Associations of cardiorespiratory fitness and muscle strength during pregnancy with metabolic health outcomes and inflammatory parameters at 1-year postpartum in women after gestational diabetes
Dan Yedu Quansah, Amar Arhab, Jardena J. Puder

TL;DR
Higher fitness and muscle strength during pregnancy may protect against poor metabolic health after gestational diabetes.
Contribution
First study to show that fitness and strength during pregnancy improve postpartum metabolic outcomes in women with gestational diabetes.
Findings
Higher CRF during pregnancy was linked to lower postpartum glucose intolerance, MetS, and insulin resistance.
Higher handgrip strength during pregnancy was associated with better metabolic markers and lower inflammation.
The benefits of handgrip strength were independent of traditional diabetes risk factors.
Abstract
Women with gestational diabetes mellitus (GDM) have increased risk of insulin resistance, glucose intolerance, and low-grade systemic inflammation in the postpartum. Higher cardiorespiratory fitness (CRF) and muscular strength are associated with improved metabolic outcomes in the general population, but data in women with GDM are lacking. We investigated the longitudinal associations of CRF and muscular strength during pregnancy with glucose intolerance, insulin resistance and inflammation parameters at 1-year postpartum in women with GDM. This is a secondary analysis of the MySweetHeart trial, which included 179 women with GDM. During pregnancy, CRF was assessed using the Chester Step test, and muscular strength was measured via handgrip strength (HS) and adjusted for pre-pregnancy body mass index (BMI). At one-year postpartum, participants underwent a 75 g oral glucose tolerance…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
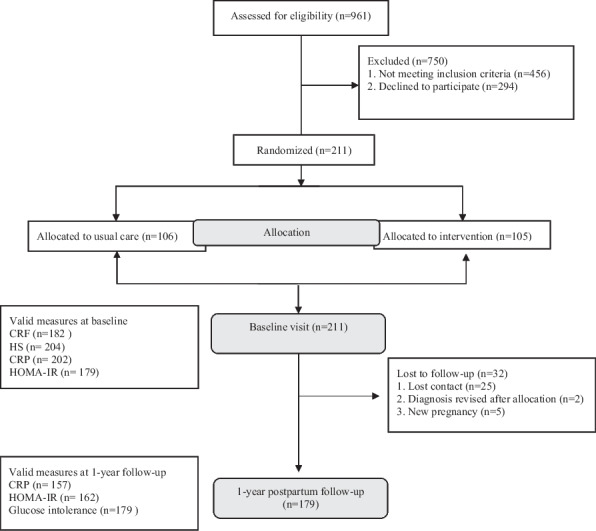 Figure 1
Figure 1- —https://doi.org/10.13039/501100001711Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung
- —University of Lausanne
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGestational Diabetes Research and Management · Pregnancy and preeclampsia studies · Maternal Mental Health During Pregnancy and Postpartum
Introduction
Gestational diabetes mellitus (GDM) is referred to as hyperglycemia first diagnosed during pregnancy without fulfilling the criteria for pre-existing diabetes [1]. GDM is characterized by increased insulin resistance and decreased insulin secretion [2] and is associated with increased risk of the metabolic syndrome (MetS) and future diabetes [3]. Women with GDM have an increased chronic, low-grade inflammation state compared to those without GDM. Excessive weight gain, weight retention and poor glucose control, often observed in women with GDM, can further accentuate the chronic inflammatory state which in turn is linked to insulin resistance, particularly hepatic insulin resistance [4] and the development of future diabetes and CVD in the postpartum [5, 6].
