Treatment failure and associated risk factors for periprosthetic-joint infections caused by streptococci versus other etiologies: a single-center retrospective cohort study
Arnaud Fischbacher, Jonathan Tschopp, Sylvain Steinmetz, Noémie Boillat-Blanco, Olivier Borens

TL;DR
This study found that streptococcal joint infections have similar treatment failure rates as other infections, but certain types like Streptococcus dysgalactiae and specific treatments like DAIR are linked to higher failure risks.
Contribution
Identified specific risk factors for treatment failure in streptococcal periprosthetic-joint infections compared to other pathogens.
Findings
Streptococcal periprosthetic-joint infections had a 23% treatment failure rate, similar to other pathogens (21%).
Streptococcus dysgalactiae and DAIR treatment were significantly associated with higher failure rates in streptococcal infections.
Streptococcal etiology alone was not significantly linked to treatment failure.
Abstract
There is no consensus on the antibiotic course or type of surgical treatment in streptococcal periprosthetic-joint infections (PJIs). We aimed to compare the treatment failure rate at 2 years of PJIs caused by streptococci to PJIs caused by other pathogens and identify factors associated with failure. It was a single-center retrospective cohort study conducted between 2009 and 2019. We included all patients aged ≥ 18 years undergoing treatment for hip or knee PJI with a 2-year follow-up. We analyzed the treatment failure rate at 2 years of streptococcal PJIs versus PJIs caused by other pathogens with failure defined as a non-successful treatment using the Delphi-based international multidisciplinary consensus of success. We also analyzed factors associated with failure including streptococcal etiology and type of treatment. We included 404 patients; 62 (15%) had a streptococcal PJI,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
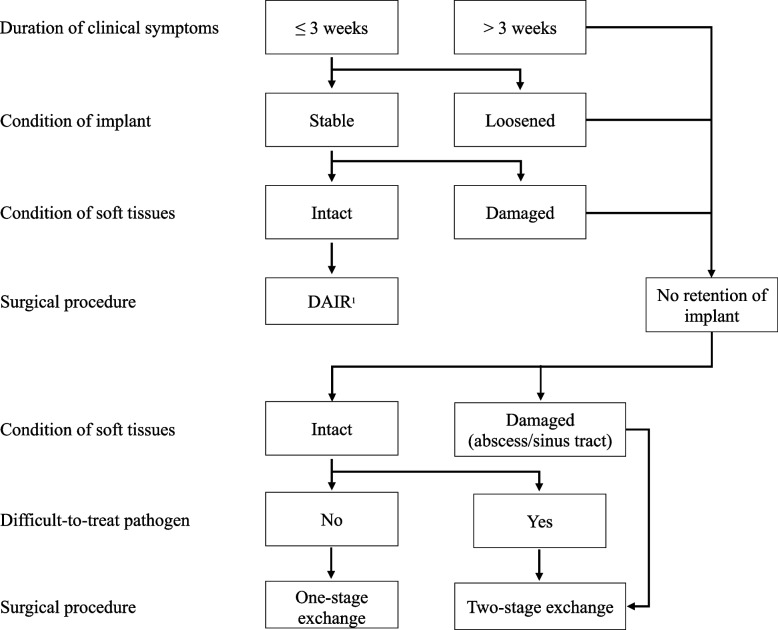 Figure 1
Figure 1- —University of Lausanne
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Infections and Treatments · Orthopaedic implants and arthroplasty · Bone fractures and treatments
Introduction
Total hip and knee arthroplasties are expected to increase significantly in the next decades to improve the quality of life of an ever-aging population [1]. Periprosthetic-joint infection (PJI) is one of the most feared complications after arthroplasty, with an incidence of 1% to 2% after primary arthroplasty and 4% to 8% after revision arthroplasty [2, 3]. This complication is associated with prolonged hospital stays, high costs and increased morbidity and mortality [4–8]. Streptococci are responsible for approximately 10% of PJIs and are the second most common bacterial species after staphylococci [9]. Hematogenous spread from a distant focus of infection represents the predominant route of infection. Streptococci were thought to be easy to treat due to their high sensitivity to antibiotics and their acute presentation, making debridement, antibiotics and implant retention (DAIR) possible. However, multiple studies have linked streptococci to an increased risk of recurrence compared to other bacteria with high relapse rates (20–42%), suggesting that these infections may be labeled as “difficult to treat” [9–11]. Some authors even recommend that these infections should be treated with a prolonged course of suppressive antibiotics [12]. The reason for this is still unclear and could be due to the lack of an effective anti-biofilm treatment, knowing that the use of rifampin did not show evidence to improve the outcome [10, 12, 13]. Finally, there is no consensus on the influence of surgical treatment selection with recent studies suggesting that two-stage revision is the treatment of choice [14, 15].
