Pattern of Independent Factors Influencing Preterm Infants' Chance of Survival to Discharge Without Any Significant Morbidities
Anna Petrova, Rajeev Mehta

TL;DR
The study identifies factors affecting preterm infants' survival without major health issues, such as extreme prematurity and mechanical ventilation.
Contribution
The paper presents novel predictors of survival without bronchopulmonary dysplasia, intraventricular hemorrhage, and retinopathy of prematurity in preterm infants.
Findings
Extreme prematurity (22-27 weeks) decreases the chance of survival without BPD, IVH, and ROP.
Mechanical ventilation and thrombocytopenia are significant predictors of poor outcomes in preterm infants.
Maternal pre-eclampsia increases the likelihood of survival without major morbidities.
Abstract
Background Recognizing the factors that contribute to significant morbidity in preterm infants is essential for effective clinical management and parental counseling. However, current knowledge in this area remains limited. Methods This retrospective single-center study aimed to identify the predictors of bronchopulmonary dysplasia (BPD), intraventricular hemorrhage (IVH), and retinopathy of prematurity (ROP) in surviving infants born between 22 and 32 weeks of gestation. Of the 443 infants studied, 269 did not have any of these conditions, while 174 had at least one. Among the latter group, 110 infants had one, and 64 had more than one disease. We conducted group-based comparisons of 33 maternal, intrapartum, and neonatal factors, which helped identify 15 potentially significant predictors. These were included in regression models to identify those that predicted survival without…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
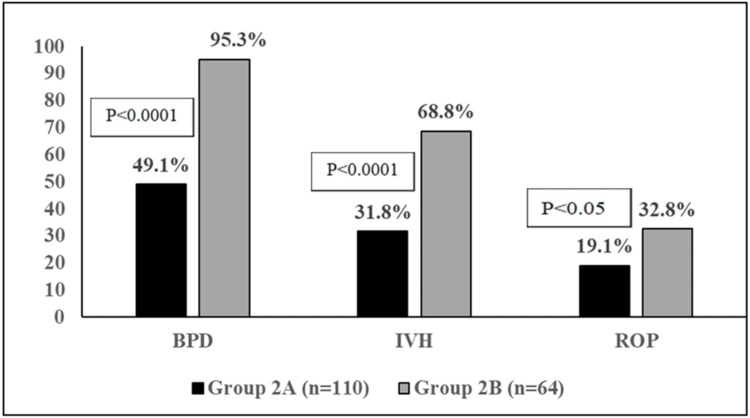 Figure 1
Figure 1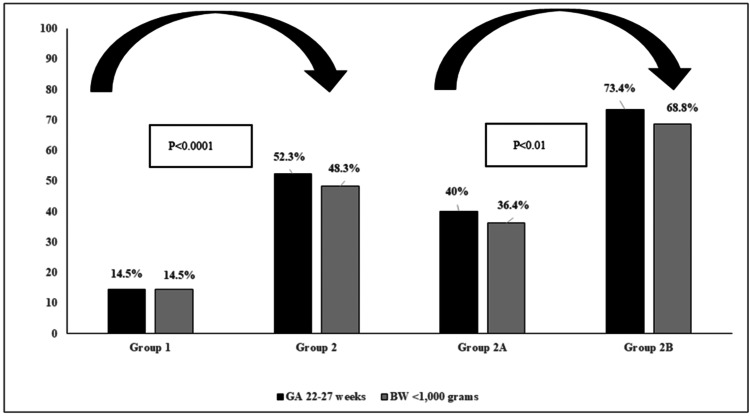 Figure 2
Figure 2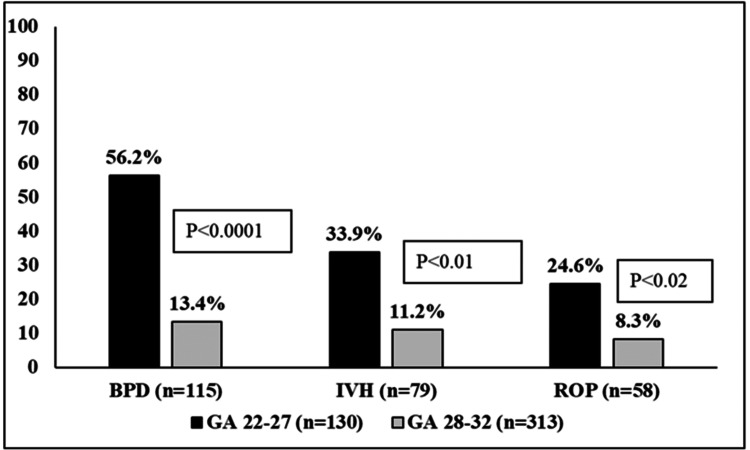 Figure 3
Figure 3| Factors | Group 1 (N=269) | Group 2 (N=174) | Group 2A (N=110) | Group 2B (N=64) |
| GA (M+/-SD, wks) | 29.6 +/- 1.9 | 27.2 +/- 2.4*** | 27.9 +/- 2.3*** | 26.0 +/- 2.2*** |
| BW (M+/-SD, g) | 1371 +/- 377 | 1044 +/- 353*** | 1137 +/- 346*** | 887 +/- 309*** |
| Male sex | 50.4% (135/268) | 48.0% (82/171) | 46.8% (51/109) | 50.0% (31/62) |
| Maternal age >35 y | 22.4% (64/262) | 22.2% (38/171) | 25.5% (28/110) | 16.4% (10/61) |
| White race | 33.2% (84/268) | 38.5% (67/174) | 44.6% (49/110) | 28.2% (18/64) |
| Medicaid/uninsured | 46.6% (124/266) | 45.1% (78/173) | 40.4% (44/109) | 53.1% (34/64) |
| No prenatal care | 4.5% (12/269) | 4.0% (7/174) | 3.6% (4/110) | 4.7% (3/64) |
| Drug use | 4.1% (11/269) | 2.9% (5/174) | 2.7% (3/110) | 3.1% (2/64) |
