Medication Use by Older Adults with Frailty: A Scoping Review
Rishabh Sharma, Tanaya Sharma, Brent McCready-Branch, Arshia Chauhan, Caitlin Carter, SooMin Park, Imra Hudani, Prapti Choudhuri, Tejal Patel

TL;DR
This review explores how medication use affects older adults with frailty, focusing on inappropriate medications and polypharmacy.
Contribution
The study provides a comprehensive overview of medication use patterns and risks in frail older adults across multiple countries.
Findings
Polypharmacy and hyper-polypharmacy are significantly more common in individuals with frailty.
Potentially inappropriate medications are prevalent among frail older adults, with wide variability in reported rates.
Frailty prevalence varies greatly across studies, indicating a need for standardized definitions and assessments.
Abstract
Frailty among older adults heightens their risk of negative health outcomes, and medication use plays a major role in this increased vulnerability. Various aspects of medication use elevate the risk of poor outcomes in individuals with frailty. The current scoping review was designed to explore medication use in older adults with frailty in primary care, focusing on the prevalence of potentially inappropriate medications (PIMs), polypharmacy, medication adherence, and their role in contributing to adverse drug events. This scoping review was conducted using the Arksey and O’Malley, supplemented by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Extension for Scoping Reviews (PRISMA-ScR) guidelines. A search of the literature was conducted from inception to November 2023 in Ovid EMBASE, PubMed (MEDLINE), Scopus, EBSCOhost CINAHL, and Ovid International…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
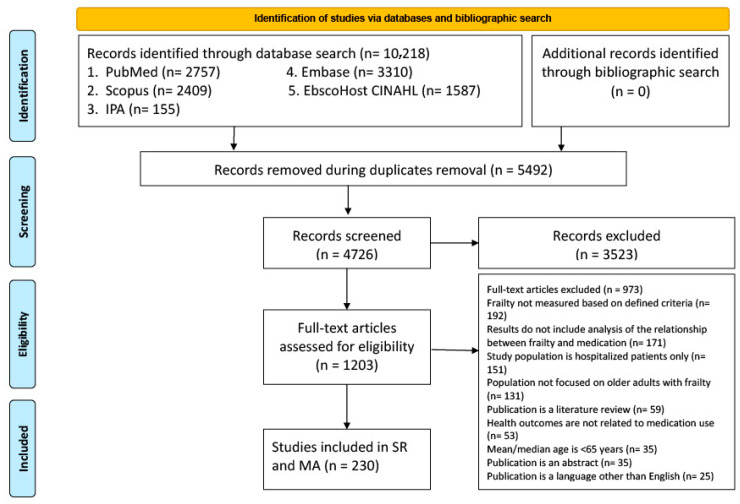 Figure 1
Figure 1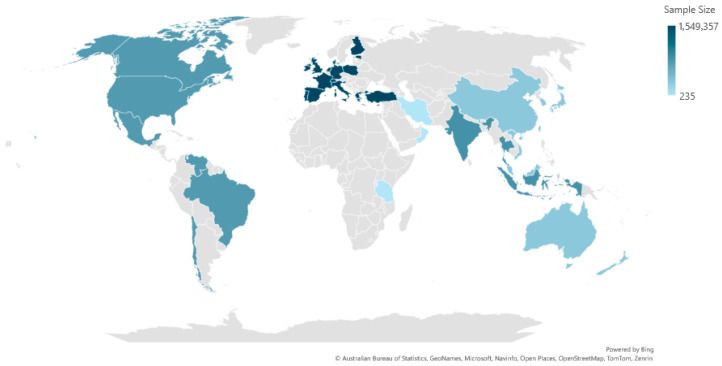 Figure 2
Figure 2- —Canadian Frailty Network
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFrailty in Older Adults · Pharmaceutical Practices and Patient Outcomes · Medication Adherence and Compliance
1. Introduction
The global population is aging rapidly. By 2030, one in six people worldwide will be aged 60 or older, from 1 billion in 2020 to 1.4 billion. By 2050, this number is expected to reach 2.1 billion, with those aged 80 years or over tripling to 426 million [1]. In Canada, the aging trend is accelerating as baby boomers move into the 65+ age group. Currently, over 800,000 Canadians are 85 or older, a number projected to triple by 2050 [2]. This demographic shift presents significant implications for healthcare systems, economies, and societies at large. Older adults with comorbidities such as hypertension, diabetes, cardiovascular diseases, and stroke are at a higher risk of morbidity and mortality [3]. Multimorbidity—defined as having two or more chronic conditions—is increasingly common, with 8.3% of Canadians reporting three or more in 2021, up from 7.5% in 2015 [4,5]. There are several challenges that are associated with aging, one of the most significant contributors being the increased risk of frailty [6].
Currently, there is no clear consensus on the definition of frailty. A widely accepted definition, proposed by Fried et al., describes frailty as “a state of age-related physiological vulnerability resulting from impaired homeostatic reserve and a reduced capacity of the organism to withstand stress” [7]. Increasingly, researchers acknowledge the multifactorial nature of frailty [8]. A recent integral conceptual model by Gobbens et al. defines frailty as a dynamic state affecting an individual who experiences losses in one or more domains of human functioning (physical, psychological, and social), caused by various influences, which increases the risk of adverse outcomes [9]. Frailty can be described through various lenses, including physical, psychological, and social aspects [10].
Frailty is commonly classified into three categories: robust, pre-frail, and frail [7]. Individuals may move between these stages depending on various factors. Frailty is often worsened by multiple medication use, poor nutrition, inactivity, and social isolation [11]. Older adults with frailty are more vulnerable to serious health outcomes from minor illnesses or events, such as influenza or falls, and face higher risks of hospitalization, long-term care, and mortality [12]. These issues can significantly affect daily functioning and increase dependence on caregivers, impacting both the individual’s and their family’s quality of life [13]. Several tools are available to assess frailty, helping to guide clinical care and identify those at risk. Common tools include the Frailty Index (FI), which evaluates accumulated health deficits; the Fried Frailty Phenotype, based on physical markers like weight loss and weakness; and the Clinical Frailty Scale (CFS), a visual rating of fitness levels. Other tools include the Geriatric 8 (G8), Edmonton Frail Scale (EFS), Tilburg Frailty Indicator (TFI), and PRISMA-7, each assessing various physical, psychological, or social dimensions [14]. These tools vary in complexity and focus. With the increases in the aging population in Canada, it is important to monitor this population due to its impact on quality of life, ability to age at home, and increased risk of mortality [15,16,17].