This retrospective study aimed to compare the treatment failure rate of streptococcal PJIs to PJIs caused by other pathogens and identify factors associated with failure.
Materials and methods
Study design, setting and participants
We performed a single-center retrospective cohort study in a university hospital in Switzerland between 2009 and 2019. We included all consecutive patients aged ≥ 18 years undergoing treatment for hip or knee PJI (both primary and revision arthroplasties). Patients were identified from the intervention register of the hospital. All included patients had a follow-up medical visit after the second postoperative year and a signed general consent form for their data to be used retrospectively. We excluded patients with unknown 2-year outcome due to loss of follow-up and those who did not give consent for their data to be used.
Study procedures
We extracted demographics, type of prosthesis, characteristics of the infection, type of surgical intervention and antimicrobial treatment from institutional medical records. Microbiological results including blood cultures, synovial fluid and tissue sample cultures and PCRs (eubacterial PCR 16S) were also extracted. Information on follow-up at 3, 6, 12 and 24 months was extracted from the same institutional medical records.
Definitions
PJIs were retrospectively defined using the 2021 European Bone and Joint Infection Society (EBJIS) criteria [16]. The infection was classified according to the duration of symptoms at diagnosis as acute (≤ 3 weeks of symptoms) or chronic (> 3 weeks of symptoms). PJIs were furthermore classified into early (< 3 months), delayed (> 3 months to ≤ 2 years) and late (> 2 years) infections according to the time to onset following the implantation or revision surgery [3]. Treatment failure at 2-year follow-up was defined as a non-successful treatment using the Delphi-based international multidisciplinary consensus of success and could be either infection relapse, new infection or death [17]. Infection relapse was defined as the persistence or reappearance of signs and/or symptoms of infection (pain, swelling, redness or wound fistula) during the first two years after surgery. New infection was defined the same way but needed the identification of a different pathogen from the primary PJI.
Surgical treatment
An established treatment algorithm was usually followed after multidisciplinary discussion to decide on the type of surgical treatment (Fig. 1) [3]. Patients with acute infections usually underwent DAIR, with polyethylene exchange systematically performed. Patients with chronic infections, loosened implants or damaged soft tissues usually underwent one- or two-stage exchange depending on the soft tissues (abscess or sinus tract). In case of a two-stage exchange, a longer interval (≥ 6 weeks) was used before reimplantation when a difficult-to-treat pathogen (i.e., with no anti-biofilm therapy available) was documented. Implant removal, joint arthrodesis, or amputation were performed in severely immunocompromised patients, in those with active intravenous drug use, and in cases where arthroplasty would not provide any benefit. Inappropriate surgical treatment was defined as DAIR for a chronic infection.Fig. 1. Surgical treatment algorithm (adapted from [3]). ^1^DAIR: debridement, antibiotics, and implant retention
Antimicrobial treatment
The medical team usually followed international guidelines on antibiotic treatment [18]. Empiric intravenous antibiotics were started at time of surgery. A switch to targeted antibiotics was usually performed as soon as possible upon reception of microbiological results (tissue samples and sonication) and susceptibility testing. The intravenous treatment was given for 1–2 weeks depending on the clinical evolution and current guidelines and was followed by an oral regimen for a total of 12 weeks. In case of a two-stage exchange, antibiotics were continued until re-implantation without an antibiotic-free interval. A prolonged course of suppressive antibiotics was never used. The type of antibiotic treatment was recorded as well as the use of anti-biofilm treatment (i.e., at least one day of rifampin for Gram-positive cocci and fluoroquinolones for Gram-negative bacilli). Streptococcal PJIs were treated with rifampin until published data showed no evidence of benefit in the outcome [10, 12, 13].