Previous meta-analysis of prospective observational cohorts outside of the perinatal context indicated that low cardiorespiratory fitness (CRF) and handgrip strength (HS) are both independently associated with increased cardiovascular disease (CVD) risk and mortality due to various physiological mechanisms such as impaired insulin sensitivity, altered body composition, disturbed lipid profile, inflammation and dysregulation of blood pressure [7, 8]. CRF is the capacity of cardiorespiratory systems to provide muscles with oxygen during sustained and/or intense exercise, and HS, on the other hand, is the ability to lift and move objects with maximum force for a short period of time [9]. In a large population study, the associations of CRF and HS with mortality [10] remained significant even after adjustment for the traditional cardiovascular risk factor burden. An inverse relationship between high CRF and HS with low grade systemic inflammation has been previously established [11–13]. Outside of pregnancy, population-based studies suggest that higher CRF and HS lower inflammation risk [14]. Physical activity that leads to increased CRF and HS stimulates the release of myokines and other immune mediators during muscle contraction, modulates immune function and reduces systemic inflammation, which are key mechanisms in the prevention and management of chronic diseases such as CVD [15–17].
In the general population, there is a relationship between CRF and HS and metabolic syndrome (MetS) [18–21]. Outside of pregnancy, an independent inverse relationship between high CRF and HS with the prevalence of diabetes including clinically meaningful reductions in diabetes risk by small increments in CRF and HS have also been established [22–27]. Specifically, an inverse relationship between CRF and HS with fasting insulin, insulin resistance and beta cell function have been established, the later independent of obesity [28–30]. During pregnancy, both CRF and HS are related to a reduced risk of GDM while the relationship between pre-natal physical activity intervention and glucose tolerance remains controversial [31–35]. In the postpartum, one study showed that CRF but particularly HS, is strongly associated with improved glucose tolerance and features of MetS at 6–10 years after GDM [36]. There is a protective role of CRF and HS during pregnancy on inflammatory parameters and other cardiometabolic risk factors [17], including a reduced risk of GDM [27, 28].
However, prospective associations of both CRF and HS with insulin resistance, glucose intolerance and metabolic outcomes in metabolically high-risk women with GDM up to the later postpartum are lacking. It is also unknown whether these relationships are independent of traditional diabetes-risk factors including family history of diabetes, previous history of GDM, age, ethnicity, and pre-pregnancy BMI. This knowledge can provide information to stratify GDM women with lower CRF and HS during pregnancy for early risk intervention and management to prevent diabetes and other metabolic health problems in the postpartum. This study investigated the associations of CRF and HS during pregnancy with metabolic health outcomes (glucose intolerance, MetS, insulin resistance), and CRP at 1-year postpartum in a cohort of women with GDM.
Methods
Study design and patient population
This is a secondary analysis of the MySweetheart trial (NCT02872974). Details of the MySweetheart trial have been previously described [37–39]. The trial tested the effect of an interdisciplinary lifestyle and psychosocial intervention on improving metabolic and mental health outcomes in women with GDM during pregnancy up to 1-year postpartum [37]. General eligibility criteria included women ≥ 18 years, diagnosed with GDM between 24–32 weeks gestational age (GA) according to the International Association of Diabetes and Pregnancy Study Groups and the American Diabetes Association (ADA) guidelines [1, 40]. Of the 211 participants included at baseline (105 were randomized to intervention and 106 to usual care), we included 179 participants who completed the 1-year postpartum follow-up in our analyses (Fig. 1). In this analysis, we pooled all participants together and adjusted for group allocation because predictors and outcomes in this analysis were similar in the intervention and usual care groups.Fig. 1. Flow chart of included study participants. CRF denotes cardiorespiratory fitness; HS denoted Handgrip Strength; CRP denotes c-reactive protein; HOMA-IR denotes Homeostatic Model Assessment for Insulin Resistance
GDM management and patient follow-up
Women in the usual care group were followed-up according to the current ADA and Endocrine Society guidelines [1, 41]. They were seen at 24–32 weeks GA by either a physician, or a diabetes-specialist nurse and followed-up until delivery. During these visits, they received information on GDM, specific recommendations regarding lifestyle changes and gestational weight gain (GWG) based on the 2009 recommendations of National Academy of Medicine (previously Institute of Medicine) [42]. Women were taught how to perform self-control of blood glucose both fasting and 2 h postprandial. Women also had one appointment with a registered dietician to receive individualized dietary advice [43]. They were advised to reduce sedentary behavior and engage in physical activity. At 1-year postpartum, patients underwent a 75 g oGTT and received general advice on lifestyle changes.