Individuals with frailty experience heightened sensitivity to medication, which can increase the chances for adverse effects even at regular dosages [18,19,20]. Furthermore, use of polypharmacy, potentially inappropriate medications (PIMs), medication adherence, and errors impact health outcomes [21]. A systematic review and meta-analysis by Toh et al. reported that among frail older adults (synthesized data from 66 studies, involving 167,888 participants), polypharmacy (≥5 medications) had a pooled prevalence of 59%, and hyper-polypharmacy (≥10 medications) was observed in 22% of cases [19]. Additionally, cognitive impairments may cause difficulties in remembering doses, while physical limitations can make tasks like opening pill bottles challenging, further complicating medication management [22]. Finally, medication use in this population is further complicated by age-related changes such as altered drug metabolism, and reduced renal and liver function, all of which increase the risk of medication toxicity and treatment-related harm [20].
In recent years, there has been an increase in both the number and variety of studies exploring the relationship between medication use and frailty. Researchers are delving into various aspects, such as how specific medications might contribute to or alleviate frailty, the impact of polypharmacy, and the interplay between different drug classes and frailty risk. Despite this expanding body of research, a comprehensive review that synthesizes all these findings and provides a holistic understanding of the concepts is still missing. This scoping review was conducted to explore and summarize the existing research on medication use in community-dwelling older adults with frailty.
2. Materials and Methods
To conduct this scoping review, we followed the five-stage framework proposed by Arksey and O’Malley [23], as described below. Additionally, we utilized the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Extension for Scoping Reviews (PRISMA-ScR) to structure and present our results comprehensively (Supplementary Table S1) [23,24].
2.1. Identifying the Research Question
This scoping review aims to comprehensively explore medication use patterns and outcomes among older adults with frailty in primary care settings. The primary objectives are as follows:
- To analyze medication use in older adults with frailty by examining the prevalence of PIMs, polypharmacy, capacity for medication management, adherence to prescribed regimens, medication errors, and associated health outcomes.
- To provide recommendations for addressing medication-related issues in this population by detailing available tools (such as medication review instruments) and processes (including deprescribing strategies) that can aid in identifying and managing these problems.
2.2. Identifying the Relevant Studies
A comprehensive search strategy was designed and implemented by an experienced librarian (CC) across five databases—PubMed (MEDLINE); Ovid Embase; Scopus; EBSCOhost CINAHL; and Ovid International Pharmaceutical Abstracts—from inception to 3 November 2023. The core search concepts included in the search strategy were frailty; elderly; and medication use. All database search strategies contained keywords and associated synonyms for each of these core concepts, as well as relevant subject headings, if the database contained an index of controlled vocabulary. Search terms were linked with Boolean operators (AND/OR) and keywords were limited to the title and abstract fields only. Truncation was applied to several keywords and the proximity or adjacency search operator was utilized, based on the database’s functionality. All search strategies were limited to English only, and conference abstracts were removed from the Ovid Embase search results. The complete search strategies for each database can be found in Supplementary Table S2. The search results were exported into Covidence (Veritas Health Innovation, Melbourne, Australia) and duplicates were removed.
2.3. Study Selection
Eligibility criteria for study inclusion were developed using the Evidence-Based Medicine PICO framework (Population, Intervention or Exposure, Comparison or Control, Outcomes), focusing on community-dwelling frail older adults (mean or median age ≥ 65 years). Studies were included if they assessed frailty using validated criteria and examined any aspect of medication use, such as polypharmacy, PIMs, medication errors, deprescribing, medication management, or medication-related health outcomes. Eligible study designs included observation (cohort, cross-sectional, case–control) and interventional (randomized-controlled trials (RCTs), pre–post) studies. Articles were excluded if they were not published in English, were expert opinions, case reports, abstracts, literature reviews, and protocols without data analysis, involved non-human participants, or were conducted in institutional settings such as hospitals or long-term care. A two-stage screening process was conducted by a team of seven research assistants (RS, TS, BMB, AC, SP, IH, PC). In the first stage, titles and abstracts were independently reviewed by two independent research assistants. In the second stage, full-text articles were independently reviewed by two independent research assistants, with disagreements resolved through discussion with a third reviewer (TP). Weekly team meetings were held to ensure consistency and resolve discrepancies.
2.4. Data Charting
We created a standard Microsoft^®^ Excel^®^ spreadsheet, specifically the Office 365 ProPlus Version 1906 form, in advance to extract essential information from the articles. The following data were abstracted: study design (qualitative/quantitative studies, RCTs, non-RCTs, retrospective studies), location of the study (country and setting such as primary care), primary and secondary objectives, sample size, type and measure of frailty, population demographics (age, gender, number of medications, number of medical conditions, severity of frailty, baseline medication use, etc.), medication use interventions, study outcomes, results, and additional comments. Data abstraction was independently completed by two reviewers from the team of seven research assistants. The extracted data were then compared by one more reviewer from the team of research assistants who had not performed data extraction for the study to ensure accuracy, consistency, and completeness.
2.5. Collating, Summarizing, and Reporting the Results
To address the first primary objective, we employed a narrative synthesis approach. We began by developing a preliminary synthesis, grouping studies that focused on similar concepts, such as the prevalence of frailty using different criteria, the prevalence of PIMs, and the prevalence of polypharmacy, into a tabular format. Using Excel, we created tables to explore relationships between medication use, polypharmacy, hyper-polypharmacy, and frailty. Additionally, we reported the results of any type of statistical analyses conducted to investigate the association between medication use and frailty in these studies.
For the second objective, we detailed any interventions or recommendations for addressing medication-related issues in this population. These included descriptions of available tools, such as medication review instruments, and processes, including deprescribing strategies, that can aid in identifying and managing these problems.
3. Results
A total of 10,218 references were identified across various electronic databases (see Figure 1, PRISMA Flow diagram). After removing 5492 duplicate entries, 4726 titles and abstracts were screened based on the study’s predefined inclusion and exclusion criteria. Of these, 1203 articles were selected for full-text review, resulting in 230 eligible studies. Out of 230 studies, 223 are unique, indicating that 7 studies are overlapping or use the same population data.