Data analyses
Statistical analyses were performed with STATA 16® (Statacorp, Texas). Continuous variables are presented as median with interquartile range (IQR) and categorical variables as numbers with percentage. We compared demographics, type of prosthesis, characteristics of the infection and type of intervention and antimicrobial treatment between patients with streptococcal PJIs and those with PJIs caused by other pathogens using Mann Whitney-U, chi-squared, or Fisher exact tests, as appropriate. A P-value ≤ 0.05 was considered statistically significant. To identify factors associated with treatment failure in the whole study population and in patients with streptococcal PJIs, we used a multivariate logistic regression model with backward selection and a significance level of P ≥ 0.10 for removal from the model.
Results
Study population
Of 456 consecutive screened patients with PJI, 37 (8%) were excluded due to lack of consent and 15 (3%) due to loss of follow-up within 2 years after PJI. Five (10%) of these 52 excluded patients had streptococcal PJIs. A total of 404 patients were included in the study; 62 (15%) had streptococcal PJIs (Table 1). Among patients with streptococcal PJIs, 56% had hip PJIs and 44% knee PJIs. Patients with streptococcal PJIs were older at time of diagnosis and more comorbid. Streptococcal PJIs were more often acute than non-streptococcal PJIs. Table 1. Demographic and clinical data of streptococcal versus non-streptococcal PJIs (n = 404 patients)Streptococcal PJIsN** = 62 (15%)****Non-streptococcal PJIsN = 342 (85%)PDemographics^1^ Age, median (IQR)75(66–81)69(61–77)0.004 Males, n (%)31(50)189(55)0.44 Charlson Comorbidity Index, median (IQR)4(3–6)4(2–5)0.03 BMI, median (IQR)29(24–33)29(25–33)0.58Type of prosthesis, n (%)0.70 Hip35(56)202(59) Knee27(44)140(41)Type of infection, n (%)0.03 Acute36(58)148(43) Chronic26(42)194(57)Infection timing, n (%)0.26 Early13(21)73(21) Delayed34(55)153(45) Late15(24)116(34)Type of intervention, n (%)0.33 DAIR22(35)121(35) One-stage exchange3(5)43(13) Two-stage exchange34(55)152(44) Implant removal3(5)22(6) Arthrodesis02(1) Amputation02(1)Use of anti-biofilm antibiotics^2^, n (%)8(13)239(70) < 0.001**Treatment failure after 2 years, n (%)14(23)71(21)0.78 Infection relapse (%)9(64)36(51) New infection (%)3(21)19(27) Death (%)2(14)16(22)IQR: interquartile range, BMI: body mass index, DAIR: debridement, antibiotics, and implant retention^1^Race or ethnicity information was not available; ^2^At least one day of either rifampin or fluoroquinolones
Microbiology
Among the 404 patients, 353 (87%) had a documented pathogen. 62 (15%) had a streptococcal monomicrobial PJI. For non-streptococcal PJIs, the most isolated bacteria were coagulase-negative staphylococci followed by Staphylococcus aureus and Gram-negative bacilli. Of note, three polymicrobial infections included streptococci. The detailed distribution of bacterial species is provided in Table 2. Table 2. Microbiological findings of PJIs (n = 404 patients)Streptococcal speciesN = 62**(15%)Streptococcus pyogenes4(6%)Streptococcus agalactiae17(28%)Streptococcus dysgalactiae16(26%)Streptococcus bovis group2(3%)Streptococcus viridans group23(37%)Other