| Any chronic illness | 36.1% (97/269) | 32.2% (56/174) | 32.7% (36/110) | 31.3% (20/64) |
| PIH/hypertension | 15.2% (41/269) | 14.5% (26/174) | 14.6% (16/110) | 15.6% (10/60) |
| Maternal infection | 5.6% (15/269) | 5.8% (10/174) | 7.3% (8/110) | 3/1% (2/64) |
| Breech presentation | 21.6% (58/268) | 21.8% (38/174) | 20.0% (22/110) | 25.0% (16/64) |
| Placental pathology | 11.2% (30/269) | 13.8 (24/174) | 13.6% (15/110) | 14.1% (9/64) |
| Preeclampsia | 24.9% (67/269) | 12.1% (21/174)*** | 13.6% (15/110)* | 9.4% (6/64)** |
| PPROM | 40.2% (107/266) | 42.9% (73/170) | 43.5% (47/108) | 41.9% (26/62) |
| Antenatal steroids | 84.9% (225/265) | 82.6% (142/172) | 82.6% (90/109) | 82.5% (52/63) |
| Antenatal antibiotics | 43.8% (113/258) | 54.2% (90/166)* | 55.7% (59/106)* | 51.7% (31/60) |
| Multiple gestations | 28.6% (77/269) | 23.0% (40/174) | 23.6% (26/110) | 21.9% (14/64) |
| Abnormal FHR | 13.8% (37/269) | 9.8% (17/174) | 9.1% (10/110) | 10.9% (7/64) |
| Cesarean section | 68.6% (181/264) | 67.1 (114/170) | 70.4% (76/108) | 61.3% (38/62) |
| Apgar at 1 min <3 | 24.9% (67/269) | 12.1% (21/174)*** | 13.6% (15/110)* | 12.7% (8/63)* |
| Apgar at 5 min <5 | 3.4% (9/267) | 8.1% (14/173)* | 5.5% (6/110) | 12.7% (8/63)** |
| SGA | 9.3% (25/268) | 9.3% (16/173) | 10.1% (11/109) | 7.8% (5/64) |
| Intubation at birth | 29.8% (79/265) | 66.3% (114/172)*** | 61.1% (66/108)*** | 75.0% (48/64)*** |
| Surfactant use | 34.5% (91/264) | 66.5% (115.173)*** | 61.5% (67/109)*** | 75.0% (48/64)*** |
| Dexamethasone | 5.7% (15/264) | 28.2% (48/170)*** | 22.4% (24/107)*** | 38.1% (24/63)*** |
| MV | 31.2% (84/269) | 77.0% (134/174)*** | 69.1% (76/110)*** | 90.6% (58/64)*** |
| CPAP | 87.4% (235/269) | 93.1% (162/174) | 91.8% (101/110) | 95.3% (61/64)* |
| PDA | 21.6% (58/268) | 52.9% (92/174)*** | 46.4% (51/110)*** | 64.1% (41/64)*** |
| Sepsis | 16.0% (43/269) | 32.8% (57/174)*** | 30.0% (33/110)** | 37.5% (24/64)*** |
| Thrombocytopenia | 5.2% (14/268) | 19.5% (34/174)*** | 17.2% (19/110)*** | 12.4% (15/64)*** |
| NEC | 1.1% (3/269) | 9.8% (17/174)*** | 10.0% (11/110)*** | 9.4% (6/64)*** |
| Congenital anomalies | 8.9% (24/269) | 19.0% (33/174)** | 18.2% (20/110)* | 20.3% (13/64)** |
| Factors (Yes (1) vs. No (0)) | Model 1 (G1 (0) vs. G2 (1)) | Model 2 (G1 (0) vs. G2A (1)) | Model 3 (G1 (0) vs. G2B (1)) |
| GA 22-27 | 0.68 (0.48, 0.97) | 1.96 (1.21, 3.18) | |
| BW <1,000 g | |||
| Pre-eclampsia | 1.44 (1.05, 1.97) | ||
| Intrapartum AB | 1.43 (1.10, 1.87) | ||
| Intubation at birth | |||
| Surfactant | |||
| Apgar at 1 min <3 | |||
| Apgar at 5 min <5 | |||
| Congenital anomalies | |||
| DART Protocol | |||
