Aortic pseudoaneurysm as a rare complication of purulent pericarditis: case report and literature review
Chun-Yu Yueh, Ming-Li Li, Ching-Feng Wu

TL;DR
A rare case of aortic pseudoaneurysm caused by purulent pericarditis is reported, highlighting the importance of early detection and treatment.
Contribution
This case report adds to the limited literature on aortic pseudoaneurysm as a complication of purulent pericarditis.
Findings
A 46-year-old man developed an aortic pseudoaneurysm following purulent pericarditis caused by MRSA.
The patient was successfully treated with thoracic endovascular aortic repair and patch repair.
The case underscores the need for prompt management of rare but life-threatening complications.
Abstract
Purulent pericarditis has become rare in the antibiotic era, particularly when complicated by secondary infections such as an aortic pseudoaneurysm. We report a 46-year-old man who presented with persistent chest pain and cold sweats for three days. Imaging revealed a large pericardial effusion, and cultures grew methicillin-resistant Staphylococcus aureus(MRSA). The patient underwent partial pericardiectomy with delayed sternal closure and open irrigation. On day 23, he developed right shoulder pain, and imaging revealed a pseudoaneurysm of the ascending aorta. Thoracic endovascular aortic repair combined with bovine pericardial patch repair was performed. He survived and remained stable during a 13-month outpatient follow-up. Given the potential for fatal outcomes, clinicians should maintain a high index of suspicion and initiate prompt management, despite the rarity of this…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
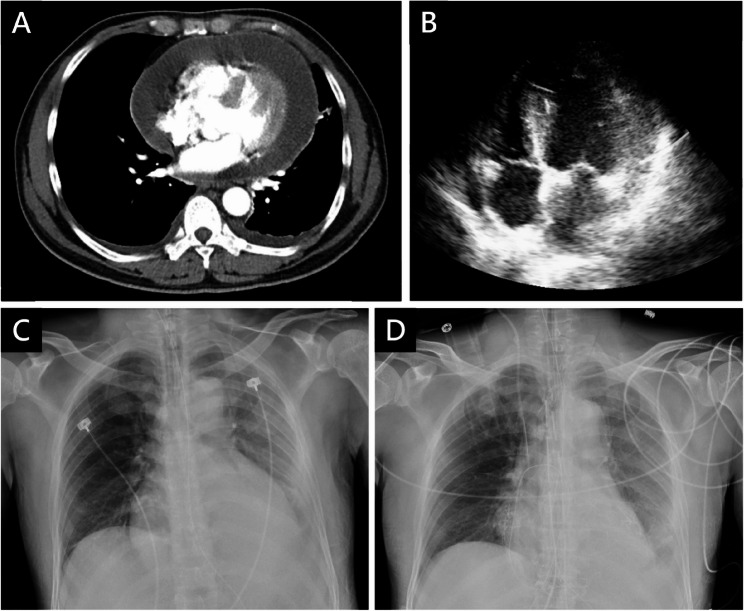 Figure 1
Figure 1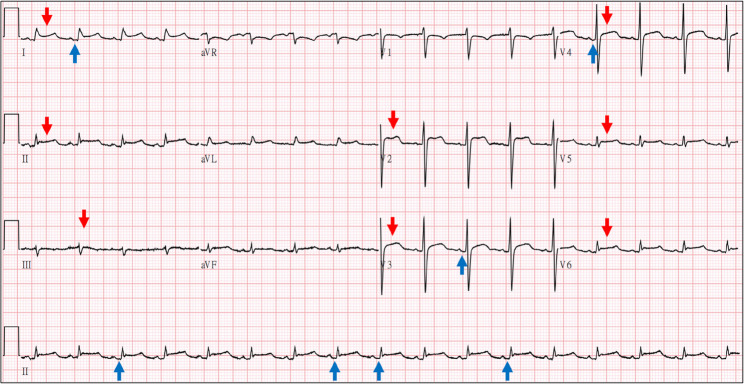 Figure 2
Figure 2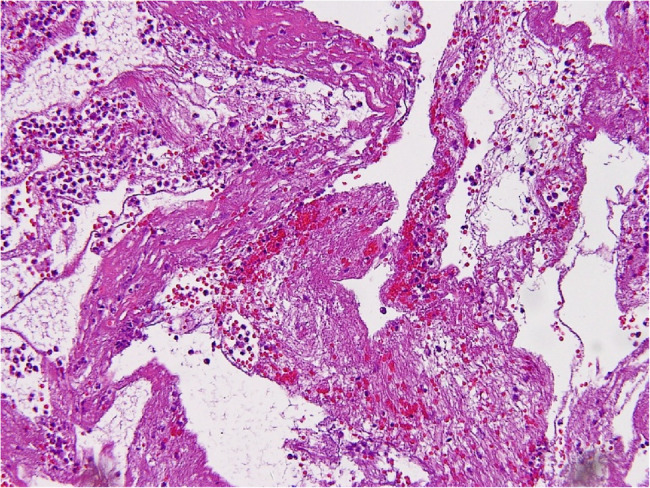 Figure 3