On top of the usual care, women randomized to the intervention had four clinical lifestyle visits during pregnancy and four lifestyle and psychosocial visits in the postpartum, two peer support group workshop (one in pregnancy and one in the postpartum), and a bimonthly lifestyle coach support, mostly through telemedicine. The full intervention description has been previously described [38]. These appointments focused on tailored behavioral and psychosocial strategies to improve diet, physical activity, mental health, and social support, and to improve adherence to GWG and weight retention recommendations. In the postpartum, continuous breastfeeding for at least 6-month was encouraged and aerobic and resistance physical activity for 150 min a week and resistance physical activity twice a week, all at a moderate intensity, were recommended.
Measures
Baseline demographic and health characteristics
We collected data on maternal socio-demographic characteristics including age, nationality/ethnic origin, and educational level during the baseline GDM visit at 24–32 weeks GA. Information on medical characteristics including previous history of GDM, family history of diabetes, gravida, parity, and family social support during pregnancy (living with partner or with support, yes/no) were extracted from participants’ medical charts.
Assessment of cardiorespiratory fitness (CRF) and muscular strength
We measured CRF (maximal oxygen uptake (VO_2_max) during pregnancy using the Chester Step test, a multistage submaximal exercise test, to assess aerobic fitness of participants [44]. The Chester Step test has demonstrated validity against indirect calorimetry to predict cardiorespiratory capacity [45]. Participants were asked to step up and down for a maximum of 10 min. The step rate started at 15 steps/min and increased every 2 min by 5 steps/min. The step rate was set by an audiotape and step height (15, 20 or 25 cm) was adapted to the patients’ physical characteristics and/or activity level. At the end of each 2 min stage, heart rate and rate of perceived exertion on Borg’s scale were recorded. The test was stopped when the rate of perceived exertion was ≥ 15, when the patient reached 80% of the estimated maximal heart rate (220-age) or showed signs of distress, or when the 10 min duration was reached (end of the test). Result from the Chester Step test were used to estimate the VO_2_max [45].
Handgrip strength (HS) was used as a proxy indicator of MS. It was assessed using the Jamar dynamometer during the baseline visit [46]. Participants were instructed on the proper use of the dynamometer and ensured that they were in the correct hand and wrist position during squeezing before the start of the test. Participants sat in a chair and squeezed the dynamometer as tightly as possible. Three measures were taken for each hand and the highest value of each hand was used for analysis. We calculated BMI-corrected HS by dividing handgrip strength values by pre-pregnancy body mass index (BMI) as recommended by previous studies [47, 48].
Assessment of metabolic health variables
Pre-pregnancy weight was extracted from participants’ medical charts or, if rarely missing, was self-reported. We measured height and weight at the baseline visit during pregnancy and weight again at 1-year postpartum to the nearest 0.1 cm and 0.1 kg with electronic scales (Seca®). BMI was expressed as a ratio of weight in kilograms to the square of height in meters (kg/m^2^). We extracted data on the need for glucose-lowering medical treatment during pregnancy (use of insulin and/or metformin) from maternal medical records. At 1-year postpartum, women underwent a 75 g oGTT with glucose and insulin sampling at 30 min intervals for 2-h. We then calculated insulin resistance/sensitivity, both by HOMA-IR (mostly hepatic insulin resistance) and MATSUDA (mostly total body insulin sensitivity) [49, 50]. Metabolic syndrome (MetS) status at 1-year was defined according to the International Diabetes Federation guidelines, which is based on either waist circumference > 80 cm or BMI ≥ 30 kg/m^2^ and at least two of the following cut-offs: triglycerides ≥ 1.7 mmol/l, HDL < 1.3 mmol/l, blood pressure ≥ 130/85 mmHg, FPG ≥ 5.6 mmol/l or type 2 diabetes mellitus [51]. As women are in a perinatal context, we use the definition with either the BMI or the waist circumference cut-off.