| MV | 0.48 (0.35, 0.98) | 1.68 (1.21, 2.34) | 2.99 (1.75, 5.04) |
| PDA | |||
| Thrombocytopenia | 0.52 (0.35, 0.79) | 1.74 (1.11, 2.75) | 3.22 (1.80, 5.73) |
| Sepsis | 0.74 (0.56, 0.97) | ||
| NEC | 0.28 (0.22, 0.91) | 2.1 (1.01, 4.40) | |
| AUC | 0.82 (0.78, 0.84) | 0.70 (0.61, 0.73) | 0.90 (0.88, 0.93) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeonatal Respiratory Health Research · Infant Development and Preterm Care · Neonatal and fetal brain pathology
Introduction
There has been a significant improvement in survival and rate of morbidities in prematurely born infants [1]. However, infants born at extremely preterm gestation continue to remain at an elevated risk of being diagnosed with at least one major morbidity [2], which negatively impacts their quality of life [3] and increases health expenditure [1,4]. One of the challenges associated with delivery at extremely preterm gestation is predicting the development of significant morbidities in the surviving neonate. A few reports [5-7], inconsistent in their gestational age (GA)-based inclusion criteria, selection of predictor factors, and types of the studied morbidities, have focused on identifying factors beyond GA and birth weight (BW) to predict significant health problems in preterm babies. A large study, which included data from Spain (SENI500) and the Latin American Neonatal Networks (NEOCOSUR), reported a reduced risk of developing intraventricular hemorrhage (IVH grade 3-4), periventricular leukomalacia (PVL), bronchopulmonary dysplasia (BPD), retinopathy of prematurity (ROP), necrotizing enterocolitis (NEC), and late-onset sepsis (LOS) in infants born at a GA of 24 to 30 weeks if they were female, had higher Apgar scores, and were not intubated [5]. Simultaneously, the risk increased for infants born from multiple pregnancies, small for gestational age (SGA), and within the Latin American Network [5]. The Canadian Neonatal Network's study of infants born at a GA of 22-32 weeks highlights a higher probability of surviving without BPD, IVH (grade 3-4), PVL, and ROP for females and those born at advanced GA and BW [6]. A study from California utilized the Statewide Health Planning and Development database to construct resiliency scores for estimating the probability of survival without BPD, NEC, IVH (grades 3-4), PVL, and ROP in infants born at less than 32 weeks [7]. The authors stated that resilience scores predict morbidity in preterm infants more accurately than risk assessments. Unfortunately, the lack of an automated score calculator could restrict adherence if the resilience scores are implemented in neonatal practice [8].