Figure 3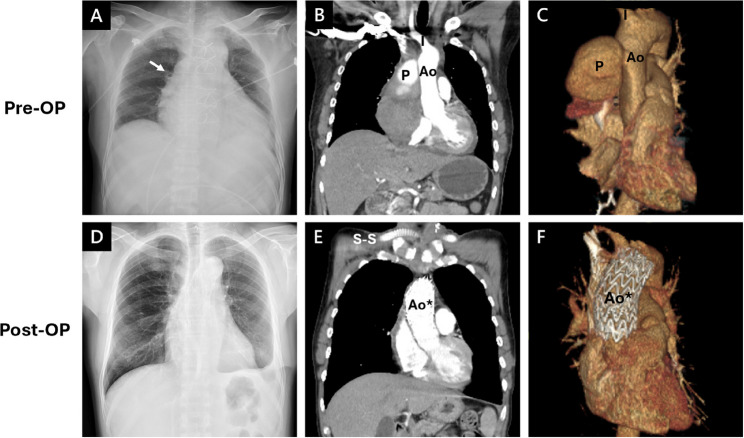 Figure 4
Figure 4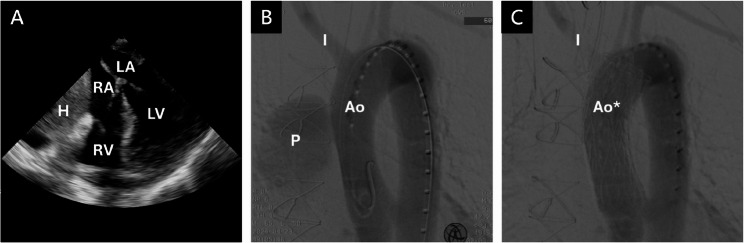 Figure 5
Figure 5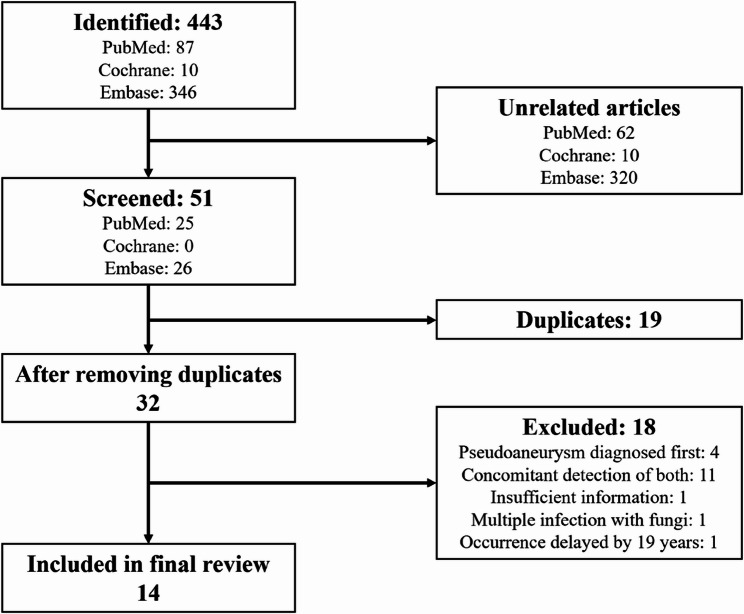 Figure 6
Figure 6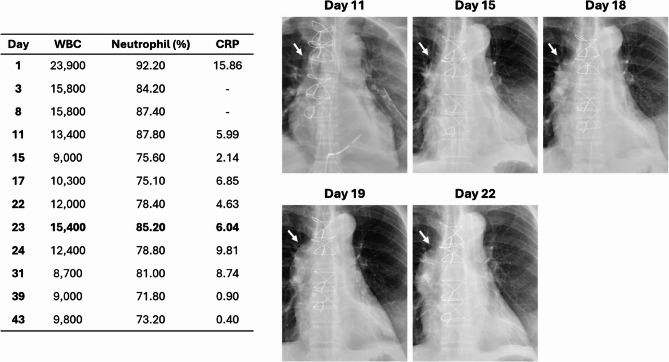 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPericarditis and Cardiac Tamponade · Infectious Aortic and Vascular Conditions · Infective Endocarditis Diagnosis and Management
Introduction
Purulent pericarditis has become uncommon in the antibiotic era, and its coexistence with an aortic pseudoaneurysm is even rarer. This combination can lead to a life-threatening clinical emergency with a high risk of fatal progression. However, the underlying pathophysiological connection remains unclear, as reported in several similar cases. Here, we describe a case of a 46-year-old man diagnosed with methicillin-resistant Staphylococcus aureus (MRSA) purulent pericarditis complicated by a mycotic pseudoaneurysm of the ascending aorta. To better understand this rare phenomenon, we reviewed 14 published cases [1–14], aiming to analyze their clinical features, explore plausible mechanisms, and provide a useful reference for future clinical practice.
Case presentation
A 46-year-old man with a history of intravenous heroin use and hepatitis C was transferred to our medical center due to persistent chest pain and cold sweats for three days. At the referring local hospital, chest computed tomography (CT) and transthoracic echocardiogram (TTE) revealed a large pericardial effusion encasing the heart (25 mm; Fig. 1A, B). Pericardiocentesis (PCC) yielded 300 mL of yellowish, turbid fluid. Upon arrival at our emergency department, he exhibited tachycardia and tachypnea (temperature 36.0 °C, heart rate 102 bpm, blood pressure 141/104 mmHg, and respiratory rate 30/min). The electrocardiogram (ECG) demonstrated diffuse ST-segment elevations with PR segment depressions (Fig. 2). Chest X-ray (CXR) revealed an enlarged cardiac silhouette (Fig. 1C), and laboratory investigations showed leukocytosis (23,900/µL) and an elevated C-reactive protein (CRP 15.86 mg/dL). Empirical vancomycin plus ceftriaxone therapy was initiated based on the working diagnosis of purulent pericarditis.
Fig. 1. Preoperative Imaging of the Chest Upon Admission and Postoperative Radiograph. (A) Chest CT conducted at the former hospital revealed a 25.79 mm large pericardial effusion surrounding the entire heart. (B) TTE subcostal view showed a 25.48 mm pericardial effusion. (C) CXR (AP view) showed an enlarged heart configuration. (D) CXR (AP view) after partial pericardiectomy demonstrated a smaller heart size
Fig. 2. Electrocardiogram with Significant Pericarditis Patterns. The significant patterns included diffuse ST elevation (red arrows) and PR depression (blue arrows)
On day 2, partial pericardiectomy was performed to control the infection and prevent progression to constrictive pericarditis. Intraoperatively, 300 mL of purulent fluid was drained, and the pericardial cavity was irrigated with warm saline irrigation and packed with gauze. The surgery was uneventful, and the mediastinal wound was left open for ongoing observation and serial irrigation. The postoperative CXR demonstrated a reduction in cardiac size (Fig. 1D). Deep pus collected intraoperatively grew methicillin-resistant Staphylococcus aureus (MRSA), prompting escalation of antibiotics to daptomycin. Histopathological examination demonstrated suppurative inflammation with dense neutrophilic infiltration and fibrinous tissue (Fig. 3). Serial wound irrigations were performed every other day, and the sternal wound was closed on postoperative day 6.