3.1. Characteristics of Included Studies
The 223 studies were conducted across 39 countries [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156,157,158,159,160,161,162,163,164,165,166,167,168,169,170,171,172,173,174,175,176,177,178,179,180,181,182,183,184,185,186,187,188,189,190,191,192,193,194,195,196,197,198,199,200,201,202,203,204,205,206,207,208,209,210,211,212,213,214,215,216,217,218,219,220,221,222,223,224,225,226,227,228,229,230,231,232,233,234,235,236,237,238,239,240,241,242,243,244,245,246,247,248,249,250,251,252,253,254]. The characteristics of the included studies are summarized in Supplementary Table S3. The studies have been divided into different regions as follows: 41 studies were conducted in North and South America ([25,31,32,37,45,50,53,57,64,69,71,74,75,77,84,86,90,98,104,108,109,112,115,123,126,132,134,143,162,164,167,170,175,195,196,210,216,223,224,244]), 6 studies in the Middle East ([34,106]), 106 studies in Europe ([26,27,28,29,30,33,35,37,39,41,43,47,51,55,59,60,62,65,66,72,76,78,79,81,85,91,96,99,100,103,105,106,107,111,114,116,117,118,119,120,121,124,125,127,130,131,133,135,136,137,142,146,147,150,151,152,153,154,156,158,159,160,161,165,166,168,173,177,179,180,181,183,185,187,188,190,192,194,197,200,203,204,205,206,208,209,211,213,217,219,225,226,229,233,235,238,239,241,242,243,245,247,250,251,254]), 11 studies in Southeast Asia ([42,128,138,140,145,155,191,199,212,220,246]), 56 studies in the Western Pacific ([36,40,44,46,58,61,63,67,68,80,82,83,87,88,92,95,102,113,122,129,139,144,149,157,163,169,171,172,176,178,186,189,193,198,201,202,207,214,215,218,221,230,231,232,234,236,237,240,248,249,252,253]), 1 study in Africa [89], and 2 studies in Australia and the USA ([70,93]). Figure 2 illustrates the heatmap showing the distribution of studies collected in this scoping review by region and sample size. A total of 202 studies included both women and men ([25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,41,42,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,140,141,142,143,144,145,146,147,148,150,151,152,153,154,155,156,157,158,160,161,162,163,165,166,167,168,169,170,171,172,173,174,175,176,177,178,179,180,181,182,183,185,186,187,188,189,190,191,192,193,194,195,196,197,198,199,200,201,202,203,204,205,206,207,208,209,210,211,212,213,215,216,217,219,220,221,224,225,226,227,228,229,230,231,232,233,234,235,236,237,238,239,240,241,242,243,244,245,246,247,248,249,250,251,252,253,254]); however, seven studies have only included female populations ([40,149,164,186,223,224,249]) and ten studies only included male populations ([43,63,82,83,139,159,184,214,218,222]). Among the studies, 120 were cross-sectional studies ([25,27,28,29,30,31,32,34,36,38,41,42,44,45,50,55,58,61,64,65,68,69,71,72,73,75,77,78,81,84,86,89,94,95,99,100,102,105,107,109,110,111,112,113,115,123,124,125,128,130,131,133,138,139,140,142,143,144,145,148,149,151,154,155,158,160,161,162,167,171,173,175,177,179,180,182,185,187,189,192,193,196,197,198,199,200,201,203,204,206,208,212,213,214,215,216,217,218,219,221,224,225,228,229,231,232,233,234,239,240,242,243,244,247,248,250,251,252,253]), 31 studies were prospective cohort studies, ([40,46,51,57,63,66,67,82,83,85,91,121,132,134,156,157,164,170,178,184,186,188,202,205,207,211,220,222,226,230,236,245]), 18 studies were secondary analyses of a cohort study ([25,33,37,47,63,76,80,88,116,118,126,135,144,152,159,163,183,190,191,223,237]), 6 studies were randomized controlled trials ([70,98,127,150,166,172]), 5 studies were secondary analyses of a trial, ([79,92,93,106,117]), 13 studies were longitudinal studies ([26,59,74,101,104,122,129,136,147,169,181,210,246]), 20 studies were retrospective cohort studies ([39,43,53,60,62,87,114,120,153,165,168,176,194,195,209,227,235,238,241,249]), 3 studies were case–control studies ([56,137,146]), and 1 study was a quasi-experimental uncontrolled pre–post [96]; one each was a randomized, unblinded noninferiority trial [103], repeated cross-sectional cohort study [254], quasi-experimental pre–post test design [90], retrospective pre–post study [108], cluster randomized trial [35], and pilot study [119].
Notably, Ye et al., 2022 [26] published one more study using the same population. Similarly, Thiruchelvam, 2021, authored four studies utilizing data from the Australian Longitudinal Study on Women’s Health (ALSWH), focusing on various aspects such as the prevalence and association of continuous polypharmacy and frailty among older women, frailty and PIMs using the 2019 Beers Criteria, and the impact of home medicines review on frailty among community-dwelling older women ([40,49,97,141]). Additionally, Muhlack et al. published two studies using the same population data [51,52].
3.2. Prevalence of Frailty
The analysis of the prevalence of individuals with frailty across different countries reveals significant variability. The prevalence of individuals identified as non-frail, pre-frail, and frail ranged from 7.5 to 93.2% ([75,96]), 11.8 to 72.9% ([125,225]), and 0.9 to 89.2% ([76,99]), respectively. The prevalence of frailty among older adults varies within and across different countries. For example, in Taiwan, frailty prevalence ranged from 2.9% to 45.8%, ([73,189]), while in Brazil, it ranged from 9.4% to 67.4% ([64,109]). Similar variations were found in countries in Europe and North America (Netherlands: 11.6% to 55% ([200,250]); Spain: 3.7% to 89.2% ([99,136]); UK: 9.2% to 51.5% ([43,120]); USA: 6.8% to 41% ([75,104]); Canada: 1.8% to 44% ([57,216])) and in Asia (Turkey: 7.1% to 45% ([81,187]); Singapore: 6.2% to 27% ([145,220]. The highest prevalence of frailty was reported in a cross-sectional study in Spain, with 89.2% (74 out of 83 participants) [99].
A total of 40 validated scales to measure frailty were used in studies included in this scoping review. The most used scales were the Fried Frailty Phenotype ([29,31,33,43,44,45,47,51,55,56,63,64,70,71,73,75,76,77,81,82,83,84,85,93,94,95,98,105,109,110,116,117,122,123,126,127,132,134,136,139,149,162,163,164,166,174,178,179,186,188,192,193,196,198,203,204,206,208,209,211,212,217,218,219,223,225,227,230,233,239,244,245,246,247,250,251] and the 5-item FRAIL Scale [28,40,42,88,112,133,142,148,156,157,170,184,191,213,220,234,242]). Few studies used a combination of two or more frailty criteria. A total of 77 studies utilized the Fried Frailty Phenotype, with the frailty prevalence ranging from 0.9% to 67.4% ([76,109]). The prevalence for the 5-item FRAIL Scale ranged from 6.2% to 30.8% ([112,220]). The prevalence for the Edmonton Frailty Scale ranged from 25 to 78% ([79,155]).
3.3. Medication Use in Frailty
Twenty studies reported the mean number of medications used by individuals with different frailty statuses, while eight studies reported the median number of medications used by individuals with different frailty statuses, and one study reported both the mean and median numbers of medications used. Supplementary Table S4 shows the distribution of studies reporting the mean or median number of medications in older adults with different frailty statuses. The mean number of medications among older adults with pre-frailty ranges from 2.9 (±standard deviation (SD) 2.2) [234] to 9.9 (±SD 3.7) [215]. For those with frailty, the mean number of medications ranges from 4.3 (±SD 2.9) [234] to 15.6 (±SD 16.8) [173]. Across the studies reporting the median number of medications, among older adults with pre-frailty it ranged from 3 (Interquartile range (IQR) 4) [36] to 12 (range 9–16) [50]. For those with frailty, it ranged from 3 (IQR 3.5) [36] to 16 (range 12–20) [50]. Of the twenty-nine studies that reported on mean and median numbers of medications, nineteen used statistical tests to find out if there is a statistically significant difference in the mean or median number of medications among the three groups of frailty (non-frail, pre-frail, and frail). Seventeen of the nineteen studies that used statistical tests yielded statistically significant results (see Table S4 in Supplementary).