bacteria speciesN***** = 342***(85%)**Staphylococcus aureus^1^88(26%)Coagulase-negative staphylococci107(31%)Enterococci12(4%)Other Gram-positive cocci^2^2(1%)Gram-negative bacilli^3^36(11%)Anaerobes^4^21(6%)Fungi1(1%)Polymicrobial infections^5^24(7%)Culture-negative infections51(15%)^1^80 methicillin-sensitive S. aureus (MSSA), 8 methicillin-resistant S. aureus (MRSA)^2^1 Bacillus cereus, 1 Corynebacterium striatum^3^14 E. coli, 3 Citrobacter koseri, 3 Proteus mirabilis, 1 Proteus vulgaris, 5 Pseudomonas aeruginosa, 2 Enterobacter cloacae, 3 Klebsiella aerogenes, 3 Klebsiella pneumoniae, 3 Campylobacter fetus^4^14 Cutibacterium acnes, 1 Propionibacterium avidum, 1 Granulicatella, 1 Bacterioides fragilis, 1 Bacterioides vulgatus, 1 Fingoldia magna, 1 Clostridium celerecrescens, 1 Ruminococcus gnavus^5^1 Streptococcus dysgalactiae, 1 Streptococcus agalactiae, 1 Streptococcus viridans group
Treatment
Table 1 summarizes the surgical and antimicrobial treatment. In streptococcal PJIs, surgical treatment consisted of DAIR in 22 (35%) patients (with polyethylene exchange systematically performed), one-stage exchange in 3 (5%), two-stage exchange in 34 (55%), and implant removal in 3 (5%). The only treatment difference between streptococcal and non-streptococcal PJIs was that streptococcal PJIs were treated less often with anti-biofilm antibiotics (13% vs. 70%, P < 0.001). Only two streptococcal PJIs were treated with DAIR and anti-biofilm antibiotics, with treatment failure in both.
Treatment failure at 2 years of streptococcal PJIs versus PJIs caused by other pathogens
Among the 62 streptococcal PJIs, treatment failure at 2-year follow-up was observed in 14 (23%) patients. Infection relapse occurred in 9 (64%) patients and new infection in 3 (22%). Two patients (14%) died. The treatment failure rate was similar to that for PJIs caused by other pathogens (21%, 71/342) (P = 0.78) (Table 1). We also found a similar failure rate between streptococcal PJIs and PJIs caused by other pathogens after one-stage exchange (0/3, 0% vs. 6/43, 14%, P = 0.49), two-stage exchange (3/34, 9% vs. 24/152, 16%, P = 0.30), and DAIR (9/22, 41% vs. 34/121, 28%, P = 0.35).
Factors associated with treatment failure at 2 years
Streptococci infection was not associated with treatment failure in univariate (OR = 0.88, 95% CI 0.41–1.89, P = 0.73) or multivariate logistic regression analyses (OR = 1.55, 95% CI 0.62–3.89, P = 0.35) (Table 3). Only polymicrobial infections were associated with treatment failure in univariate (OR = 3, 95% CI 1.18–7.64, P = 0.02) and multivariate analyses (OR = 6.71, 95% CI 2.14–21.06, P = 0.001). Conversely, risk of treatment failure was reduced in culture-negative infections in univariate (OR = 0.06, 95% CI 0.21–0.54, P = 0.001) and multivariate analyses (OR = 0.07, 95% CI 0.01–0.58, P = 0.01).
Regarding the surgical treatment, DAIR was associated with treatment failure in univariate (OR = 2.87, 95% CI 1.76–4.69, P = 0.001) and multivariate analyses (OR = 11.27, 95% CI 3.58–35.50, P = 0.001). Risk of treatment failure was reduced with the use of anti-biofilm antibiotics in univariate analysis (OR = 0.61, 95% CI 0.38–0.99, P = 0.05) but not in the multivariate model.