However, on day 23, the patient developed chest pain in the morning. His vital signs were within normal limits except for elevated blood pressure (145/113 mmHg). Five hours later, the pain radiated to his right shoulder and arm, for which diclofenac gel was prescribed for pain relief. Two hours afterward, the symptoms recurred, prompting further evaluation. Repeat vital signs revealed hypotension (88/53 mmHg) and bradycardia (58 bpm). The ECG showed normal sinus rhythm without abnormal patterns. Portable CXR demonstrated an enlarged cardiac configuration (Fig. 4A). Urgent CT scan revealed a contained rupture on the right side of the ascending aorta, forming a hematoma measuring 12.4 cm × 9.2 cm and compressing the superior vena cava (Fig. 4B and C). Upon recognition of this unexpected finding, the patient was immediately transferred to the operating room for emergency intervention.
Fig. 3. Microscopic Examination of Pericardium Specimen. Hematoxylin and eosin staining of the pericardium demonstrated suppurative inflammation with dense neutrophilic infiltration and fibrinous tissue
Fig. 4. Imaging Studies Before (A-C) and After (D-F) Thoracic Endovascular Aortic Repair. (Ao, Aorta; I, Innominate artery; P, Pseudoaneurysm; Ao, Aorta with TEVAR)*
In the operating room, transesophageal echocardiography (TEE) confirmed a large hematoma compressing the right heart (8.03 × 6.34 cm; Fig. 5A). Thoracic endovascular aortic repair (TEVAR) was performed; partial occlusion of the innominate artery ostium necessitated a left-to-right subclavian artery bypass (S-S bypass) using an 8 mm × 40 cm vascular graft (Fig. 5B, C). Median sternotomy was then performed for debridement, and a 3 × 2 cm defect in the ascending aorta was repaired with bovine pericardium. Subsequently, a left anterolateral thigh (ALT) flap was utilized to reconstruct the sternal wound defect. The procedures went uneventfully, and the patient was discharged on day 45 with oral trimethoprim-sulfamethoxazole and doxycycline.
Fig. 5. Transesophageal Echocardiography and Angiography Images of the Aortic Pseudoaneurysm. (A) TEE showed that the right atrium and right ventricles were compressed by the huge hematoma. (B,** C)** Angiography before and after TEVAR. (H,* Hematoma; RA*,* Right atrium; RV*,* Right ventricle; LA*,* Left atrium; LV*,* Left ventricle; P*,* Pseudoaneurysm; Ao*,* Aorta; Ao**,* Aorta with TEVAR; I*,* Innominate artery)*
Two months later, contrast-enhanced CT scan showed no evidence of pseudoaneurysm or aortic rupture. The most recent visit to our outpatient department was 13 months after discharge, showing no signs of recurrence or complications (Fig. 4D–F).
Discussion
According to the 2025 European Society of Cardiology (ESC) guidelines [15], the primary management of purulent pericarditis requires aggressive intervention to reduce its high mortality risk. This includes pericardial drainage combined with intravenous antibiotics, as well as other strategies such as subxiphoid pericardiotomy with rinsing, intrapericardial thrombolysis using streptokinase, or pericardiectomy. In our case, after partial pericardiectomy, a delayed sternal closure (DSC) was performed to allow repeated irrigation and direct inspection. The open sternotomy site was temporarily covered with a sterile bag and a drain, with gauze changed every other day. Our literature research revealed that typical irrigation involves the use of indwelling drains inserted during pericardiotomy for normal saline flushing; however, DSC with repeated open-cavity wet dressing changes has not previously been reported. We hypothesize that this unconventional approach may have contributed to direct aortic injury, subsequently resulting in the ascending aortic pseudoaneurysm.
