Comparison of Serum Sodium Levels Following Intravenous Administration of Isotonic and Hypotonic Solutions in Young Children: A Randomized Controlled Trial
Nisara Chongcharoen, Yupaporn Amornchaichareonsuk, Suwanna Pornrattanarungsi, Ornatcha Sirimongkolchaiyakul

TL;DR
This study compared how isotonic and hypotonic IV fluids affect blood sodium levels in young children and found isotonic fluids better maintain sodium without complications.
Contribution
The study provides new evidence on the safety and efficacy of isotonic IV fluids in maintaining serum sodium in young children.
Findings
Isotonic fluids caused a greater increase in serum sodium at 24 hours compared to hypotonic fluids.
No significant cases of hyponatremia or hypernatremia occurred in either group.
Both groups had similar rates of hyperchloremic metabolic acidosis and no complications.
Abstract
Objectives: This study evaluated changes in serum sodium (S Na) 24 h after the administration of isotonic versus hypotonic intravenous fluids (IVFs) and the incidences of dysnatremia and hyperchloremic metabolic acidosis. Methods: This double-blind, randomized controlled trial involved children aged 3 months to 5 years who were admitted to a general ward between November 2020 and September 2022 and required IVF. We randomly assigned patients (1:1) to receive either an isotonic solution (D50.9%NaCl) or hypotonic solution (D50.45%NaCl). Serum electrolyte and venous blood gas levels were obtained at the time of IVF administration and 24 and 48 h after IVF administration. During this study, all participants were monitored for vital signs, body weight, fluid intake and output, and clinical symptoms of dysnatremia. Results: Totals of 69 and 68 patients received isotonic and hypotonic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
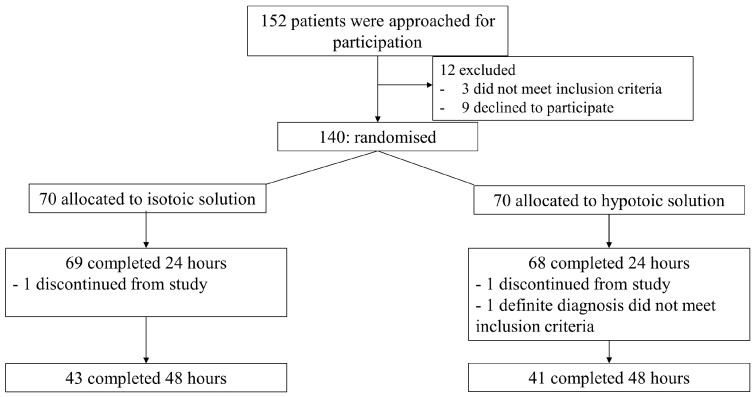 Figure 1
Figure 1- —Navamindradhiraj University Research Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsElectrolyte and hormonal disorders · Sodium Intake and Health · Trauma, Hemostasis, Coagulopathy, Resuscitation
1. Introduction
Supportive care using intravenous fluids (IVFs) has been provided to children who were being treated in hospitals and could not take oral intake. During the past decade, evidence has suggested that hypotonic IVF (sodium 30–100 mEq/L) administration increases the risk of hyponatremia, particularly hyponatremic encephalopathy [1,2], which increases the risk of morbidity and mortality. Currently, an isotonic solution is used worldwide for children who are past the newborn period and do not have underlying diseases [3].
However, interesting questions must be answered. Young children are at a high risk of developing hyponatremia from hypotonic fluids [4]. A few studies have undertaken specific analysis in this age group [5,6,7]. Common causes of admission—such as gastroenteritis or bronchiolitis, which are the most common etiologies for admission at our study site—in younger children have a high prevalence of developing hyponatremia compared with older children [8,9]. Some studies have focused specifically on general wards [6,7,10], where most pediatric admissions occur, and on common diseases. Past studies on fluid types have been broad, encompassing both medical and surgical conditions [11,12,13]. Furthermore, young children are at a high risk of developing hypernatremic complications from isotonic solutions, and there are limited significant findings in the previous studies on the newborn period [14].
Moreover, isotonic solutions have a higher chloride component than human plasma and can cause hyperchloremic metabolic acidosis, which is associated with acute kidney injury and gastrointestinal dysfunction in critically ill children [15]. Past studies that examined these effects focused on critically ill pediatric populations within intensive care units (ICUs); as such, there is a paucity of data regarding the incidence and clinical significance of electrolyte and acid–base imbalances in non-ICU children receiving isotonic fluids [4], and specific studies that involved young children are scarce. ICU patients experience severe diseases, complex complications, and stressful events that affect the electrolyte balance control in the body compared with patients admitted to the general ward. Moreover, young children have a physiological profile that is distinct from older children, including a greater proportion of total body water and a different ratio of extracellular to intracellular fluid [16]. This age group has immature renal function. Young children are potentially more vulnerable to electrolyte disturbances. Therefore, this study was conducted to evaluate the changes in mean serum sodium levels 24 h after the administration of isotonic versus (vs.) hypotonic solutions in young children who were admitted to a non-ICU ward. The secondary objectives included the incidences of hyponatremia, hypernatremia, and hyperchloremic metabolic acidosis and changes in the mean serum sodium levels 48 h after IVF administration.