Supplementary Table S5 summarizes the findings from eleven studies on medication usage among different categories of frailty: non-frail, pre-frail, and frail. The most reported medication class among older adults with frailty was for hypertension, with five studies identifying it as the most common medication among participants. Analgesics were reported as the most common medication class in two studies, while medications for the treatment of diabetes was the most prescribed in two studies. Finally, one study found that medications for osteoporosis were the most common among individuals with frailty. The study by Chaitoff et al. [32] reports that among individuals with frailty, the usage rates for diabetes medication, hypertension medication, statins, and aspirin are 33.8%, 75.3%, 45.5%, and 54.9%, respectively. In a study by Ballew et al. [75], 75.7% of individuals identified as non-frail were on a hypertension medication and 52.9% on statins, while a higher proportion of individuals with frailty were on each (87.4% and 54.8%, respectively). Additionally, the study by Jankowska-Polańska et al. [78] highlights that angiotensin-converting enzyme inhibitors are commonly used, with 48% of individuals identified as non-frail and 42.9% of individuals with frailty taking them. The study by Ribeiro et al. [115] shows high usage rates of angiotensin-converting enzyme inhibitors/angiotensin receptor blockers (ACEI/ARBs) and beta-blockers among individuals with frailty, ranging from 83% to 100%. A study by Liu et al. [178] reveals metformin and glucosidase inhibitors as commonly used diabetes medications among individuals with frailty, with usage rates of 39% and 48.8%, respectively. Finally, studies by Koponen et al. [208] and Chen et al. [230] indicate significant usage of analgesics and hypnotics among individuals identified as frail, with rates for analgesics reaching up to 68.1% and for hypnotics up to 19.3%.
3.4. Prevalence of Polypharmacy and Hyper-Polypharmacy
Thirty-three studies investigated the prevalence of polypharmacy across three groups of participants that differed in frailty status (Supplementary Table S6). The prevalence of polypharmacy in older adults with frailty ranges from 1.3% to 96.4% ([76,177]). In a study by König et al. [76], polypharmacy was defined as the use of five or more medications per day, with 1.3% of frail individuals affected, compared to 40.7% of pre-frail individuals. In contrast, Krawariti et al., using a definition of four or more medications per day, found a much higher prevalence of 96.4% among frail individuals in a small Greek sample of 53 community-dwelling older adults [177]. Another German study by Buttery et al. [152] observed that 85.8% of frail individuals were on polypharmacy (≥5 medications), with differences across non-frail, pre-frail, and frail populations.
Eleven studies investigated the prevalence of polypharmacy and hyper-polypharmacy across groups of participants identified as non-frail, pre-frail, and frail (Supplementary Table S7). Among these studies, four ([105,124,208,217]) studies found polypharmacy to be most prevalent among groups with pre-frailty. However, in six studies, polypharmacy was found to be more prevalent among the frailty group ([47,70,83,182,204,211]). In contrast, six ([83,105,120,204,211]) found hyper-polypharmacy to be most prevalent among groups with frailty.
The studies reviewed consistently show that polypharmacy (5–9 medications) and hyper-polypharmacy (≥10 medications) are more prevalent among individuals with pre-frailty and frailty compared to individuals identified as non-frail, as summarized in Supplementary Table S7. Polypharmacy rates among individuals identified as non-frail ranged from 16.2% [124] to 49.1% [182]. For individuals with pre-frailty, the prevalence ranged from 39.1% [208] to 74.2% [182]. Polypharmacy rates among the frail individuals ranged from 39.8% [124] to 76% [182].
3.5. Prevalence of PIMs in Older Adults Based on Frailty
Twelve studies investigated the prevalence of PIMs across groups ranging in frailty status, each using one or more PIMs criteria ([25,33,40,45,49,52,58,70,71,90,179,184,211]). Five studies used Beers Criteria ([25,40,45,70,184]), three studies used STOPP/START (Screening Tool to Alert doctors to Right Treatment) Criteria ([33,58,211]), three studies ([52,90,179]) used a combination of Beers Criteria and STOPP criteria, and one study used each of the European Union (EU) (7)-PIM List [52], PRISCUS List [52], the Turkish Inappropriate Medication Use in the Elderly (TIME) [179], and Brazilian Consensus Potentially Inappropriate Drugs for Older People [71]. Generally, across all studies that reported on PIMs, the prevalence of PIM among individuals with frailty ranged from 2.4% [211] to 95.9% [40]. Across studies that reported PIMs based on Beers Criteria, the prevalence among individuals with frailty ranged from 13.9% [184] to 84.7% [49]. In contrast, for studies that reported PIMs based on STOPP/START Criteria, the prevalence ranged from 2.4% [211] to 86.7% [33] (refer to Table 1).
3.6. Drug-Related Problems in Older Adults with Frailty
Six studies investigated the prevalence of drug-related problems (DRPs) across groups ranging in frailty status (refer to Table 2). Two studies used the Medication Risk Questionnaire (MRQ-10) ([26,161]), two studies used anticholinergic burden (ACB) ([55,160]), one study used Short Emergency Geriatric Assessment (SEGA) [130], and one study used the Swedish Finnish Interaction X-reference (SFINX) Monitor [184]. Generally, across all these studies, the prevalence of DRPs among individuals with frailty ranged from 0.2% [160] to 77.6% [160]. Rhalimi et al. [130] used the SEGA to categorize DRPs. Among the group identified as somewhat frail, 77% (492 out of 638) had no DRPs [130]. In the group with frailty, 62% had no DRPs [130]. For the group identified as very frail, 60% had no DRPs, and 40% had DRPs. These differences were statistically significant (p < 0.001) [130].
The studies by Ye et al. ([26,161]) investigated the risk of DRPs in different populations categorized by their frailty status, using the MRQ-10 (refer to Table 2). The MRQ-10, a validated tool, assesses risks associated with polypharmacy, inappropriate prescribing, poor adherence, and multiple medical problems. In the 2022 study [26], the group identified as non-frail had a significantly lower risk of DRPs, with 65.2% categorized as low risk and 34.8% as high risk at 12 months follow-up. Conversely, the group with pre-frailty exhibited a higher risk, with 52.4% at low risk and 47.6% at high risk, showing a significant difference with p-values of <0.001 for both categories [26].
The study by Alves et al. [71] assessed occurrences of drug–drug interactions (DDIs) at baseline using the Micromedex Drug Reax System across various frailty levels. In the group identified as non-frail, out of 181 individuals, 65 (35.9%) experienced DDIs [71]. In the group with pre-frailty, 131 out of 323 individuals (40.6%) had DDIs [71]. The group with frailty had the highest proportion, with 46 out of 76 individuals (60.5%) experiencing DDIs [71].