We designed this single-center retrospective study to highlight the importance of predicting significant health challenges in the survival of preterm infants. Our primary goal was to identify whether maternal, intrapartum, and neonatal factors independently predispose to the survival of infants born between 22 and 32 weeks of GA without experiencing any BPD, IVH, and ROP. Our second goal was to explore the factors that predict the diagnosis of one or more of these morbidities. Existing evidence suggests that the number of morbidities is a key factor linked to an increased risk of adverse neurodevelopmental outcomes [9]. To enhance clinical management and empower family education, it is essential to understand the factors that lead to the development of serious preterm morbidities.
Materials and methods
This study utilized a retrospective cohort design that focused on surviving infants with GA less than 33 weeks of completed gestation between January 2007 and January 2016 and admitted to the 37-bed Level III Neonatal Intensive Care Unit (NICU). The study was approved by the Rutgers Robert Wood Johnson Institutional Review Board (ID: 20160000233) on 03/04/2016.
Data characteristics
We used GA as specified by the obstetrician to select neonates from NeoData, a data system designed to assist in the daily patient management of neonates, and a standardized data collection tool to gather the documented maternal, antenatal, and intrapartum variables from the electronic medical records (EMR). Because of the low rates of chronic and maternal infection-related morbidity, we defined categories based on whether at least one morbidity was documented. We categorized maternal age into two groups: 35 years and older or less than 35 years, owing to the heightened risk of adverse fetal conditions associated with advanced maternal age, defined as 35 years and older [10]. We classified BW as extremely low birth weight (ELBW) if the neonate weighed less than 1,000 grams [11] and categorized infants as SGA if their birth weight fell below the 10th percentile for their GA [12]. We defined a low Apgar score as a score of less than three at one minute and less than five at five minutes [13]. Patients with thrombocytopenia were identified if their platelet count was at least once less than 150,000/microL [14]. The diagnosis of sepsis was used if the blood culture or cerebrospinal fluid (CSF) was assessed as positive for bacterial pathogens, and NEC was utilized without considering stage [15].
Definition of morbidities
The primary outcomes were focused on morbidities documented in the EMR: (i) IVH of any grade, including low grade [16], because it is linked with neurodevelopmental impairment in infants born prematurely [17]; (ii) BPD of any grade because of the questionable validity of the existing definitions of this most common preterm birth-related pathology [18,19]; and (iii) ROP, if it was diagnosed and monitored by the NICU ophthalmologist.
Outcome definition
We defined the diagnosis-specific groups of surviving infants as (i) without any IVH, BPD, and ROP (Group 1); (ii) with at least one of these morbidities (Group 2); (iii) with only one of the studied morbidities (Group 2A); and (iv) with more than one morbidity (Group 2B).
Sample size
We calculated the sample size needed to create a binary stepwise logistic regression model to predict survival to discharge without BPD, IVH, and ROP. The formula used was N = 10 * k / p, where N is the total number of infants studied (N=443), 10 is the events per variable (EPV), k is the number of independent variables, and p is the fraction of infants who were discharged without all three studied morbidities (0.614). We estimated that up to 27 independent variables (k) could be included in the model with a sample size of 436 subjects.