Glucose intolerance
We defined glucose intolerance (GI) at 1-year postpartum based on results of a 75-g oGTT (fasting plasma glucose (FPG) and 2 h glucose) test and HbA1c according to ADA criteria [1]. Women were classified as normal (FPG < 5.6 mmol/l or 2-h glucose < 7.8 mmol/l or HbA1c < 5.7%) or pathologic (FPG ≥ 5.6 mmol/l or 2-h glucose ≥ 7.8 mmol/l or HbA1c ≥ 5.7%) based on the oGTT results [1]. Of the 179 with valid laboratory data at 1 year postpartum, 119 had GI which included 54 women with prediabetes and 6 women with diabetes.
Measurement of C-reactive protein (CRP)
We measured CRP at 1-year postpartum in serum aliquots using a latex-enhanced immunoturbidimetric assay on a Cobas 8000 autoanalyser (Roche Diagnostics, Mannheim, Germany) with assay characteristics as reported by the manufacturer ((LOD (0.5–1), CV intra (3.7% at 0.840 mg/l) and CV total (inter) (4.0% at 0.840 mg/l)).
Statistical analyses
All statistical analyses were performed with Stata/SE 15.1 (StataCorp LLC, TX, USA). We presented demographic and other descriptive variables as means (± standard deviation) or percentages (%) where appropriate. Predictors (VO_2_max and BMI-corrected handgrip strength) and continuous outcome variables including HOMA-IR, MATSUDA, and CRP were normally distributed. We used paired t-tests to determine the changes between VO_2_max (CRF), BMI-corrected HS, CRP, and other metabolic health variables between the baseline at 24–32 weeks GA and the 1-year postpartum. Regression analyses were used to determine the relationship between VO_2_max and BMI-corrected HS with glucose intolerance, HOMA-IR, MATSUDA, MetS (both MetS-BMI and MetS-WC) and CRP at 1-year postpartum. In both analyses, we used two models; in model 1, we adjusted for group allocation and in model 2, we further adjusted for the following diabetes-risk factors (confounders): family history of diabetes, previous history of GDM, age, ethnicity, and pre-pregnancy BMI (except in the analyses between BMI-corrected HS where we did not adjust for BMI to avoid redundancy). In all analyses, predictors and outcomes were similar in both groups (intervention vs usual care), and the results, particularly the effect sizes, were similar when the analyses were restricted only to the usual care group or both groups. Therefore, to increase our sample size, we pooled both groups and adjusted for group allocation in all analyses. Reported beta-coefficients for all regression estimates were standardized. All statistical significances were two sided and accepted at p < 0.05.