A systematic search was conducted using the keywords and the Boolean operators: (“Purulent pericarditis” OR “Pericardial effusion” OR “Pericarditis”) AND (“Pseudoaneurysm” OR “False aneurysm” OR “Mycotic aneurysm” OR “Infected aneurysm”) AND (“Aortic” OR “Aorta”). Because of the rarity of this complication, no time restrictions were applied, and only English-language publications were included. Three major medical databases – PubMed, Cochrane Library, and Embase – were searched and yielded 443 articles in total. After scanning abstracts, removing duplicates, and excluding irrelevant studies, 14 similar cases were included in the final review (Fig. 6).
Fig. 6. Literature Search Strategy and Screening Process
Only 14 similar cases have been reported over the past 70 years. The underlying comorbidities included intravenous drug abuse, diabetes mellitus, and hypertension. Staphylococcus aureus (8 cases) and Streptococcus pyogenes (3 cases) were the predominant pathogens. Most patients underwent surgical interventions, including pericardial window, pericardiostomy, and pericardiectomy. Pseudoaneurysm occurred from immediately postoperatively up to day 91, and most commonly involving the ascending aorta, followed by the aortic arch and the sinus of Valsalva. Among these cases, 11 patients survived, whereas 3 expired before or after the diagnosis of pseudoaneurysm (Tables 1 and 2).
Pseudoaneurysm formation may result from one or more of the following mechanisms. The first is direct injury, which can occur secondary to previous invasive procedures; one article reported an infected aortic suture line after prior surgery as a causative factor [16], and other studies have shown that approximately 65% to 83% of patients with pseudoaneurysms had undergone a previous mediastinal operation [17–19]. All cases reviewed in our study involved one or more procedures before the development of the aortic pseudoaneurysm. The second factor is local extension; infection from adjacent sites – such as pneumonia or pericarditis – may extend to the aortic wall [16, 20–23]. All cases in this study involved pericarditis, suggesting that infection can possibly spread to the aorta in rare circumstances. The third factor is bacteremia in the presence of underlying aortic pathology, particularly atherosclerosis [11, 23], which is the most common condition in patients with pseudoaneurysm. Bacteremia may lead to microbial seeding of atherosclerotic plaques, causing progressive aortic wall erosion and eventual rupture. Other potential mechanisms, including lymphatic spread or septic embolization from infective endocarditis, have also been proposed to contribute to pseudoaneurysm formation.