Statistical analysis
We identified differences in categorical and continuous variables among neonates in Group 1 vs. Group 2, Group 1 vs. Group 2A, and Group 1 vs. Group 2B using the chi-square test and analysis of variance (ANOVA), and the Mann-Whitney U test for nonparametric variables when necessary. Identified significant factors were incorporated as independent variables in stepwise logistic regression models, using a backward elimination approach for predictors. In Model 1, we focused on the factors predicting survival without any morbidity; in Model 2, we examined survival with one morbidity, and in Model 3, we assessed survival with more than one of the studied morbidities. GA and BW were included in the models as categorical variables (22-27 vs. 28-32 weeks and ELBW vs. >1,000 grams) because the variance inflation factor (VIF) between GA and BW is 1.0. Data are presented as proportions with 95% confidence intervals (95% CI), parametric continuous data as means with 95% CI, and nonparametric data as medians with interquartile ranges (IQR). The outcomes from each model were articulated via odds ratios (OR) with 95% Confidence Intervals (95% CI). Additionally, we employed receiver operating characteristic (ROC) analysis, represented by the area under the curve (AUC), to evaluate the discriminatory power between dependent groups in each model. We used the bootstrap technique to assess the internal validity of the stepwise logistic regression model. The AUC is presented with 95% CI. It was considered acceptable if the AUC was 0.7-0.8, excellent if 0.8-0.9, and outstanding if more than 0.9. P-values at less than 0.05 were considered statistically significant. We used TIBCO Statistica™ 14.01.25, 2020 (TIBCO Software Inc., Palo Alto, California, US). This software facilitates the execution of a wide range of statistical analyses, including regression modeling.
Results
Of the 498 selected infants, 52 who died and three with incomplete birth data were excluded. Of the 443 surviving neonates, 269 (60.7%, 95% CI 56.0%, 65.31%) were free from any IVH, BPD, and ROP (Group 1), while 174 (39.3%, 95% CI 34.7%, 44.0%) were diagnosed with at least one disease (Group 2), including 110 (63.2%, 95% CI 55.6%, 70.4%) with one (Group 2A) and 64 (36.8%, 95% CI 29.6%, 44.4%) with two (n=50) or all three (n=14) morbidities (Group 2B). IVH was recorded in 70 (45.4%, 95% CI 37.9%, 53.1%), BPD in 115 (66.1%, 95% CI 58.5%, 73.1%), and ROP in 58 (33.3%, 95% CI 26.4%, 40.9%) infants.
Figure 1 illustrates the larger proportion of BPD cases and the less frequent diagnosis of IVH and ROP in Groups 2A and 2B.
The proportion of BPD, IVH, and ROP cases in Group 2A and Group 2BBPD: Bronchopulmonary dysplasia; IVH: Intraventricular hemorrhage; ROP: Retinopathy of prematurity; Group 2A: with only one of the studied morbidities; Group 2B: with more than one morbidity.
Disease-specific rates of IVH, BPD, and ROP in the 443 infants studied were 15.8% (95% CI 12.5%, 19.5%), 26.0% (95% CI 22.0%, 30.3%), and 13.1% (95% CI 10.1%, 16.6%), respectively.
GA-based distribution of morbidity and risk factors
Out of the 443 infants in the study, 29.3% (95% CI 25.2%, 33.8%) were extremely preterm (GA 22-27 weeks), and 27.8% (95% CI 23.6%, 32.2%) were born with ELBW (BW<1,000 grams). Figure 2 demonstrates the group-based difference in the proportion of infants born with GA 22-27 weeks and BW <1,000 grams.
Proportion (%) of infants with gestational age (GA) of 22-27 weeks and birth weight (BW) <1,000 grams in the studied groups
These infants were less likely to have a single disease diagnosed than those with more than one of the studied morbidities (P<0.01). Data in Figure 3 shows that IVH, BPD, and ROP rates were three to four times higher in infants born with a GA of 22-27 weeks as compared to those born with a GA of 28-32 weeks.
Rates (%) of BPD, IVH, and ROP in infants born with GA of 22-27 and 28-32 weeksGA: Gestational age; BPD: Bronchopulmonary dysplasia; IVH: Intraventricular hemorrhage; ROP: Retinopathy of prematurity
Group-based comparison of the studied factors is shown in Table 1.