Results
The mean age and pre-pregnancy BMI were 33.4 ± 5.6 years and 25.8 ± 5.4 kg/m^2^ respectively (Table 1). Among the 211 women included at baseline, 45% had a need for glucose-lowering treatment during pregnancy, 12% of women had a previous history of GDM and 64% had a family history of diabetes. Compared to the baseline visit, weight (-6.8 ± 5.7 kg, p < 0.001) and BMI (-2.5 ± 2.1 kg/m^2^, p < 0.001), were significantly decreased at 1-year postpartum, while fasting glucose (1.01 ± 1.6 mmol/l) increased (Table 2). In addition, CRP (4.02 ± 3.36 vs 2.99 ± 3.84 mg/l; p = 0.005), and HOMA-IR (3.59 ± 2.04 vs 3.24 ± 2.31; p = 0.007) were significantly lower at 1-year postpartum. The mean BMI-corrected HS at baseline was 2.29 ± 0.69 kg and CRF was 40.28 ± 15.02 mLO_2_/kg/min. Table 1. Baseline maternal socio-demographic of study participantsVariableAll (n = 211)n, %Age (year), mean ± SD33.4 ± 5.6Pre-pregnancy weight (kg) mean ± SD69.7 ± 15.8Pre-pregnancy BMI (kg/m^2^) mean ± SD25.8 ± 5.4Ethnicity/Nationality^a^ Switzerland62 (32.46) Rest of Europe and North America83 (43.46) Asia and Oceania14 (7.33) Africa23 (12.04) Latin America7 (3.66) Others2 (1.05)Education level Compulsory school incomplete^b^2 (0.95) Compulsory school achieved57 (27.01) High school19 (9.0) General and vocational education42 (19.91) University91 (43.13)Glucose-lowering treatment in pregnancy Yes90 (45.45) No108 (54.55)History of GDM Yes25 (11.84) No186 (88.15)Family history of diabetes^c^ Yes136 (64.45) No75 (35.55)Parity Zero120 (56.87) One57 (27.01) Two18 (8.53) ≥ Three16 (7.58)Gravida One88 (41.71) Two50 (23.7) ≥ Three73 834.6)Social support during pregnancy Yes191 (90.52) No20 (9.48)GDM denotes gestational diabetes mellitus; SD denotes standard deviation; BMI denotes body mass index^a^20 participants had missing data on ethnicity^b^In Switzerland, compulsory schooling lasts eleven years^c^Family history of diabetes consists of those with first-degree relationship of the participant (e.g., mother, father, brother, sister, daughter, son)Table 2. Changes in outcomes variables between pregnancy and at 1-year postpartumVariableNAt baseline 24-32GAAt 1-year postpartumMean differenceP-valueMean ± SDMean ± SDMean ± SDWeight (kg)17979.3 ± 14.572.4 ± 1.2-6.8 ± 5.7 < 0.001BMI (kg/m^2^)17929.4 ± 4.926.8 ± 5.6-2.5 ± 2.1 < 0001Fasting glucose (mmol/l)1534.9 ± 0.45.9 ± 1.61.01 ± 1.6 < 0.001HOMA-IR1403.59 ± 2.043.24 ± 2.31-0.34 ± 1.500.007CRP (mg/l)1504.02 ± 3.362.99 ± 3.84-1.03 ± 3.530.005BMI denotes Body mass index, CRP denote c-reactive proteinHOMA-IR denotes Homeostatic Model Assessment for Insulin Resistance
Longitudinal associations between CRF with insulin resistance, metabolic syndrome, inflammation, and glucose intolerance
Table 3 shows the longitudinal associations between CRF during pregnancy with insulin resistance, metabolic syndrome, inflammation, and glucose intolerance at 1-year postpartum. We observed a significant association between higher CRF during pregnancy and a lower risk of glucose intolerance at 1-year postpartum (β = -5.53, p = 0.047). Similarly, a higher CRF was associated with a lower risk of the MetS-WC (β = -0.59, p = 0.009), lower insulin resistance (HOMA-IR: β = -1.42, p = 0.019) and with increased insulin sensitivity (MATSUDA: β = 0.99, p = 0.017). These observed associations were not significant when we additionally adjusted for confounders including family history of diabetes, previous history of GDM, age, ethnicity and pre-pregnancy BMI. Table 3. Relationship between cardiorespiratory fitness during pregnancy with insulin resistance, inflammation, metabolic syndrome, and glucose intolerance at 1-year postpartumVariableBeta coefficient95% CIP valueModel 1 Glucose intolerance, yes-5.53-10.9, -0.070.047 