Table 1. Summary of 14 reported cases of purulent pericarditis with pseudoaneurysmAuthor (Year)Sex/AgeChief ComplaintMedical HistoryPathogenLocation ofPseudoaneurysmTime1Foley MM (1956)M/6Febrile, malaise- M. tuberculosis Sinus of Valsalva91d2Fitzgerald JD (1964)M/52Lassitude, vague Ill- S. aureus Ascending aorta8d3Brahan RB (1990)F/70Substernal CP, feverDM C. septicum Aortic arch14d4Aranda J Jr (1998)M/63SOB, lightheadedness, fever, coughPSVT S. aureus Ascending aortaPost-OP5Barth H (2000)F/16SOB, fever, diarrheaVaricella S. pyogenes Ascending aorta2d6Ingoglia M (2011)M/57Substernal CPHTN, HLD, CKD, COPD, smoking, CAD s/p PCI MSSA Ascending aortaPost-OP7Erkut B (2011)F/8SOB, fever, sore throat- Staphylococcus Ascending aorta3d8Tan CO (2013)M/38RUQ painIVDA MRSA Sinus of ValsalvaIntra-OP9Han S (2016)F/49Severe SOBUncontrolled DM, HTN K. pneumoniae Ascending aortaPost-OP10Meier D (2018)M/42Tiredness, diarrhea, jaundice, leg edemaIVDA, untreated HIV, HCV liver cirrhosis MSSA Ascending aorta7d11Fry E (2018)F/18Pleuritic CP, SOBStrep pharyngitis S. pyogenes Ascending aortaA few days12Higuchi T (2022)F/10Neck and bilateral shoulder pain- S. pyogenes Aortic arch6d13Song JG (2023)F/2Persistent fever, AMS- MRSA Ascending aorta7d14Pandhair O (2023)M/61Positional CP, SOBMRSA cellulitis MRSA Aortic arch4d*This case (2025)M/46Persistent CP, cold sweatIVDA, HCV MRSA Ascending aorta21d
Table 2. Intervention of all reviewed cases of purulent pericarditis with subsequent pseudoaneurysmPericardial Effusion/Volume (mL)InterventionOutcomePurulent PericarditisMycotic Pseudoaneurysm1Clear yellow/90PCC, pericardiectomyNone (Autopsy)Dead2Cloudy yellow/270;3,000 in total (7 taps)PCC, pericardial windowNone (Ruptured)Dead3Exudate/-PCCAneurysmectomy + Dacron graftAlive4Serosanguinous/750PCC, pericardial windowNone (Refused)Alive5Honey-colored, viscous/150PCC, pericardial windowAneurysmectomy + homograftAlive6Cloudy and bloody/-Pericardial window(subxiphoid + left minithoracotomy)Ascending aortic replacement (Hemashield graft)Closure of SVC fistula (Bovine pericardial patch)Alive7Viscous/350Subxiphoid pericardial drainagePericardial patchAlive8UnmentionedPericardial windowResection (anterior mitral valve leaflet homograft)Alive9Yellowish, turbid/500Subxiphoid pericardiostomyAscending aortic replacement (Hemashield graft)Alive10Purulent/1250Percutaneous drainage + subxiphoid surgical drainageAscending aorta + hemiarch replacement (Dacron graft)Alive11Serous/300; Purulent/130PCC + drainageCorMatrix patchAlive12Cloudy/200Pericardial drainageAneurysmectomy + ascending aortic graftAlive13Brownish-red with fibrin/330PCC + catheter drainage + decorticationAneurysmectomy + aortic repairAlive14Hazy/600PCC, pericardial windowNone (Died before surgery)Dead*Yellowish, turbid/300PCC, partial pericardiectomyDSC, open drainage, wet dressingZone 0 TEVAR + Left-to-right S-S bypassAortic repair (bovine pericardial patch)Alive
In our patient, pseudoaneurysm formation was likely multifactorial. Although DSC with repeated wet dressings may have contributed to aortic wall injury, mechanical trauma alone seems insufficient to explain the delayed onset, as no pseudoaneurysm was identified during subsequent irrigations. The chest radiograph from day 11 to day 22 demonstrated a progressively enlarging right cardiac border, accompanied by elevated WBC and CRP levels, suggesting a potential infectious involvement of the ascending aorta (Fig. 7). Collectively, these findings indicate a probable association among repeated invasive management, ongoing infection from pericarditis, and subsequent pseudoaneurysm formation.
Fig. 7. Serial Laboratory Data and Chest X ray Images Over the Hospital Course
This study contains several limitations. First, as a single-case report with atypical postoperative course, its generalizability is limited; therefore, our observations should be interpreted as an association rather than a causal relationship. Second, the number of comparable cases in the literature review is very small, and the initial management strategies were heterogeneous, making statistical analysis arduous. Third, our review was constrained by the rarity of the condition and by reliance on published case reports, which are susceptible to reporting bias. These limitations cannot be overcome at present, and larger case series or systematic reviews will be necessary to prove its causality in the future.