**Table 1: Group-based comparison of maternal, antenatal, and neonatal factorsGA: Gestational age; SGA: Small for Gestational Age; IUGR: Intrauterine Growth Restriction; ELBW: Extremely Low Birth Weight; Maternal chronic morbidity: defined on EMR (diabetes, hypertension, asthma, hyper/hypothyroidism, seizures, coagulopathy, leukemia, and systemic connective diseases); Maternal infection morbidity: defined on EMR (urinary tract infection (UTI), sexually transmitted infection (STI), group B strep (GBS)); PPROM: Preterm premature rupture of membranes; DART: Dexamethasone: A Randomized Trial; FHR: Fetal heart rate; MV: Mechanical Ventilation; CPAP: Continuous Positive Airway Pressure; PDA: Patent Ductus Arteriosus; NEC: Necrotizing Enterocolitis; M: Mean +/-Standard Deviation (SD); *P<0.05-0.02; **P<0.01; *P<0.001.
As shown in Table 1, the demographic characteristics and most antenatal and intrapartum factors were comparable between the study groups. Infants in Group 1 had higher GA and BW than those in Group 2, Group 2A, and Group 2B. The rate of preeclampsia was higher in Group 1 than in Group 2, Group 2A, and Group 2B. A higher proportion of mothers in Group 2 and Group 2A received intrapartum antibiotics than those in Group 1. A higher proportion of infants in Group 1 were born with a one-minute Apgar score <3 than those in Group 2, Group 2A, and Group 2B. However, an Apgar score <5 at five minutes, intubation at birth, use of surfactant, dexamethasone, and mechanical ventilation were more prevalent in Group 2, Group 2A, and Group 2B than in Group 1. Additionally, more infants in Group 2, Group 2A, and Group 2B were diagnosed with PDA, sepsis, mild congenital anomalies, thrombocytopenia, and NEC than in Group 1.
Factors predicting survival without any disease (Group 1), with one (Group 2A), and more than one (Group 2B) preterm birth-related morbidities
Among the 33 factors in the univariate analysis (Table 1), 15 were included in each model (Table 2).
Data from Model 1 showed a reduced likelihood of survival free from IVH, BPD, and ROP if infants who were born at GA 22-27 weeks required mechanical ventilation and were diagnosed with thrombocytopenia, sepsis, or NEC. However, the chance for survival without any of the studied morbidities increased if the mothers of the infants were diagnosed with pre-eclampsia. An AUC of 0.82 was considered very good for distinguishing infants without a diagnosis of IVH, BPD, and ROP from those diagnosed with at least one of these morbidities.
Model 2 demonstrated that infants exposed to intrapartum antibiotics, mechanical ventilation, thrombocytopenia, and NEC were more likely to be diagnosed with one morbidity as compared to infants without any of the studied morbidities. An AUC of 0.70 indicates a good differentiation between cases with one morbidity and those without any morbidities by identifying significant predictors. Furthermore, Model 3 highlighted that birth at GA 22-27 weeks, mechanical ventilation, and diagnosis of thrombocytopenia were the primary predictors for developing more than one disease. An AUC of 0.90 indicated the model's ability to distinguish between infants at risk for survival to discharge with multiple morbidities and those discharged without BPD, IVH, and ROP.
Discussion
In line with our research, more than 60% of infants born before 33 weeks have survived without being diagnosed with IVH, BPD, or ROP, which aligns with other reports showing survival rates without various significant preterm birth-related morbidities in infants born between 24 and 30 weeks [5], 22 and 32 weeks [6], and 23 and 32 weeks [7]. As in those reports, we too have highlighted the primary role of GA in predicting preterm infant survival without significant morbidities, but did not find an independent effect of gender [6], Apgar scores [5], intubation [5], SGA weight, and multiple pregnancies [5].
