Combinatorial BCL2/BCL2L1 expression predicts clinical response to ruxolitinib in myelofibrosis
Giacomo Coltro, Viola Videschi, Francesca Gesullo, Federica Violi, Manjola Balliu, Alessandro M. Vannucchi, Paola Guglielmelli

TL;DR
High baseline expression of BCL2 and BCL2L1 genes predicts better response to ruxolitinib in myelofibrosis patients.
Contribution
A combinatorial score of BCL2 and BCL2L1 gene expression improves prediction of ruxolitinib response in myelofibrosis.
Findings
Baseline BCL2 and BCL2L1 expression is significantly higher in responders to ruxolitinib.
A combinatorial score of BCL2 and BCL2L1 outperforms individual genes in predicting treatment response.
Responders show BCL2 down-regulation when treatment response is lost.
Abstract
Myelofibrosis is characterized by aberrant JAK/STAT signaling, with approved therapy including the JAK inhibitor ruxolitinib. Preclinical evidence implicates BCL-2 family proteins in MF pathogenesis and therapeutic response. Here, we evaluated baseline and on-treatment expression of BCL2, BCL2L1 (encoding BCL-xL), and MCL1 in 19 myelofibrosis patients receiving ruxolitinib. Quantitative PCR fold-change (FC) values, relative to healthy donors, revealed reduced baseline BCL2 (mean FC 0.15) and MCL1 (0.32) expression, with BCL2L1 showing a non-significant trend toward upregulation. Baseline BCL2 and BCL2L1 expression was significantly higher in patients achieving spleen response (responders; n = 7) compared to non-responders (BCL2: 0.30 vs 0.07, p = 0.0130; BCL2L1: 2.73 vs 0.52, p = 0.0096). Logistic regression confirmed both as independent predictors of response. We derived a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
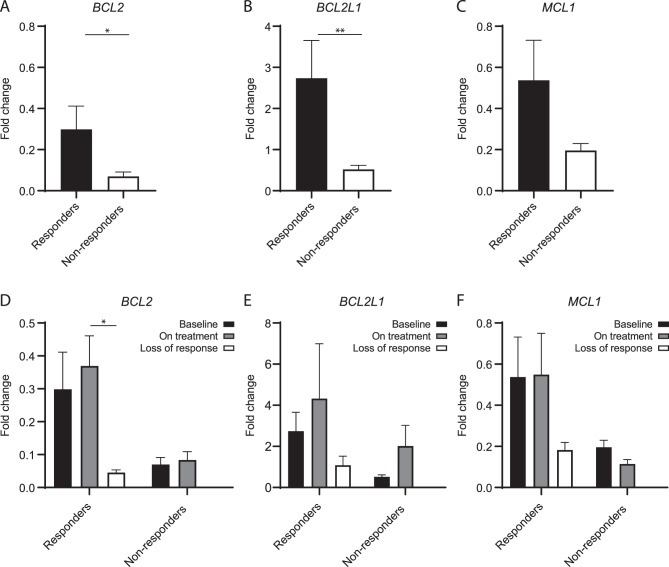 Figure 1
Figure 1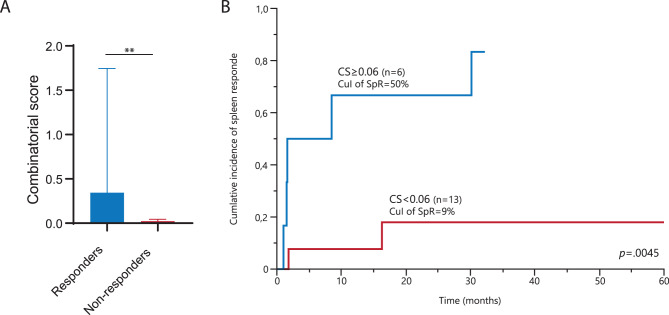 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMyeloproliferative Neoplasms: Diagnosis and Treatment · Acute Myeloid Leukemia Research · Platelet Disorders and Treatments
To the editor,
Myelofibrosis (MF) is driven by dysregulation of the JAK/STAT pathway, which is critically involved in cell growth, survival, and differentiation [1]. This dependence prompted the development of JAK inhibitors (JAKi), with ruxolitinib (Rux) being the first approved. Emerging evidence implicates the BCL-2 family proteins in MF development and treatment response [2, 3], supported by preliminary evidence of efficacy of combining JAK2 and BCL-xL inhibition [4].
Herein, we investigated baseline and on-treatment expression levels of BCL2, BCL2L1 (encoding BCL-xL) and MCL1 in 19 MF patients (11 primary MF, 8 secondary MF) treated with Rux. Gene expression was assessed by qPCR on granulocyte cDNA, and expressed as fold-change (FC) using the Ct (2−ΔΔCt) method (additional information in Supplemental Material).
Compared to healthy donors, baseline expression of BCL2 and MCL1 was lower in Rux-naïve patients, with mean FCs 0.15 (SEM, 0.05) and 0.32 (SEM, 0.08), respectively. Conversely, BCL2L1 showed a trend for up-regulation with mean FC 1.33 (SEM, 0.41). No significant correlations were noted between baseline expression and clinical and molecular characteristics, except for higher BCL2L1 expression in EZH2-mutated patients.