Athuraliya et al. [184] investigated the prevalence of DDIs based on the SFINX Monitor. They found that individuals with frailty were significantly more likely to experience negative DDIs compared to individuals identified as non-frail [184]. In the group identified as non-frail, 5.47% (195 out of 3550) were at risk of potential adverse DDIs, and 6.82% (242 out of 3550) experienced ADEs [184]. In the group with frailty, 18.22% (127 out of 684) were at risk of potential adverse DDIs, and 18.71% (128 out of 684) experienced ADEs [184] (see Table 2).
3.7. Impact of Medication Review on Polypharmacy Across Different Frailty Levels
The study by Molist-Brunet et al. [96] investigates the effects of medication review on polypharmacy (defined as the continuous use of ≥5 medications) across varying degrees of frailty, examining whether polypharmacy decreased, remained unaltered, or increased after the review. Among individuals with no frailty, 11.5% (4/32) experienced a decrease in polypharmacy, 69.3% (22/32) remained unchanged, and 19.2% (6/32) saw an increase, with no significant change (p > 0.05) [96]. In those with mild frailty, 22.1% (25/113) saw a decrease, 71.2% (80/113) were unaltered, and 6.7% (8/113) experienced an increase, with a significant p-value of 0.04 [96]. For moderate frailty, 21.6% (43/201) had a decrease, 76.6% (154/201) remained unchanged, and 1.8% (4/201) saw an increase, showing high significance (p < 0.001) [96]. In severe frailty, 54.5% (45/82) experienced a decrease in polypharmacy, while 45.5% (37/82) remained unchanged, and no increase was observed, with a highly significant p-value (p < 0.001) [96].
3.8. Association Between Polypharmacy, Hyper-Polypharmacy, Medication Use, PIMs, and Frailty
Table 3 provides a comprehensive analysis of the associations between medication use, polypharmacy, PIMs, DRPs, and frailty. The data are divided into various factors and their significant or non-significant associations based on different studies.
3.8.1. Association Between Polypharmacy and Frailty
A total of 27 studies examined the association between polypharmacy and frailty. Of the 27 studies, 20 studies report a significant association between polypharmacy and frailty (refer to Table 3) ([25,26,37,46,47,77,80,83,101,105,110,117,129,133,186,189,191,209,217,251]). The strength of the association varied depending on how polypharmacy was defined. Studies by Aprahamian et al. and Aznar-Tortonda et al. found significant associations between using three or more drugs and the risk of frailty ([25,133]). Polypharmacy with ≥4 drugs was also found to be significantly associated with frailty in one study [25] but not in another [234].
However, the association with frailty became more consistent and robust when polypharmacy was defined as (≥5 drugs). Numerous studies, such as those by Aprahamian et al. [25], Ye et al. [26], Kurnat-Thoma et al. [37], Moon et al. [46], Closs et al. [77], Jung et al. [80], Gnjidic et al. [83], Cheung et al. [101], Badrkhahan et al. [110], de Godoi Rezende Costa Molino et al. [117], Thapaliya et al. [186], Setiati [191], Jazbar et al. [60], and Prieto-Contreras et al. [251], confirmed significant associations with an increase in the risk of frailty. However, studies by Huang et al. [73], Hasan et al. [128], and Arslan et al. [180] did not find significant associations.
Some studies explored even higher thresholds, such as ≥6 or ≥8 medications; for instance, polypharmacy (≥6 drugs) showed a positive association with frailty ([25,129]). In the case of polypharmacy with ≥8 drugs, one study found a positive association [189] while the second did not [221]. Polypharmacy (5–9 drugs) shows a positive association with frailty, with significant associations found by Saum et al. [47], Reallon et al. [105], and Herr et al. [217], while Chaouacha et al. [182] did not find a significant association. Polypharmacy (≥5 drugs) plus PIMs shows a positive association, as indicated by Aprahamian et al. [25].
3.8.2. Association Between Hyper-Polypharmacy and Frailty
Six studies assessed the association between hyper-polypharmacy and frailty, all of which demonstrated a significant association between hyper-polypharmacy and frailty (refer to Table 3). Hyper-polypharmacy (both >9 or ≥10 drugs) shows a significant association with higher risk of frailty ([47,83,105,182,217]), as did both polypharmacy (≥5 drugs)[70].
3.8.3. Association Between Medication Use and Frailty
A total of 13 studies reported a significant association between different medication use factors and frailty (refer to Table 3) ([60,83,105,128,142,165,171,178,195,205,223,227,234]). A higher average number of medications shows a positive association with frailty ([163,234]). Medications for high blood pressure, coronary and other heart diseases, diabetes, joint and other pain, anxiety, depression, sleep problems, osteoporosis, chronic bronchitis, and inflammation also showed a positive association [60]. Medication for high blood cholesterol showed a negative association with frailty [60]. Prescription of oral anticoagulation among those with non-valvular atrial fibrillation showed a positive association with frailty [195]. Metformin use shows a positive association with frailty [178]. However, another study determined no significant associations between oral anti-diabetic drugs, insulin, antihypertensives, and lipid-lowering drugs [226].
Antidepressant users with depressive symptoms show a positive association with frailty, as indicated by Lakey et al. [223]. First-generation and second-generation anti-psychotics show a positive association with frailty [165]. Exposure to anticholinergic medications, sedative medications, benzodiazepine, and sleep medication use shows a positive association with frailty ([105,142,171,234]).
3.8.4. Association Between PIMs and Frailty
Seven studies have reported a significant association between PIMs (using any criteria) and frailty (refer to Table 3) ([26,45,51,70,71,160,168]). PIM use determined by 2012 and 2019 Beers Criteria show a positive association with frailty ([45,70]) while PIMs determined by 2015 Beers Criteria show mixed results. For example, Muhlack et al. [51] found positive associations, while Aprahamian et al. [25] and Hasan et al. [128] found no significant association. Beers Criteria to avoid cognitively impaired patients (BEERS dementia PIM), PRISCUS PIM, and EU (7) all show a positive association with frailty, as indicated by Muhlack et al. [51]. The Brazilian Consensus on Potentially Inappropriate Drugs for Older People shows a positive association with frailty, as indicated by Alves et al. [71]. START/STOPP version 2 criteria show no association: Tampaki et al. [91] and Hasan et al. [128] found no significant associations.
The Drug Burden Index (DBI) shows a positive association with frailty, with significant associations ([83,128,227]). Anticholinergic burden (ACB) shows a positive association with frailty, as indicated by Cheong et al. [160]. Anticholinergic drug scale (ADS) score (>0) shows a positive association with frailty, as indicated by Lampela et al. [168].
3.9. Recommendations for Addressing Drug-Related Problems (DRPs) in Older Adults with Frailty
This section highlights recommendations for addressing DRPs in older adults with frailty, providing a comprehensive overview of strategies and interventions designed to manage DRPs in this vulnerable population.