The regression model revealed an increased likelihood for survival without IVH, BPD, and ROP in infants exposed to maternal pre-eclampsia, a factor not previously studied while defining disease-free survival of preterm infants. Several studies have examined the role of pre-eclampsia in the development of IVH, BPD, and ROP as a single condition. These studies have reported inconsistent findings, such as a decreased risk for IVH [20], BPD [21], and ROP [22]; an increased risk for BPD [23] and ROP [24]; or no effect on the development of BPD [25]. A study [7] aimed at developing a resiliency model for survival of neonates with a GA of less than 32 weeks found that 24.7% of surviving infants without significant morbidities were born to mothers with pre-eclampsia. In contrast, only 10.5% of infants who did not survive were born to mothers with pre-eclampsia. This highlights the importance of further investigation into how pre-eclampsia affects preterm outcomes.
Additionally, our study identified an increased chance of survival without any IVH, BPD, or ROP if the infants had not been placed on mechanical ventilation and were not diagnosed with sepsis, thrombocytopenia, or NEC. Several studies have analyzed the role of these factors in the development of IVH, BPD, and ROP, but not for survival free of all these morbidities in infants born prematurely. It has been shown that the duration of mechanical ventilation increased the risk for ROP development and the prediction of the need for ROP treatment [26]. Animal studies identified mechanical ventilation-associated increased risk of cerebral inflammation and white matter injury in the immature brain [27]. Furthermore, any abnormal platelet levels were identified as a single marker for the development of BPD [28], ROP [29], and IVH [30]. Our previous study [31] found a clear link between the development of IVH and lower GA and thrombocytopenia, regardless of the severity of thrombocytopenia or the postnatal age at which it begins. Culture-proven sepsis, especially when recurrent, was identified as a factor that increased the risk for IVH, BPD, and ROP [23,32,33]. There is also a possible link between NEC and IVH-related neurodevelopmental outcomes [34], ROP [35], and the contribution of the NEC-related gut-lung axis to the pathophysiology of BPD [36].
In this study, we also examined factors predicting the number of morbidities diagnosed in surviving preterm neonates. The diagnosis of a single morbidity was predicted by exposure to intrapartum antibiotics, mechanical ventilation, and the diagnosis of thrombocytopenia or NEC. The relationship between the administration of intrapartum antibiotics and the development of one of the studied morbidities is not yet fully understood. The use of antibacterial therapy was associated with a diagnosis of clinical chorioamnionitis, which was associated with an increased risk for BPD [37] and IVH [38], but meta-analysis has shown that other factors may influence the identified associations. Consequently, the causal relationship between the use of intrapartum antibiotics and the development of BPD and IVH is not definitive. As mentioned earlier, mechanical ventilation, thrombocytopenia, and NEC are significant factors associated with an increased risk for BPD [28,36], IVH [34], and ROP [26,29,35]. Based on the AUC, factors that discern less than 80% of infants with one morbidity from those without any studied disease have limited clinical utility [39]. Mechanical ventilation and thrombocytopenia emerged as powerful predictors for diagnosing multiple morbidities, demonstrating an even more substantial impact than that seen in Model 2, which examined factors related to the development of at least one studied morbidity. In addition, the possibility of the diagnosis of more than one morbidity increased on average by two times for infants born with GA of 22-27 weeks compared to those born with GA of 28-32 weeks. An AUC of 0.90 indicated an excellent level of discrimination for surviving infants diagnosed with more than one morbidity compared to those who survived to discharge free of IVH, BPD, and ROP by extremely preterm gestation, mechanical ventilation, and thrombocytopenia.
Our study findings emphasize the importance of considering multiple factors for further exploration when analyzing the likelihood of diagnosing morbidity related to preterm birth in infants who survive to discharge. In addition to the GA and BW, a better understanding of other independent factors that forecast major preterm birth-related morbidities could be important not only for clinical management but also for parental counseling. Additionally, the study findings open new possibilities for understanding and predicting survival outcomes in preterm infants and provide valuable insights for further research and potential interventions.
