Interestingly, another study suggested that team-based care might provide the means to maintain relational COC. However, the authors also felt that enabling this would likely require that teams remain small and consist of stable personnel, and it is essential to consider how tasks are distributed among different professional groups [16]. The PCPs in our study emphasised the importance of preserving the ability to flexibly adjust daily operations at the local level. Development of COC in the system requires joint dialogue, goal setting and follow-up monitoring at the local level [23].
In Finland, participation in specialist medical training contributes to turnover within the primary care workforce. All specialising doctors are required to work in primary health care for varying mandatory periods. Thus, the resources of PCPs will continue to be variable and pose challenges to relational COC in the future. Earlier proposals have suggested a pair of PCPs working together to ensure relational COC [16]. Similarly, our data suggest that relational COC could be distributed within smaller teams, such as pairing a specialist with a resident physician to jointly manage care. In addition, the number of part-time PCPs is increasing. However, there is also some evidence that clinic-specific COC (seeing own PCP or if not available, another PCP in the same clinic) is associated with less use of emergency services or need for hospital care [24].
One aspect in developing COC is the preferences of patients. Some prefer fast access to care instead of COC. This preference may also vary for the same individual depending on the problem for which they are seeking help [25]. In our study, the PCPs also discussed which patients should be targeted for COC, which is in line with previous qualitative studies [16,26]. However, it is important to remember that the individuals who would benefit most from COC or services do not always ask for or receive them [27].
In our study, PCPs proposed multiple digital solutions that could improve COC. In a qualitative study in Belgium, shared health records were perceived as supporting interprofessional team work in general practice [28]. In another study, respondents also noted that more effective use of EHRS could improve informational COC in team communication [16]. In addition, the EHRS could aid staff in scheduling appointments with the same PCP [17]. By improving informational and management COC, it may be possible to partially offset the disadvantages of a disrupted relational COC [5]. A recent Finnish study suggested that doctors can experience stress when digital systems do not support their work [29]. Well-functioning systems can support informational COC as well as the comfort and retention of doctors, and thus COC.
Efforts have been made in Finland to resolve the dilemma between the need, demand, and availability of services in different ways, such as by increasing multiprofessional team-based work. Maintenance of everyday clinical work solutions that support COC requires that staff perceive it as an important and shared goal. When the staff is volatile and there is also a widespread shortage of PCPs in Europe [30], it is important to find new solutions to maintain the core values of general practice in clinical practice. However, the implementation of new clinical practices requires time as well as adequate support structures and sufficient resources [26]. In summary, the clinical practice proposals presented in this study demonstrate an appreciation of functional teamwork to provide patients with a seamless and appropriate care pathway.
Strengths and limitations
The study produced perspectives for improving COC. The responses were mainly from specialists in general practice or junior doctors in residency training in general practice, offering a rich and diverse perspective. Responses were from all areas of Finland. In addition, most of them had extensive working experience in primary health care. The respondents produced a wealth of answers to open-ended questions, which indicates the importance of the topic for them. A strength of the study was the use of several methods to share the invitation link.
Answers to the open-ended questions were received in written form and some of them were short. It was not possible to make a specific interpretation of the answers from the respondents, and the authors’ background factors may have had an impact on interpretation. In this study, doctors willing to participate might hold different views from those who did not. However, the answers of the respondents probably reflect the Finnish health care context. The questionnaire did not specify COC in more detail, which may have influenced the responses. We did not want to focus on just one part of COC, as its dimensions are interconnected.
Implications for practice and policy
The results contain internationally relevant information, even though health care systems vary. The key question is how to implement these practices. Based on the results, leadership and vision at the organisational level play a key role. Unfortunately, in large organisations, which are common in Finland, the day-to-day management is sometimes handled at a higher level, making it difficult to make changes at the practical level or improve day-to-day operations. Our study highlights the importance of aligning daily work and system management with the practical work environment, alongside shared goal setting, continuous monitoring, and timely feedback.
In conclusion
Health care is undergoing continuous transformation, necessitating the parallel development of strategies to maintain COC within this evolving landscape. Involving practitioners in the development process is essential, as their firsthand experience provides valuable insight into the operational environment. Such collaboration ensures that the resulting practices remain relevant and applicable, even amid systemic changes. Enhancing COC should not be viewed as an isolated initiative but rather as an integral component of strengthening the primary health care system as a whole.
Supplementary Material
Supplemental Material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nordic Federation of General Practice (NFGP). Core Values and Principles of Nordic General Practice/Family Medicine. Scand J Prim Health Care. 2020;38(4):367–368. doi:10.1080/02813432.2020.1842674.33284030 PMC 7782180 · doi ↗ · pubmed ↗
- 2Kajaria-Montag H, Scholtes S, Gray DP, et al. Continuity and locum use for acute consultations: observational study of subsequent workload. Br J Gen Pract. 2025;75(752):e 181–6–e 186. doi:10.3399/BJGP.2024.0312.39870531 PMC 11800408 · doi ↗ · pubmed ↗
- 3Hetlevik Ø, Holmås TH, Monstad K. Continuity of care, measurement and association with hospital admission and mortality: a registry-based longitudinal cohort study. BMJ Open. 2021;11(12):e 051958. doi:10.1136/bmjopen-2021-051958.PMC 864063434857569 · doi ↗ · pubmed ↗
- 4Nowak DA, Sheikhan NY, Naidu SC, et al. Why does continuity of care with family doctors matter? Review and qualitative synthesis of patient and physician perspectives. Can Fam Physician. 2021;67(9):679–688. doi:10.46747/cfp.6709679.34521712 PMC 9683367 · doi ↗ · pubmed ↗
- 5Pahlavanyali S, Hetlevik Ø, Baste V, et al. Continuity and breaches in GP care and their associations with mortality for patients with chronic disease: an observational study using Norwegian registry data. Br J Gen Pract. 2024;74(742):e 347–54–e 354. doi:10.3399/BJGP.2023.0211.38621803 PMC 11044022 · doi ↗ · pubmed ↗
- 6Pereira Gray DJ, Sidaway-Lee K, White E, et al. Continuity of care with doctors-a matter of life and death? A systematic review of continuity of care and mortality. BMJ Open. 2018;8(6):e 021161. doi:10.1136/bmjopen-2017-021161.PMC 604258329959146 · doi ↗ · pubmed ↗
- 7Engström SG, André M, Arvidsson E, et al. Personal GP continuity improves healthcare outcomes in primary care populations: a systematic review. Br J Gen Pract. 2025;75(757):e 518–25–e 525. doi:10.3399/BJGP.2024.0568.40355250 PMC 12729051 · doi ↗ · pubmed ↗
- 8Gulliford M, Naithani S, Morgan M. What is ‘continuity of care’? J Health Serv Res Policy. 2006;11(4):248–250. doi:10.1258/135581906778476490.17018200 · doi ↗ · pubmed ↗