Table 3. Factors associated with 2-year treatment failure: univariate and multivariate analysesCureN** = 319 (79%)FailureN = 85 (21%)Univariate analysisMultivariate analysisOR95% CIPOR95% CIPDemographics Age, median (IQR)70(62–78)71(62–80)1.010.99–1.030.38 Males, n (%)169(53)51(60)1.330.82–2.170.25 Charlson, Comorbidity Index, median (IQR)4(2–5)4(2–5)1.010.89–1.140.93 BMI, median (IQR)29(25–33)29(26–33)1.020.98–1.060.28Type of prosthesis, n (%) Hip185(58)52(61)reference Knee134(42)33(39)0.880.53–1.430.60Type of infection, n (%) Acute135(42)49(58)referencereference Chronic184(58)36(42)0.540.33–0.870.0123.201.02–10.100.05Infection timing, n (%) Early67(21)19(22)reference Delayed156(49)31(37)0.700.37–1.330.28 Late96(30)35(41)1.290.68–2.440.44Use of antibiofilm antibiotics^1^, n (%)203(64)44(52)0.610.38–0.990.05Type of intervention, n (%) Non-DAIR^2^223(70)38(45)reference DAIR96(30)47(55)2.871.76–4.69 < 0.00111.273.58–35.50 < 0.001Inappropriate surgery4(1)3(4)2.881.31–13.130.17Microbiology* Staphylococcus aureus*^3^66(21)22(26)referencereference Coagulase-negative staphylococci88(28)19(22)0.650.32–1.290.221.380.58–3.290.47* Streptococcus* spp48(15)14(16)0.880.41–1.890.731.550.62–3.890.35* Enterococcus* spp9(3)3(4)1.000.25–4.031.001.510.27–8.350.64 Other Gram positive cocci^4^20 Gram-negative bacilli^5^27(8)9(11)1.000.41–2.451.001.330.47–3.770.59 Anaerobes^6^17(5)4(5)0.710.21–2.320.571.330.35–5.060.67 Fungi01 Polymicrobial infections^7^12(4)12(14)31.18–7.640.026.712.14–21.060.001** Culture-negative infections50(16)1(1)0.060.21–0.54** < 0.0010.070.01–0.580.01**IQR: interquartile range, BMI: body mass index, DAIR: debridement, antibiotics, and implant retention^1^At least one day of either rifampin or fluoroquinolones^2^ Cure: one-stage exchange (n = 40), two-stage exchange (n = 159), implant removal (n = 20), arthrodesis (n = 2), amputation (n = 2)/Failure: one-stage exchange (n = 6), two-stage exchange (n = 27), implant removal (n = 5), arthrodesis (n = 0), amputation (n = 0)^3^80 methicillin-sensitive S. aureus (MSSA), 8 methicillin-resistant S. aureus (MRSA)^4^1 Bacillus cereus, 1 Corynebacterium striatum^5^14 E. coli, 3 Citrobacter koseri, 3 Proteus mirabilis, 1 Proteus vulgaris, 5 Pseudomonas aeruginosa, 2 Enterobacter cloacae, 3 Klebsiella aerogenes, 3 Klebsiella pneumoniae, 3 Campylobacter fetus^6^14 Cutibacterium acnes, 1 Propionibacterium avidum, 1 Granulicatella, 1 Bacterioides fragilis, 1 Bacterioides vulgatus, 1 Fingoldia magna, 1 Clostridium celerecrescens, 1 Ruminococcus gnavus^7^1 Streptococcus dysgalactiae, 1 Streptococcus agalactiae, 1 Streptococcus viridans group
Factors associated with treatment failure at 2 years among patients with streptococcal PJIs
S. dysgalactiae infection was associated with treatment failure (6 relapses and 2 new infections in 16 patients, 50%) in univariate (OR = 6.67, 95% CI 1.40–31.72, P = 0.02) and multivariate analyses (OR = 9.45, 95% CI 1.37–65.46, P = 0.02) (Table 4). The frequency of treatment failure was higher in patients with a streptococcal PJI treated with DAIR compared to other surgical treatments (9/22, 41% vs. 5/40, 12%) making DAIR a factor associated with failure in univariate (OR = 4.85, 95% CI 1.37–17.17, P = 0.01) and multivariate analyses (OR = 9.31, 95% CI 1.80–48.20, P = 0.008). Risk of treatment