3.9.1. Comprehensive Medication Review and Deprescribing
The cornerstone of addressing DRPs in older adults involves thorough medication reviews and targeted deprescribing practices. One notable intervention is the Family Conferences to Facilitate Deprescribing in Older Outpatients with Frailty and With Polypharmacy (COFRAIL) initiative [35]. The COFRAIL cluster randomized trial aimed to assess the impact of general practitioner (GP)-led family conferences on medication use and clinical outcomes in older adults with frailty and polypharmacy [35]. The study included community-dwelling adults aged 70 and older, taking at least five medications daily. The intervention group, which participated in structured family conferences, showed a temporary reduction in the number of medications at six months. At six months, the mean number of medications in the intervention group decreased from 8.98 (3.56) to 8.11 (3.2) compared to 9.24 (3.44) to 9.32 (3.59) in the control group with a statistically significant difference at six months in the mixed-effect Poisson regression model (p = 0.001). However, in twelve months, the difference was no longer significant, indicating a lack of sustained deprescribing effects over time. After six months, the mean (SD) number of EU (7)-PIMs was significantly lower in the intervention group (1.30 [1.05]) than in the control group (1.71 [1.25]; p = 0.04). There was no significant difference in the mean number of EU (7)-PIMs after 12 months. Commonly deprescribed medications included proton pump inhibitors, urate-lowering drugs, statins, and oral antidiabetics. Despite a modest reduction in medication use, the study did not find a significant reduction in hospitalizations between the intervention and control groups after twelve months.
3.9.2. Pharmacist-Led Deprescribing Reviews
Nishtala et al. (2023) reported a post hoc analysis of an RCT to evaluate the impact of a pharmacist-led deprescribing intervention on anticholinergic burden in frail, community-dwelling older adults [92]. Using the Anticholinergic Cognitive Burden (ACB) scale, the intervention aimed to reduce high risk medication use, such as amitriptyline, diphenhydramine, and oxybutynin, to mitigate cognitive decline. While the pharmacist-led reviews led to a modest reduction (−0.23 mean reduction) in anticholinergic burden, the effect was small and nonsignificant overall (Hedges’ g = −0.04, 95% CI −0.26 to 0.19) [92]. Before the COVID-19 lockdown, a greater deprescribing effect was observed (mean ACB change of −0.38, 95% CI −0.84 to 0.04), but this was not sustained post-lockdown. Limited GP engagement and healthcare disruptions were key barriers to deprescribing success. These findings emphasize the need for stronger interdisciplinary collaboration and structured deprescribing strategies to reduce inappropriate medication use in frail older adults.
3.9.3. Interdisciplinary Team Approaches
Molist-Brunet et al. (2022) conducted a quasi-experimental (uncontrolled pre–post) study to assess the impact of a patient-centered medication review on medication use in older adults with multimorbidity [96]. The intervention, conducted by an interdisciplinary team including a geriatrician and a clinical pharmacist, aimed to reduce inappropriate prescriptions and optimize pharmacological treatment based on individual health goals [96]. The mean number of chronic medications per patient decreased by 17.96%, from 8.13 (SD 3.87) to 6.67 (SD 3.72), after the intervention (p < 0.001). The Medication Regimen Complexity Index (MRCI) was reduced by 19.03% from 31.0 (SD 16.2) to 25.1 (SD 15.1), reflecting a simpler and more manageable medication regimen for patients. The Drug Burden Index (DBI), indicating sedative and anticholinergic medication exposure, decreased by 8.40% from 1.19 (SD 0.82) to 1.09 (SD 0.82) (p < 0.001). The greatest reduction in medication use and regimen complexity was observed in patients with severe frailty (p< 0.001). Frail patients were more likely to benefit from deprescribing interventions, particularly in reducing high risk medications.
3.9.4. Deprescribing Tools and Criteria
The Marta Mejías-Trueba et al. (2023) study evaluated the prevalence of PIMs in polymedicated older adults with multimorbidity using two deprescribing tools: LESS-CHRON and STOPPFrail [99]. The median number of prescribed drugs per patient was 14.4, highlighting a high burden of polypharmacy in this population. LESS-CHRON identified 158 PIMs, while STOPPFrail detected 127 PIMs, with both tools showing a correlation with the number of prescribed drugs. LESS-CHRON was found to be more sensitive in detecting PIMs, particularly in patients with multimorbidity, whereas STOPPFrail provided complementary insights for frail patients with limited life expectancy. The most frequently flagged medications for deprescribing included benzodiazepines for insomnia, antidepressants for reactive depression, and lipid-lowering therapies. Despite their effectiveness, the study underscores the need for individualized deprescribing strategies to reduce inappropriate medication use and improve medication safety in older adults with complex health conditions.
3.9.5. Multifactorial Interventions
A randomized clinical trial was conducted in a Barcelona primary healthcare center by Huguet et al. to evaluate the impact of a multifactorial intervention on preventing the progression from pre-frailty to frailty in community-dwelling adults aged 80 years and older [127]. The intervention included physical exercise, nutritional counseling (Mediterranean diet), social support, and medication review for polypharmacy using STOPP-START criteria.
Among 62 participants with inappropriate prescriptions, 48.4% (30/62) were resolved. After 12 months, frailty progression was lower in the intervention group (8.2%, n = 7) compared to the control group (23.9%, n = 21) (RR was 2.90 times higher in the CG (95% CI 1.45–8.69), with 14.1% (n = 12) of intervention participants reverting to robustness (p < 0.001). Frailty progression was linked to declining autonomy, functional status, and increased social risk, reinforcing the importance of structured interventions in preventing frailty and optimizing medication use in older adults.
Overall, these detailed recommendations and interventions focus on reducing adverse drug events, improving medication appropriateness, and enhancing the overall health and quality of life for frail older adults through a structured and patient-centered approach to medication management.
4. Discussion
This scoping review provides a comprehensive overview of the prevalence and management of frailty among older adults across different regions and populations. It highlights the significant variability in frailty prevalence and the impact of various assessment tools and methodologies. The discussion below synthesizes the key findings and implications, emphasizing the importance of tailored interventions and systematic approaches to managing frailty and associated DRPs in older adults.
4.1. Variability in Frailty Prevalence
This scoping review underscores the substantial variability in frailty prevalence across different countries and studies. For instance, in Taiwan, frailty prevalence ranges from 2.9% to 45.8% ([73,189]), while in Brazil, it spans from 9.4% to 67.4% ([64,109]). The Netherlands exhibits the most variability, with rates ranging from 11.6 to 55% ([200,250]). This wide range of prevalence highlights the influence of demographic factors, study designs, and frailty measurement tools. A frailty prevalence of 1.8% among individuals in BC, as determined through electronic medical records, suggests a relatively low burden of frailty [216]. The study notes that identifying frailty using electronic medical record data is particularly challenging because many functional deficits are not routinely recorded in structured data fields [216]. This limitation results in an under-capture of frailty cases. Differences in how frailty is identified in electronic medical records versus administrative data also contribute to the low prevalence. For instance, studies using administrative data might capture those residing in long-term care facilities or those who are terminally ill, both of whom might not be represented in primary care electronic medical records and represent populations where there is a higher prevalence of frailty. The study methodology and population might also play a role. For example, linked data from BC and Manitoba might not fully represent all individuals with frailty due to differences in healthcare utilization, reporting practices, and regional health demographics [216].