HOMA-IR-1.42-2.60, -0.240.019 MATSUDA0.990.17, 1.810.017 MetS-BMI-4.80-9.76, 0.160.058 MetS-WC-0.59-10.4, -1.510.009 CRP-0.56-1.27, 0.140.120Model 2 Glucose intolerance, yes-1.20-5.98, 3.520.616 HOMA-IR-0.25-1.18, 0.670.585 MATSUDA0.07-0.74, 0.890.863 MetS-BMI-1.00-5.42, 3.410.653 MetS-WC-1.51-5.54, 2.510.456 CRP-0.3-9.68, 0.280.280Glucose intolerance at 1 year postpartum defined as FPG ≥ 5.6 mmol/l or 2 h glucose ≥ 7.8 mmol/l or HbA1c ≥ 5.7%MetS denotes metabolic syndromeWC denotes waist circumferenceBMI denotes body mass indexCRP denote c-reactive proteinHOMA-IR denotes Homeostatic Model Assessment for Insulin ResistanceModel 1: Regression model is adjusted for group allocationModel 2: Regression model is adjusted for group allocation, family history of diabetes, previous history of GDM, age, ethnicity and pre-pregnancy BMI
Longitudinal associations between BMI-corrected HS and insulin resistance, metabolic syndrome, inflammation and glucose intolerance
In Table 4, we investigated the longitudinal associations between BMI-corrected HS during pregnancy and metabolic health outcomes at 1-year postpartum. Although we did not observe significant association between BMI-corrected HS during pregnancy and glucose intolerance at 1-year postpartum, higher BMI-corrected HS was associated with lower insulin resistance (HOMA-IR) (β = -0.09, p = 0.039), MetS-BMI (β = -0.38, p < 0.001), CRP (β = -0.04, p = 0.035) and with increased insulin sensitivity (MATSUDA: β = 0.10, p < 0.001) at 1-year postpartum even after adjustment for confounders (model 2). While we observed significant inverse associations between HS with MetS-WC (β = -0.33, p = 0.001), this association was not independent of the confounders. Table 4. Relationship between BMI-corrected handgrip strength during pregnancy with insulin resistance, inflammation, metabolic syndrome, and glucose intolerance at 1-year postpartumVariableBeta coefficient95% CIP valueModel 1 Glucose intolerance, yes-0.10-0.32, 0.100.329 HOMA-IR-0.08-0.12, -0.03 < 0.001 MATSUDA0.080.04, 0.12 < 0.001 MetS-BMI-0.43-0.64, -0.22 < 0.001 MetS-WC-0.33-0.52, -0.130.001 CRP-0.03-0.05, -0.0010.038Model 2 Glucose intolerance, yes-0.25-0.55, 0.030.087 HOMA-IR-0.09-0.15, -0.030.003 MATSUDA0.100.05, 0.15 < 0.001 MetS-BMI-0.38-0.67, -0.090.010 MetS-WC-0.25-0.53, 0.010.068 CRP-0.04-0.08, -0.0030.035Glucose intolerance at 1 year postpartum defined as FPG ≥ 5.6 mmol/l or 2 h glucose ≥ 7.8 mmol/l or HbA1c ≥ 5.7%MetS denotes metabolic syndromeWC denotes waist circumferenceBMI denotes body mass indexCRP denote c-reactive proteinHOMA-IR denotes Homeostatic Model Assessment for Insulin ResistanceModel 1: Regression model is adjusted for group allocationModel 2: Regression model is adjusted for group allocation, family history of diabetes, previous history of GDM, age and ethnicity
Discussion
In this cohort of women with GDM followed during pregnancy up to 1-year postpartum, increased cardiorespiratory fitness (CRF) during pregnancy was protective of glucose intolerance at 1-year postpartum but this association was not independent of classical diabetes risk factors. Both CRF and BMI-corrected HS during pregnancy were associated with lower hepatic insulin resistance (HOMA-IR), increased whole body insulin sensitivity (MATSUDA), and a lower risk of metabolic syndrome at 1-year postpartum, while HS alone was further related to lower CRP. After adjusting for classical diabetes risk factors, the associations between HS with lower metabolic syndrome (Mets-BMI), hepatic insulin resistance (HOMA-IR), CRP and increased whole body insulin sensitivity (MATSUDA) remained significant. Our results demonstrate that improving CRF but particularly HS during pregnancy can improve adverse metabolic health outcomes in women after GDM.