Conclusion
Purulent pericarditis complicated by an ascending aortic pseudoaneurysm is an exceptionally rare but potentially fatal condition. In this case, the most plausible pathogenesis was multifactorial, involving direct aortic injury with contiguous infectious spread from methicillin-resistant Staphylococcus aureus (MRSA) pericarditis. This report also highlights that delayed sternal closure – previously unreported strategy in this setting – may be a risk factor and should therefore be applied with caution. We recommend avoiding unnecessary invasive procedures and ensuring close surveillance during the early postoperative period.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1FOLEY MM, PROBERT WR, SEAL RM. False aneurysm of ascending thoracic aorta complicating tuberculous pericarditis. Tubercle. 1956;37(3):183-6. 10.1016/s 0041-3879(56)80039-1. PMID: 13352372.10.1016/s 0041-3879(56)80039-113352372 · doi ↗ · pubmed ↗
- 2Aranda J Jr, Tauth J, Henning RJ, O’Hara M. Pseudoaneurysm of the thoracic aorta presenting as purulent pericarditis and pericardial effusion. Cathet Cardiovasc Diagn. 1998;43(1):63 – 7. 10.1002/(sici)1097-0304(199801)43:1%3C 63::aid-ccd 19%3E 3.0.co;2-u. PMID: 9473194.10.1002/(sici)1097-0304(199801)43:1<63::aid-ccd 19>3.0.co;2-u 9473194 · doi ↗ · pubmed ↗
- 3Barth H, Moosdorf R, Bauer J, Schranz D, Akintürk H. Mycotic pseudoaneurysm of the aorta in children. Pediatr Cardiol. 2000;21(3):263-6. 10.1007/s 002460010054. PMID: 10818188.10.1007/s 00246001005410818188 · doi ↗ · pubmed ↗
- 4Erkut B, Becit N, Kantarci M, Ceviz N. Mycotic pseudoaneurysm of the ascending aorta following purulent pericardial effusion diagnosed by multi-slice computed tomography. Cardiovasc J Afr. 2011;22(3):143–4. PMID: 21713305.10.5830/CVJA-2010-03821713305 · doi ↗ · pubmed ↗
- 5Schulz-Menger J, Collini V, Gröschel J, Adler Y, Brucato A, Christian V, Ferreira VM, Gandjbakhch E, Heidecker B, Kerneis M, Klein AL, Klingel K, Lazaros G, Lorusso R, Nesukay EG, Rahimi K, Ristić AD, Rucinski M, Sade LE, Schaubroeck H, Semb AG, Sinagra G, Thune JJ, Imazio M, ESC Scientific Document Group. 2025 ESC Guidelines for the management of myocarditis and pericarditis. Eur Heart J. 2025;46(40):3952–4041. 10.1093/eurheartj/ehaf 192. PMID: 40878297.10.1093/eurheartj/ehaf 19240878297 · doi ↗ · pubmed ↗
- 6Atik FA, Navia JL, Svensson LG, Vega PR, Feng J, Brizzio ME, Gillinov AM, Pettersson BG, Blackstone EH, Lytle BW. Surgical treatment of pseudoaneurysm of the thoracic aorta. J Thorac Cardiovasc Surg. 2006;132(2):379 – 85. 10.1016/j.jtcvs.2006.03.052. PMID: 16872966.10.1016/j.jtcvs.2006.03.05216872966 · doi ↗ · pubmed ↗
- 7Villavicencio MA, Orszulak TA, Sundt TM 3rd, Daly RC, Dearani JA, Mc Gregor CG, Mullany CJ, Puga FJ, Zehr KJ, Schaff HV. Thoracic aorta false aneurysm: what surgical strategy should be recommended? Ann Thorac Surg. 2006;82(1):81 – 9; discussion 89. 10.1016/j.athoracsur.2006.02.081. PMID: 16798195.10.1016/j.athoracsur.2006.02.08116798195 · doi ↗ · pubmed ↗