2. Materials and Methods
A randomized double-blind controlled trial was conducted at the general inpatient ward of Vajira Hospital, Bangkok, Thailand, between November 2020 and September 2022. Children aged 3 months to 5 years who required IVF treatment with initial serum sodium levels of 130–140 mmol/L were enrolled in this study. The exclusion criteria were as follows: neurosurgical disorders, congenital or acquired heart disease, hepatic disease, cancer, renal dysfunction, adrenal insufficiency, diabetes insipidus, voluminous watery diarrhea, severe burn, shock, and preexisting metabolic or electrolyte disorders. This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (COA 100/2563). The trial was registered with the Thai Clinical Trials Registry under the number TCTR20201212004 on 12 December 2020. Note that this study was originally placed in this retrospective registry because of miscommunication between the research team; the research team was promptly registered correctly upon the detection of the error.
2.1. Intervention
The randomization sequence involved a balanced block of four computer-generated methods supervised by a person who was not directly involved in this study, and the code was opened after the parents were allowed to enroll their children in this study. Patients (1:1) were allocated to receive isotonic solution (0.9% NaCl in 5% dextrose; sodium 154 mmol/L) or hypotonic solution (0.45% NaCl in 5% dextrose; sodium 77 mmol/L). The randomization code was kept in a secure location and was not accessible to the research team. The code was only to be unblinded in the case of a serious adverse event, such as a severe electrolyte disturbance requiring immediate, specific treatment. This process ensured the integrity of this study by preventing bias that influenced the patient care or outcome assessment. The fluid types were masked by a person not involved in this study using opaque paper that was identical in appearance and labeled as A or B. This process enabled us to conceal the identities of the IVFs from the patient, family, nurses, physicians, and research team. Informed consent was obtained from the parents before the patients participated in this study.
The rate of IVF administration was calculated according to the Holliday–Segar formula, and the level of dehydration was managed by a treating physician who was not part of the research team. Serum electrolyte and venous blood gas levels were measured before or within 1 h of the initial administration of IVF and at 24 and 48 h if the patient continued to receive the IVF. During this study, vital signs were monitored every 4 h, fluid intake and output were recorded every 8 h, and body weight was assessed every day. Moreover, the research team closely monitored the complications of the IVF treatment, such as volume overload and electrolyte imbalance. Any patient that developed a serious clinical electrolyte disturbance, for example, alteration of consciousness or seizure, stopped receiving the IVF and serum electrolyte levels were measured immediately.
2.2. Outcomes
The primary outcome was the change in serum sodium levels 24 h after the administration of isotonic vs. hypotonic solutions. The secondary outcome was the incidence of hyponatremia (S Na < 135 mmol/L), hypernatremia (S Na > 145 mmol/L), and hyperchloremic metabolic acidosis (serum chloride ≥ 110 mmol/L [17,18] and serum bicarbonate < 20 mmol/L or venous pH < 7.35 [19]). Moreover, the difference in serum sodium levels after 48 h of the initial IVF administration between isotonic and hypotonic solutions was assessed.
2.3. Statistical Analysis
To detect changes in the serum sodium levels 24 h after receiving different IVFs, 63 patients per group were required, which was calculated based on a previous study [6] with a power of 80% and a two-sided alpha level of 5%. Assuming a 10% loss to follow-up, the sample size was increased to 70 patients in each group.
Analysis was performed using the intention-to-treat method. Continuous data are expressed as means ± standard deviations (SDs) or medians (interquartile ranges [IQRs]), whereas categorical data are expressed as percentages. Depending on the data’s normality, either the Mann–Whitney U test or independent t-test was performed to examine the group differences. Categorical data were analyzed using the chi-square test or Fisher’s exact test. To assess the outcomes, the relative risk or mean difference was calculated. Comparison of the outcomes between the isotonic and hypotonic solutions was planned to be performed using generalized linear regression for a binary outcome to estimate the risk ratio. However, we encountered convergence problems during the analysis, which are typical for log binomial regression. The analysis was switched to a modified Poisson regression with a robust error variance [20]. A p-value ≤ 0.05 was used to denote statistical significance. All statistical data were analyzed using the Statistical Package for the Social Sciences (version 23.0; IBM Corp., New York, USA).