Median Rux starting dose was 30 (range, 10–40) mg daily. After a median Rux exposure of 67 (6–121) months, 7 (37%) patients achieved spleen response (“responders”). Upon correlation analysis, BCL2 and BCL2L1 were significantly more expressed in responders, with mean FC values 0.30 vs 0.07 (p = 0.0130) and 2.73 vs 0.52 (p = 0.0096) (Fig. 1A-C). A trend was observed for MCL-1 (mean FC, 0.54 vs 0.20; p = 0.0572). Firth’s logistic regression confirmed that BCL2 and BCL2L1 FCs independently predicted response, with respective odds-ratio [OR] of 5.2 (p = 0.0337) and 1.4 (p = 0.0096).Fig. 1A-C. Bar plot of the relative expression of BCL2 (A), BCL2L1 (B), and MCL1 (C) calculated as Fold change at baseline among responder (n = 7) and non-responder patients (n = 12). D-F. Bar plot of the relative expression of BCL2 (D), BCL2L1 (E), and MCL1 (F) calculated as Fold change at baseline-best response-response loss for responder patients and at baseline-on treatment for non-responder patients. Graphs are presented as the mean and SEM of normalized expression values. Statistical significance was determined with ANOVA; *p < 0.05, **p < 0.005, ***p < 0.0005, ****p < 0.0001. Abbreviations: SEM, standard error of the mean
Next, we incorporated baseline BCL2 and BCL2L1 expression into a combinatorial score (CS) resulting from the product of respective FCs (FC^BCL-2^ * FC^BCL2L1^). The median CS for responders and non-responders was 0.34 (0.03–4.78) and 0.02 (0–0.32), respectively (p = 0.0035) (Fig. 2A). The CS outperformed individual gene expression in predicting Rux response, confirmed in logistic regression analysis (OR, 7.5; p = 0.0028). ROC analysis identified 0.06 as the optimal CS cut-off value that was associated with higher probability of Rux response (OR 3.3; p = 0.0037), with a cumulative incidence of 24-week response of 50% vs 9% (p = 0.0045) (Fig. 2B).Fig. 2A. Bar plot of the combinatorial score (CS) among responder (n = 7) and non-responder patients (n = 12). B. Cumulative incidence of spleen response according to the value of the CS: ≥0.06 (n = 6) or < 0.06 (n = 13). Graphs are presented as the mean and SEM of normalized expression values. Statistical significance was determined with ANOVA; *p < 0.05, **p < 0.005, ***p < 0.0005, ****p < 0.0001. Abbreviations: CS, combinatorial score; CuI, cumulative incidence; SEM, standard error of the mean; SpR, spleen response
Finally, we prospectively assessed changes in gene expression during Rux treatment (Fig. 1D-F). We found no significant difference between baseline and on-treatment, possibly due to the small sample size. By comparing gene expression of responders at the time of best versus loss of response, we observed a trend for down-regulation for all the three genes at the time of response loss, with a statistical significance for BCL2 (mean FC 0.08 vs 0.37; p = 0.0419). Of 15 patients with longitudinal molecular data available, one non-responder acquired a frameshift ASXL1 mutation, while one responder developed a non-stop ASXL1 mutation at response loss.
In summary, we evaluated the expression kinetics and predictive value of BCL2, BCL2L1 and MCL-1 in a cohort of MF patients treated with Rux. We developed a simple CS that accurately identified responder patients. Recently, Waclawiczek et al. presented a flow cytometry-based “Mediators of Apoptosis Combinatorial Score” (MAC-Score) including the ratio of BCL2, BCL-xL, and MCL1 protein expression in leukemic stem cells [5]; the MAC-Score predicted clinical response to azacitidine/venetoclax with increased event-free survival. Overall, these findings support the potential role of BCL-2 family member expression as predictor of treatment response.
Finally, we observed changes in BCL2 family protein expression during Rux treatment. The small numbers prevented us from obtaining statistical significance, with the exception for BCL2 expression drop at response loss. Our findings partially contrast with previous data showing higher expression of BCL2L1 and MCL1 in refractory/relapsed patients [6]. The counterintuitive kinetics –especially for BCL2– may be ascribed to an increased dependence of cell survival on BCL-2 pathway following inhibition of the JAK2/STAT or other pathways. It can also be speculated that the mRNA levels may not accurately reflect changes at the protein level [7]. Finally, we reported the acquisition of two ASXL1 mutations during Rux treatment. Recently, mutant ASXL1 was linked to epigenetic upregulation of BCL2 expression leading to enhanced sensitivity to venetoclax and azacitidine [8]. Interferon-α (IFNα) has also been reported to modulate BCL-2 family protein expression, and its combination with Rux has shown efficacy in MF, thus providing a rationale to explore combined strategies [9, 10].
In addition to their anti-proliferative and pro-apoptotic effects, BCL-2 family inhibitors may also exert relevant anti-inflammatory and immunomodulatory activity. As JAKi suppress cytokine-driven inflammation (a hallmark of MF pathogenesis), combined inhibition could yield synergistic benefit by reducing inflammatory stress and reinforcing apoptotic priming [11].
We acknowledge study limitations, including retrospective design and small study cohort. Notwithstanding, these preliminary data suggest that BCL2, BCL2L1 and MCL-1 expression may correlate with Rux response. Of note, a BCL2/BCL2L1-based CS effectively predicted Rux response. Further studies are needed to confirm and expand our data.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1