The prevalence of individuals with pre-frailty ranged from 11.8 to 72.9% ([125,225]). The study by Varan et al. had lower prevalence of pre-frailty due to the selection criteria implemented [125]. The study focused on community-dwelling older adults, who are generally more active and independent compared to those in assisted living or nursing homes. The EFS has specific scoring cut-offs that may categorize individuals differently compared to the FFI. Individuals who show mild declines in physical abilities (captured by FFI) may not meet the threshold for pre-frailty under the EFS unless additional domains are affected [125]. Similarly, as the mean age of the population studied increases, so does the prevalence of pre-frailty and frailty, as demonstrated by Pérez-Ros et al. in their study of individuals with a mean age 76.05 years [225], as well as a study conducted in Germany amongst a population with a mean age of 68.7 years and prevalence of frailty of 0.9% [76].
The choice of frailty assessment tools significantly impacts the reported prevalence rates. The article compares various tools, such as the 5-item FRAIL Scale and Fried’s Frailty Phenotype, revealing differing outcomes [7,255]. For instance, the 5-item FRAIL Scale, used by Hung et al. [189] in Taiwan, reported 22.43% of participants as frail. In contrast, Fried’s Frailty Phenotype, also utilized in the study by Hung et al. [189], showed a higher frailty rate of 45.85%. Similarly, the Edmonton Frail Scale (EFS) and the Clinical Frailty Scale (CFS) are two widely used frailty assessment tools that measure different components of frailty. For instance, the EFS might identify a higher prevalence of frailty due to its inclusion of cognitive and functional domains, whereas the CFS, which is more focused on physical performance and clinical judgment, might report a lower prevalence. Different frailty measures can significantly impact the reported outcomes in studies involving older adults [256]. The choice of frailty measure can also influence the observed relationship between frailty and outcomes such as medication use, hospitalization, and mortality [257]. This variability highlights the critical need for standardization in frailty definition and operationalization of frailty identification and monitoring.
4.2. Medication Use and Frailty
The scoping review delves into the relationship between medication use, polypharmacy, and frailty. It consistently finds that individuals with frailty tend to use more medications compared to their counterparts identified as non-frail. For instance, Aprahamian et al. [25] reported mean medication numbers of 2.56, 3.88, and 5.01 for individuals identified as non-frail, pre-frail, and frail, respectively, with significant differences (p < 0.001). Similarly, Gutiérrez-Zúñiga et al. [30] found mean medication numbers of 1.3, 3.2, and 6 for individuals identified as non-frail, pre-frail, and frail, respectively, also with significant differences (p < 0.001). Other studies, such as those by Moon et al. [46] and Gnjidic et al. [83], showed comparable trends. These results underscore a relationship between frailty and the number of medications. This relationship may be bidirectional—an increasing number of chronic conditions increases the risk of frailty but also may require more medications to be managed; however, increasing the use of medications may increase the risk of frailty as well.
Polypharmacy, defined as the use of multiple medications, is prevalent among individuals with frailty and pre-frailty [19]. The article highlights that polypharmacy rates significantly increase with frailty, with individuals with frailty consistently exhibiting higher rates of polypharmacy compared to individuals identified as non-frail and pre-frail. This association is robust across various study designs and populations, although some exceptions exist. Studies by Saeidimehr et al. [228] present atypical results where individuals identified as non-frail had higher polypharmacy prevalence. These exceptions underscore the need for context-specific analyses and interventions.
Definitions of polypharmacy varied slightly across studies, with most defining it as the use of ≥5 medications. Some studies had more specific definitions, such as the use of 5–9 medications per day or the concurrent use of ≥5 medications. The studies by Larsen et al. [57] and Kume et al. [68] explore the prevalence of polypharmacy among individuals identified as non-frail, pre-frail, and frail using different definitions. Larsen et al. [57] used two definitions: regular or occasional use of ≥9 medications and the use of ≥5 medications. The findings showed that with the first definition, 33.4%, 45%, and 52.7% of individuals identified as non-frail, pre-frail, and frail, respectively, experienced polypharmacy. With the second definition, the prevalence was higher, with 72.1%, 81.6%, and 85.5% of individuals identified as non-frail, pre-frail and frail, respectively. Similarly, Kume et al. [68] also used two definitions: the international classification (≥5 medications) and the Japanese classification (≥6 medications). According to the international classification, 18.8%, 29.4%, and 58.3% of individuals identified as non-frail, pre-frail, and frail, respectively, were on polypharmacy (p = 0.004) [68]. The Japanese classification showed 10.1% of non-frail, 19.6% of pre-frail, and 50% of frail individuals on polypharmacy (p = 0.001) [68].
4.3. Potentially Inappropriate Medications (PIMs)
Older adults with multiple health conditions often require numerous medications, increasing the risk of PIMs. The use of PIMs is notably higher among individuals with frailty, as indicated by various studies using criteria like the Beers Criteria and STOPP/START. For instance, Aprahamian et al. [25] using the Beers Criteria (2015) found PIM prevalence at 18.1%, 30.8%, and 46.5% in individuals identified as non-frail, pre-frail, and frail, respectively. Similarly, Bolina et al. [45] using the Beers Criteria (2012) reported 17%, 33.2%, and 51.1% in older adults identified as non-frail, pre-frail, and frail, respectively. Cox et al. [33] using the STOPP Fall tool indicated varied prevalence based on the number of Fall Risk Increasing Drugs (FRIDs), with the highest rates in the groups with frailty. Other studies, like Thiruchelvam et al. [49] and Uragami et al. [58], showed a clear trend of increasing PIM use from non-frail to frail categories using different versions of the Beers Criteria and STOPP-J. Durmuş et al. [179] found similar results using the TIME criteria, reporting PIMs in 37.5%, 44.5%, and 48.4% in individuals identified as non-frail, pre-frail, and frail, respectively.
The lack of a universally accepted definition of frailty complicates an understanding of the relationship between polypharmacy and PIMs and frailty. Moreover, this variability extends to the criteria used for determining PIMs as well, with tools such as the Beers Criteria, STOPP/START Criteria, and others showing different prevalences of PIMs among individuals with frailty. The discrepancies in frailty definitions and PIM criteria hinder the development of standardized interventions, emphasizing the need for a consensus on these definitions to enhance the quality of care for older adults with frailty [258]. Specific drug categories like antipsychotics, anticholinergics, and antidepressants are also associated with an increasing risk of frailty, as highlighted by Porter et al. [211].