3. Results
Of the 152 potentially eligible patients identified in the pediatric ward, 12 patients were excluded because 3 patients did not meet the inclusion criteria because of their initial serum sodium level not being 130–140 mmol/L and 9 patients declined to participate. Finally, 140 patients were randomized. Seventy patients were allocated to the isotonic group; the remaining seventy patients were allocated to the hypotonic group. The isotonic group consisted of 69 subjects because 1 patient withdrew from the trial. One patient in the hypotonic group discontinued this study before 24 h, and one patient was diagnosed with Kawasaki disease; thus, the hypotonic group had sixty-eight patients. IVF administration was discontinued because of clinical improvement and increased oral acceptability. Finally, the isotonic group had 43 patients and the hypotonic group had 41 patients who had completely received IVF at 48 h (Figure 1).
Table 1 shows the baseline characteristics of the patients. The mean ages in the isotonic and hypotonic groups were 1.95 ± 1.25 and 1.91 ± 1.32 years, respectively, where no significant difference in age was observed between the two groups. The baseline characteristics were similar between both groups, including sex, body weight, diagnosis, initial temperature, and degree of dehydration. Of the patients in the isotonic group, 27.1% were unable to eat or drink by mouth on the first day due to respiratory distress or seizures compared with 22.8% in the hypotonic group. This difference was not statistically significant (p-value = 0.55). The mean serum sodium, chloride, bicarbonate, and pH levels from venous blood gas were not different between the isotonic and hypotonic groups. Furthermore, the IVF volumes and oral intakes were similar in both groups. However, the amounts of sodium received differed according to the study protocol (isotonic group > hypotonic group) (Table 2).
3.1. Primary Outcome
The primary outcome was the change in serum sodium levels from baseline to 24 h. The isotonic group showed a change of 2.97 mmol/L (IQR, 2.32–3.62), while the hypotonic group’s change was 2.19 mmol/L (IQR, 1.54–2.84). These changes were not statistically different (mean difference, 0.78; 95% confidence interval [CI], −0.14 to 1.70; p-value = 0.09). Table 3 shows the outcomes.
3.2. Secondary Outcomes
The incidence of hyponatremia 24 h after the IVF administration was higher in the hypotonic group than in the isotonic group (13.2% vs. 7.3%); however, the difference was not statistically significant (relative risk, 0.55; 95% CI, 0.19 to 1.56; p-value = 0.25). Neither severe hyponatremia (S Na < 125 mmol/L) nor hypernatremia occurred in any participant after receiving IVF for 24 h. At 24 h, the incidence of hyperchloremic metabolic acidosis was 8.7% in the isotonic group and 2.9% in the hypotonic group. No significant difference was observed (relative risk, 2.96; 95% CI, 0.61 to 14.22; p-value = 0.17). At 48 h from baseline, there was no change in the serum sodium levels: 2.76 mmol/L (2.00–3.51 mmol/L) in the isotonic group vs. 2.41 mmol/L (1.61–3.22 mmol/L) in the hypotonic group (mean difference, 0.35; 95% CI, −0.76 to 1.45; p-value = 0.53).
3.3. Side Effects
There were no changes in body weight 24 and 48 h after the initial treatment between the two groups (24 h: mean difference, 0.01; 95% CI, −0.77 to 0.78; p-value = 0.98) (48 h: mean difference, −0.27; 95% CI, −1.36 to 0.83; p-value = 0.62). Moreover, hypertension did not develop in either group (Table 4), indicating no notable fluid overload in either group. During the study period, the patients did not have any edema, alteration of consciousness, or seizure from electrolyte imbalance or volume overload. The hospital stay duration was the same in both groups (3.35 ± 1.40 days vs. 3.34 ± 1.62 days in the isotonic vs. hypotonic groups, respectively; mean difference, 0.01; 95% CI, −0.50 to 0.52; p-value = 0.97).
4. Discussion
A double-blind randomized controlled trial was conducted to compare isotonic (0.9% NaCl in 5% dextrose) and hypotonic (0.45% NaCl in 5% dextrose) solutions. The changes in the mean serum sodium level 24 h after receiving IVF were similar between the young non-ICU patients, independent of their medical condition. This finding is different from that of Ramanathan et al. [10], who only studied patients with severe pneumonia and compared 0.9% NaCl with 0.18% NaCl, finding that the mean serum sodium significantly changed at 0 to 24 h but not significantly at 12 to 24 h. Kumar et al. [6] found a significant change in serum sodium levels 24 h after baseline in patients with medical problems; the most common diagnosis was respiratory diseases in the isotonic group (52.4%) and hypotonic group (52.4%) and the second diagnosis was central nervous system diseases in the isotonic (23.8%) and hypotonic (22.6%) groups. As the diagnosis had an influence on the hyponatremia, the frequency of diagnosis was different from our study. A meta-analysis and systematic review showed that the hypotonic solution only led to lower serum sodium levels after less than 24 h when compared with the isotonic solution [21]. A meta-analysis and systematic review [21] included differences in the cause of admission and fluid types, in contrast with the current study (Table 5).