CRF and HS are well-established predictors of metabolic health [28–30] including lower prevalence of the metabolic syndrome and type 2 diabetes and lower risk of CVD in the general population. However, the long-term benefits of prenatal exercise interventions largely remain inconsistent and prospective data linking CRF and HS with insulin resistance, glucose intolerance and metabolic outcomes in women with GDM that extend to the later postpartum were lacking. Our findings demonstrate these benefits in women with a history of GDM who have an increased risk of diabetes and CVD [52] in the postpartum period.
In our cohort of women with GDM, higher CRF during pregnancy was associated with lower risk of glucose intolerance, lower MetS, lower HOMA-IR and increased Matsuda at 1-year postpartum. However, these associations were attenuated after adjusting for classical diabetes risk factors including family history of diabetes, previous history of GDM, age, ethnicity, and pre-pregnancy BMI. These results suggest that the role of CRF in improving postpartum metabolic risk is less pronounced when pre-existing risk factors are accounted for. Previous studies associating higher CRF to improved glucose metabolism [22–27] and lower levels of chronic inflammation [14] in non-pregnant populations are consistent with our findings. Our results also align with studies that suggests that exercise intervention before and during pregnancy improves metabolic health included the development of GDM [31–35]. Notably, these studies either adjusted for age, BMI or family history of diabetes but not the diabetes risk factors.
BMI-corrected HS [47, 48] during pregnancy was significantly associated with lower prevalence of MetS-BMI, lower HOMA-IR and higher MATSUDA and these relationships were independent of classical diabetes risk factors. These results are consistent with those of an observational study conducted in the late postpartum in women with GDM where higher HS was associated with improved glucose tolerance and features of MetS in women with GDM [36]. Additionally, HS was inversely associated with CRP, even after adjusting for classical diabetes risk factors. Our findings align with the reported inverse association between HS and low-grade systemic inflammation in the literature [11–13].
The observed association of CRF and HS with glucose intolerance, MetS, insulin resistance and inflammation could be explained by the following mechanisms. Higher CRF is linked to improved mitochondrial efficiency, enhanced glucose uptake, and reduced hepatic insulin resistance [53, 54] through the release of myokines including interleukin-6, which are known to have anti-inflammatory and insulin-sensitizing effects [55, 56]. Additionally, exercise is known to increase muscle fiber hypertrophy and mitochondrial biogenesis, both of which lead to energy utilization thereby reducing metabolic risk [57]. It has been shown that improvements in endothelial function and vascular elasticity due to exercise enhance insulin delivery to peripheral tissues, promoting glucose uptake and metabolic balance [58]. Regarding inflammation, CRF is known to lower systemic inflammation through modulating autonomic function by enhancing parasympathetic activity [59]. The role of skeletal muscle in glucose homeostasis, where increased muscle mass influences insulin-stimulated glucose uptake and reduced hepatic insulin resistance could explain the relationship between HS and improved metabolic health observed in our cohort [60]. Particularly, skeletal muscle acts as an endocrine organ, secreting myokines such as irisin and brain-derived neurotrophic factor, which have been implicated in promoting insulin sensitivity and reducing inflammation [61, 62]. Taken together, these mechanisms show that HS is a critical, modifiable factor in improving postpartum metabolic health especially in women with GDM [52].