Study limitations
The first limitation of the study was its retrospective design, which may introduce selection bias. To mitigate this risk, we selected the study sample from patients admitted to the NICU. We applied strict selection criteria independent of other factors, including GA and survival status. Additionally, we standardized data collection across all participants, regardless of the outcome, to prevent misclassification bias. We also utilized EMRs. This reliable tool provided us with more accurate information, particularly for gathering maternal, intrapartum, and neonatal factors, in contrast to the International Classification of Diseases (ICD), which is known to have a variety of errors in depicting clinical data [40]. The second limitation was the insufficient sample size in Group 2A (n=110) for identifying factors predicting the type of single morbidity (IVH, BPD, or ROP). Moreover, the sample size in Model 3, fell below the critical threshold of 10 EPV, which is likely to significantly undermine the accuracy of the logistic regression coefficient. It is important to emphasize that while EPV values between five and nine may be deemed acceptable, relying on such values carries inherent risks and should not be overlooked in the analysis [41,42]. This highlights the need for further research to explore this area more comprehensively. Lastly, the findings of this study are derived from a single setting. Approximately 70% of the study population involved non-White participants, and around half were on Medicaid or uninsured, which limits the generalizability of the results to broader populations.
Conclusions
The chance for survival to discharge without IVH, BPD, and ROP in immature infants is significantly reduced when they are born at extremely preterm gestations, require mechanical ventilation, or face serious comorbidities such as thrombocytopenia, sepsis, or NEC. Among these, extremely preterm gestation, mechanical ventilation, and thrombocytopenia are the main predictors for the diagnosis of more than one of the studied morbidities, which is of utmost importance in understanding the health outcomes of immature infants. While the defined models reveal either very good or excellent levels of discrimination for the outcomes studied, further research is essential to validate these findings for clinical use.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mortality, in-hospital morbidity, care practices, and 2-year outcomes for extremely preterm infants in the US, 2013-2018 JAMA Bell EF Hintz SR Hansen NI 24826332720223504088810.1001/jama.2021.23580 PMC 8767441 · doi ↗ · pubmed ↗
- 2Resuscitation, survival and morbidity of extremely preterm infants in California 2011-2019 J Perinatol Higgins BV Baer RJ Steurer MA Karvonen KL Oltman SP Jelliffe-Pawlowski LL Rogers EE 2092164420243768980810.1038/s 41372-023-01774-6PMC 10844092 · doi ↗ · pubmed ↗
- 3Health-related quality of life of children born very preterm: a multinational European cohort study Qual Life Res Kim SW Andronis L Seppänen AV 47583220233597659910.1007/s 11136-022-03217-9PMC 9829588 · doi ↗ · pubmed ↗
- 4Burden of comorbidities and healthcare resource utilization among Medicaid-enrolled extremely premature infants J Health Econ Outcomes Res Mowitz ME Gao W Sipsma H Zuckerman P Wong H Ayyagari R Sarda SP 147155920223661929110.36469/001c.38847 PMC 9790150 · doi ↗ · pubmed ↗
- 5Factors associated with survival and survival without major morbidity in very preterm infants in two neonatal networks: SEN 1500 and NEOCOSUR Neonatology García-Muñoz Rodrigo F Fabres J Tapia JL 28929611820213363174910.1159/000513079 · doi ↗ · pubmed ↗
- 6Prediction of survival without morbidity for infants born at under 33 weeks gestational age: a user-friendly graphical tool Arch Dis Child Fetal Neonatal Ed Shah PS Ye XY Synnes A Rouvinez-Bouali N Yee W Lee SK 0597201210.1136/archdischild-2011-30014321900280 · doi ↗ · pubmed ↗
- 7Developing a resiliency model for survival without major morbidity in preterm infants J Perinatol Steurer MA Ryckman KK Baer RJ 4524574320233622098410.1038/s 41372-022-01521-3PMC 10079534 · doi ↗ · pubmed ↗
- 8Automating clinical score calculation within the electronic health record. A feasibility assessment Appl Clin Inform Aakre C Dziadzko M Keegan MT Herasevich V 369380820172840124510.4338/ACI-2016-09-RA-0149 PMC 6241755 · doi ↗ · pubmed ↗