4.4. Association Between Medication Use, Polypharmacy, and DRPs with Frailty and Its Implications
As mentioned previously, there is likely a bidirectional relationship between polypharmacy and PIM use and frailty [259]. Frailty significantly impacts medication use, as individuals with frailty are more likely to experience DRPs. Ye et al. [26] found that individuals with frailty had higher risks of DRPs at 12 months (OR: 1.75, p < 0.001), while Saum et al. [47] noted that hyper-polypharmacy (≥10 drugs) was associated with increased odds of frailty both at baseline and within a 3-year follow-up. Negative outcomes associated with polypharmacy and inappropriate medication use include falls, hospitalization, and mortality, particularly among individuals with frailty and pre-frailty [260].
4.5. Recommendations for Addressing DRPs
The report identifies several recommendations for managing DRPs in older adults with frailty. Comprehensive medication reviews and deprescribing practices, such as the COFRAIL initiative and pharmacist-led reviews, may be helpful [35]. These interventions involve interdisciplinary teams and structured approaches to assess and optimize medication use. Tools like the LESS-CHRON and SFINX Monitor can aid in identifying and addressing PIMs and drug–drug interactions ([99,184]).
Multifactorial interventions, combining several approaches, show promise in reducing sedative and anticholinergic medications and improving patient outcomes [172]. Randomized controlled trials (RCTs) evaluating these interventions highlight their effectiveness in lowering DBI scores and enhancing the quality of life for individuals with frailty.
The scoping review on medication use by older adults with frailty has several strengths and limitations. Among its strengths, the review employed a comprehensive methodology, utilizing a five-stage framework proposed by Arksey and O’Malley, supplemented by the PRISMA Extension for Scoping Reviews (PRISMA-ScR). This structured approach ensures thoroughness in identifying, selecting, and analyzing relevant studies. The literature search was extensive, covering multiple databases, which increased the likelihood of capturing all relevant studies. Additionally, the review clearly defined eligibility criteria, focusing on older adults with frailty living at home, and excluding non-English publications and studies without medication-related health outcomes, thereby maintaining the focus and relevance of the included studies. Data regarding study design, demographics, frailty measures, and outcomes were systematically extracted and analyzed, with multiple reviewers enhancing the reliability of the data. The review identified significant findings related to the prevalence of polypharmacy, hyper-polypharmacy, and PIMs among individuals with frailty, as well as the association between polypharmacy and increased odds of frailty.
However, the review also has limitations. There is a lack of a universally accepted definition of frailty and the use of various frailty measurement tools, leading to inconsistencies in diagnosis and treatment, which complicate comparisons across studies and may impact the generalizability of the findings. The exclusion of non-English publications introduces potential language bias, possibly overlooking relevant studies from non-English speaking regions. The heterogeneity of the included studies, in terms of design, population characteristics, and methodologies, poses challenges in synthesizing the findings and drawing definitive conclusions. Despite the comprehensive search strategy, there is always a possibility of selection bias, where some relevant studies might have been missed or excluded during the screening process. The review’s focus on community-dwelling older adults may limit the applicability of the findings to those in hospital or institutional settings where medication use patterns and frailty prevalence might differ. Our search ended in November 2023 and does not include more recent studies, and country-level data for 2024–2025 remain incomplete, leaving a knowledge gap for these years. Another limitation is that our review did not quantitatively analyze the range of participant ages or the length of follow-up used to assess frailty across the included studies. These factors likely contribute to the observed heterogeneity in frailty prevalence and outcomes across countries and study settings.
An additional consideration that may affect the generalizability of these findings is the role of multiple prescribers and transitions of care. Older adults, particularly those with frailty or multimorbidity, often receive prescriptions from several healthcare providers across different settings (e.g., primary care, specialists, hospital discharge). This fragmentation increases the risk of duplicate therapy, drug–drug interactions, and discrepancies in medication reconciliation. Furthermore, transitions between care settings—such as hospital to community or long-term care—represent vulnerable periods when medication regimens may change abruptly without adequate communication among prescribers. These factors can significantly contribute to the development or worsening of potentially inappropriate medication use and related geriatric syndromes.
5. Conclusions
In conclusion, the article highlights the significant variability in frailty prevalence and the impact of assessment tools and methodologies on reported rates. It emphasizes the complex relationship between medication use, polypharmacy, and frailty, underscoring the need for tailored and systematic approaches to manage DRPs. Comprehensive medication reviews, interdisciplinary approaches, and targeted interventions are crucial in optimizing medication use and improving the health outcomes of frail older adults. Standardizing frailty assessment tools and methodologies can enhance comparability across studies and inform more effective and targeted public health interventions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization Ageing and Health Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health(accessed on 15 July 2024)
- 2Government of Canada, Statistics Canada A Portrait of Canada’s Growing Population Aged 85 and Older from the 2021 Census. 27 April 2022 Available online: https://www 12.statcan.gc.ca/census-recensement/2021/as-sa/98-200-X/2021004/98-200-X 2021004-eng.cfm(accessed on 15 July 2024)
- 3Fillenbaum G.G. Pieper C.F. Cohen H.J. Cornoni-Huntley J.C. Guralnik J.M. Comorbidity of five chronic health conditions in elderly community residents: Determinants and impact on mortality J. Gerontol. Ser. A Biol. Sci. Med. Sci.200055 M 84M 8910.1093/gerona/55.2.m 8410737690 · doi ↗ · pubmed ↗
- 4Roberts K.C. Rao D.P. Bennett T.L. Loukine L. Jayaraman G.C. Prevalence and patterns of chronic disease multimorbidity and associated determinants in Canada. Health promotion and chronic disease prevention in Canada: Research, policy and practice Health Promot. Chronic Dis. Prev. Can.201535879410.24095/hpcdp.35.6.0126302227 PMC 4910465 · doi ↗ · pubmed ↗
- 5Tam T. Aging and Chronic Diseases: A Profile of Canadian Seniors Government of Canada Ottawa, ON, Canada 2020
- 6Levers M. Estabrooks C.A. Kerr J.C.R. Factors contributing to frailty: Literature review J. Adv. Nurs.20065628229110.1111/j.1365-2648.2006.04021.x 17042807 · doi ↗ · pubmed ↗
- 7Fried L.P. Tangen C.M. Walston J. Newman A.B. Hirsch C. Gottdiener J. Seeman T. Tracy R. Kop W.J. Burke G. Frailty in older adults: Evidence for a phenotype J. Gerontol. Ser. A 200156 M 146M 15710.1093/gerona/56.3.M 14611253156 · doi ↗ · pubmed ↗
- 8Feng Z. Lugtenberg M. Franse C. Fang X. Hu S. Jin C. Raat H. Risk factors and protective factors associated with incident or increase of frailty among community-dwelling older adults: A systematic review of longitudinal studies P Lo S ONE 201712 e 017838310.1371/journal.pone.017838328617837 PMC 5472269 · doi ↗ · pubmed ↗