failure was not reduced with the use of anti-biofilm antibiotics (OR = 2, 95% CI 0.50–8.00, P = 0.33). Finally, late presumably hematogenous infections were not associated with treatment failure (OR = 0.80, 95% CI 0.17–3.77, P = 0.78). Table 4. Factors associated with 2-year treatment failure among patients with a streptococcal PJICureN** = 48 (77%)FailureN = 14 (23%)Univariate analysisMultivariate analysisOR95% CIPOR95% CIPDemographics Age, median (IQR)75(67*–81)73(62–81)0.980.93–1.030.44 Males, n (%)21(44)10(71)3.210.88–11.700.07 Charlson, Comorbidity Index, median (IQR)5(4–6)4(2–7)0.980.74–1.300.90 BMI, median (IQR)29(24–34)30(26–32)1.030.93–1.140.54Type of prosthesis, n (%) Hip27(56)8(57)reference Knee21(44)6(43)0.960.29–3.210.95Type of infection, n (%) Acute25(52)11(79)reference Chronic23(48)3(21)0.300.07–1.200.09Infection timing, n (%) Early8(17)5(36)reference Delayed30(62)4(28)0.210.05–0.980.05 Late10(21)5(36)0.800.17–3.770.78Use of antibiofilm antibiotics^1^, n (%)8(17)4(29)20.50–8.000.33Inappropriate surgery1(2)0Streptococcus* species, n (%)* Streptococcus* viridans group20(42)3(21)referencereference* Streptococcus pyogenes4(8)0 Streptococcus agalactiae14(29)3(21)1.430.24–8.140.691.340.15–12.250.79 Streptococcus dysgalactiae8(17)8(57)6.671.40–*31.720.029.451.37*–*65.460.02*** Streptococcus* bovis group2(4)0Type of intervention, number (%) Non-DAIR^2^35(73)5(36)referencereference DAIR13(27)9(64)4.851.37*–17.170.019.311.80–*48.200.008IQR: interquartile range, BMI: body mass index, DAIR: debridement, antibiotics, and implant retention^1^At least one day of either rifampin or fluoroquinolones^2^Streptococcal PJIs: one-stage exchange n = 3, two-stage exchange n = 34, implant removal n = 3/Non-streptococcal PJIs: one-stage exchange n = 43, two-stage exchange n = 152, implant removal n = 22, arthrodesis n = 2, amputation n = 2
Discussion
In this study, the 2-year treatment failure rate was similar for streptococcal PJIs and non-streptococcal PJIs (23% vs. 21%, P = 0.78). Only polymicrobial infections were associated with treatment failure, and culture-negative infections with a reduced risk of failure, as already demonstrated [19, 20]. This result does not corroborate previous studies, which showed a higher failure rate in streptococcal PJIs [9–12, 14, 15]. However, our comparable failure rate with other etiologies could be explained by a greater proportion of two-stage exchanges for streptococcal PJIs in our cohort. While 58% of these infections were classified as acute, surgical treatment consisted of DAIR in only 35%. The surgical treatment algorithm was therefore not always followed, and streptococcal PJIs were treated more aggressively over time based on the expertise of the medical team. Recent studies showed a worse prognosis than previously published for streptococcal PJIs managed by DAIR [14, 15, 21]. The time from the onset of symptoms to debridement and performing polyethylene exchange might be a confounding factor. Nevertheless, these results are in line with our study in which DAIR was associated with failure, although polyethylene exchange was systematically performed and DAIR was considered inappropriate in only one patient. This finding supports that DAIR should be avoided in streptococcal PJIs when the microbiology is available before surgery.