The longitudinal associations of CRF and HS with metabolic health outcomes in this study can provide additional information to risk stratify GDM women with lower CRF and HS during pregnancy for early intervention and management to prevent diabetes and other adverse metabolic health problems in the postpartum. Our results also highlight the clinical and public health need to enlarge the clinical follow-up to include physical activity and ideally fitness assessments into care and metabolic follow-up for women with prior GDM during and after pregnancy. While CRF may offer some benefits, our results suggest that HS could be more effective in improving metabolic outcomes. In analogy to the best synergistic benefit of integrating both aerobic and resistance training in people with type 2 diabetes, there is the need to promote structured exercise programs that integrate both training methods to optimize postpartum metabolic health for women after pregnancy.
To our knowledge, this is the first study to investigate the prospective longitudinal associations of CRF and HS with glucose intolerance, hepatic insulin resistance, whole body insulin sensitivity MetS and CRP in metabolically high-risk women with GDM at 1-year postpartum. It also investigated the role of traditional diabetes-risk factors including family history of diabetes, previous history of GDM, age, ethnicity, and pre-pregnancy BMI in the relationship between CRF and HS with metabolic health. In addition, all outcome measures including CRF (VO_2_max), and HS (Jamar dynamometer for handgrip strength) were objective and validated. We also adjusted for pre-pregnancy BMI in our assessment of HS, since BMI during pregnancy does not reflect purely maternal fat or muscle mass which is more directly related to muscle strength. Limitations of this study include the lack of validated tests for assessing physical fitness in women during pregnancy, we thus used Chester step test and handgrip strength as proxy indicators for CRF and HS respectively. In addition, we pooled both intervention and control participants together to increase the sample size, since the value of predictors and outcomes and the effect sizes were similar in both groups. We also adjusted for group allocation in all analyses.
Conclusions
In this longitudinal cohort of women with GDM, followed during pregnancy until 1-year postpartum, both CRF and HS during pregnancy were associated with improved hepatic insulin resistance, whole body insulin sensitivity and MetS-WC at 1-year postpartum. The associations of HS with lower hepatic insulin resistance, increased whole body sensitivity and metabolic health including lower prevalence of MetS and lower CRP were independent of classical diabetes risk factors including family history of diabetes, age, ethnicity, and pre-pregnancy BMI. Higher CRF was associated with lower risk of glucose intolerance. Our data suggest that integrating easy-to-do physical fitness tests such as handgrip strength (hand grip strength dynamometer or chair stand test) in future intervention studies and in clinical care could be beneficial for these women. Studies should also investigate whether and what kind of exercise interventions in the perinatal period can improve longer term outcomes in this population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Blumer I, Hadar E, Hadden DR, Jovanovič L, Mestman JH, Murad MH, Yogev Y. Diabetes and pregnancy: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2018;103(11):4042. 10.1210/jc.2018-01939.10.1210/jc.2013-2465 PMC 899809524194617 · doi ↗ · pubmed ↗
- 2Arditi C, Puder J, Vial Y, Hagon-Traub I, Burnand B. Grossesse et diabète: Prise en charge multidisciplinaire du diabète: Recommandations pour la pratique clinique. 2018;14:2085.30427603 · pubmed ↗
- 3Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, Fruchart JC, James WP, Loria CM, Smith SC Jr; International Diabetes Federation Task Force on Epidemiology and Prevention; Hational Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; International Association for the Study of Obesity. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemi · doi ↗ · pubmed ↗
- 4Crescenzo R, Bianco F, Mazzoli A, Giacco A, Liverini G, Iossa S. Mitochondrial efficiency and insulin resistance. Front Physiol. 2015;5:512.10.3389/fphys.2014.00512 PMC 428351725601841 · doi ↗ · pubmed ↗
- 5Merz KE, Thurmond DC. Role of Skeletal Muscle in Insulin Resistance and Glucose Uptake. Compr Physiol. 2020;10(3):785–809. 10.1002/cphy.c 190029.10.1002/cphy.c 190029 PMC 807453132940941 · doi ↗ · pubmed ↗