Regarding microbiology, we identified a streptococcal species that was associated with a higher failure rate: Streptococcus dysgalactiae. This is consistent with a recent study, which found that Streptococcus dysgalactiae was the most common organism isolated in their failure group [14]. Two previous studies showed that Streptococcus agalactiae was also associated with a higher failure rate, but it was not the case in our study [9, 15]. The role of anti-biofilm antibiotics against streptococcal biofilms is still controversial. Several studies demonstrated that streptococci were able to produce biofilm [22–24]. However, it has been shown that the addition of rifampin does not improve the outcome, which is in accordance with our findings [10, 12–15]. Further research is needed on microbiological differences of streptococci species, such as biofilm formation, as Streptococcus dysgalactiae seems to behave differently. Lack of effective biofilm-active antibiotics may explain the higher failure rate in Streptococcus dysgalactiae PJIs. Streptococcus dysgalactiae could thus be considered a “difficult to treat” pathogen and should be surgically treated more aggressively with an implant exchange. A prolonged course of suppressive antibiotics, as recommended by some authors, could also be used when Streptococcus dysgalactiae is found after DAIR [12].
Finally, we acknowledge the limitations of our study. The study’s reliance on medical records prevented us from recording the length of the antimicrobial treatment. The results may have been distorted if the antibiotic therapy was interrupted, particularly anti-biofilm treatment. It also prevented us from identifying hematogenous infections. We presumed that late streptococcal PJIs were hematogenous. They were not associated with treatment failure, contrary to previous studies, probably due to a lack of power [14]. The accuracy of the PJIs’ definition based on criteria introduced after the collection of data might be questioned, but to overcome this limitation, all patients’ files were reviewed by an infectious disease specialist. Our findings are also limited due to the small number of cases for some streptococcal species and the observational nature of the study, with no randomization of the surgical treatment. However, some strengths of the study should be highlighted, such as the considerable number of included patients and the homogeneity regarding the surgical and antimicrobial treatment throughout the study period.
Conclusions
The treatment failure rate of streptococcal PJIs was similar to that for PJIs caused by other pathogens. However, Streptococcus dysgalactiae and DAIR were factors associated with failure among patients with a streptococcal PJI. Our results suggest that streptococcal PJIs, especially Streptococcus dysgalactiae PJIs, should be surgically treated more aggressively with an implant exchange.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Li HK, Rombach I, Zambellas R, Walker AS, Mc Nally MA, Atkins BL, Lipsky BA, Hughes HC, Bose D, Kümin M, Scarborough C, Matthews PC, Brent AJ, Lomas J, Gundle R, Rogers M, Taylor A, Angus B, Byren I, Berendt AR, Warren S, Fitzgerald FE, Mack DJF, Hopkins S, Folb J, Reynolds HE, Moore E, Marshall J, Jenkins N, Moran CE, Woodhouse AF, Stafford S, Seaton RA, Vallance C, Hemsley CJ, Bisnauthsing K, Sandoe JAT, Aggarwal I, Ellis SC, Bunn DJ, Sutherland RK, Barlow G, Cooper C, Geue C, Mc Meekin N, Brigg · doi ↗ · pubmed ↗
- 2Lora-Tamayo J, Senneville É, Ribera A, Bernard L, Dupon M, Zeller V, Li HK, Arvieux C, Clauss M, Uçkay I, Vigante D, Ferry T, Iribarren JA, Peel TN, Sendi P, Miksic NG, Rodríguez-Pardo D, Del Toro MD, Fernández-Sampedro M, Dapunt U, Huotari K, Davis JS, Palomino J, Neut D, Clark BM, Gottlieb T, Trebše R, Soriano A, Bahamonde A, Guío L, Rico A, Salles MJC, Pais MJG, Benito N, Riera M, Gómez L, Aboltins CA, Esteban J, Horcajada JP, O'Connell K, Ferrari M, Skaliczki G, Juan RS, Cobo J, Sánchez-Somo · doi ↗ · pubmed ↗