Our findings show that the incidence of hyponatremia at 24 h in the hypotonic group (13.2%) was higher than that in the isotonic group (7.3%); however, the difference was not statistically significant (p-value = 0.25). Despite no statistically significant difference in the incidence of hyponatremia between the isotonic and hypotonic groups, the fact that the incidence of this adverse event was not higher in our isotonic group and trended lower may provide evidence for the clinical appropriateness of using isotonic fluids in this population. Our findings, while not statistically significant, align with Kumar et al. [6] and Friedman et al. [22], who revealed the same finding in children who were acutely ill in general wards. Fernández-Sarmiento et al. [23] found the same result in patients admitted to pediatric ICUs. However, a systematic review and meta-analysis [21,24] of previous studies showed a significantly higher incidence of hyponatremia in patients that received a hypotonic treatment vs. an isotonic treatment, which included the ICU setting, surgical conditions, neonates, and varying types of fluids (0.18% NaCl, 0.3% NaCl, 0.45% NaCl) because non-osmotic stimuli to antidiuretic hormone secretion are triggered by pain, stress, nausea, and operations; moreover, surgical patients also had fluid leaking, which worsened their hyponatremia. Although the IVF rates in the earlier studies and our analysis were different, Wang et al. [25] discovered that the type of IVF—not its rate—affected the hyponatremia risk. The safer period regarding the hyponatremia risk from isotonic solution is 72 h following therapy; this study monitored serum sodium levels at 24 and 48 h, which can be applied in clinical practice. This study supported a previous result [26] showing that the incidence of hypernatremia was comparable across groups. Hypernatremia is of concern when using an isotonic solution, but this event did not occur in the isotonic group in this study. This underscores the importance of a clinically driven approach that prioritizes patient safety over statistical variations.
The important point against using isotonic solutions was inducing hyperchloremic metabolic acidosis because of the higher chloride component than that in human plasma. Our study demonstrated an incidence of 8.7% 24 h after the isotonic fluid treatment, which was consistent with that of hypotonic fluid. A similar result was obtained from a previous randomized controlled trial conducted in general wards and ICUs [12]. However, a retrospective cohort study in ICUs found that isotonic solutions increased the hyperchloremic metabolic acidosis risk, which was different in this study for patients in the general ward. Although one-third of the patients received isotonic solution (0.9% NaCl) at 10 mL/kg in 1 h because of moderate dehydration, this bolus volume was insufficient to generate hyperchloremic metabolic acidosis. The other adverse effects of isotonic solutions were hypertension and increased body weight, which were not found in this study because the volume intake was comparable between the two groups, and hypernatremia did not occur in the isotonic group. Regarding the outcome, the length of stay was the same between the two groups, in agreement with Robles et al. [13] and Hasim et al. [24].
Limitations
This study’s strength was that it was a double-blind randomized controlled trial in a particular age group of children who had nonsurgical issues and were admitted to the general ward, which is practical for pediatricians; however, our findings might not be generalizable to other children. While the difference in serum sodium between the isotonic and hypotonic groups was found to be statistically insignificant, we recognize a critical limitation regarding its clinical interpretation. Future study must correlate statistically significant differences in serum sodium with these definitive clinical endpoints to establish true clinical superiority. Because some young patients were breastfeeding and had uncontrolled urination, determining the precise volume intake and output was very challenging. This study did not have detailed data on the sodium contents of the milks and foods consumed by the participants. Future research should consider including this information to provide a more comprehensive analysis. Furthermore, to determine the incidence of significant hyperchloremic metabolic acidosis, we needed a larger sample size and to enroll critically ill patients in the ICU.
5. Conclusions
Isotonic solutions may be a suitable option for maintaining hydration in pediatric patients under 5 years of age who have medical issues in a general ward. Isotonic solution helps with maintaining the serum sodium level and does not significantly increase the electrolyte disturbance or clinical complications. However, the practical point of care for managing IVF involves clinical adjustment and monitoring. Future studies should focus on long-duration outcomes and the potential for complications in more critically ill young pediatric populations, where the fluid balance is more sensitive.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Benzon H.A. Bobrowski A. Suresh S. Wasson N.R. Cheon E.C. Impact of preoperative hyponatraemia on paediatric perioperative mortality Br. J. Anaesth.201912361862610.1016/j.bja.2019.07.02431540668 · doi ↗ · pubmed ↗
- 2Hoorn E.J. Geary D. Robb M. Halperin M.L. Bohn D. Acute hyponatremia related to intravenous fluid administration in hospitalized children: An observational study Pediatrics 20041131279128410.1542/peds.113.5.127915121942 · doi ↗ · pubmed ↗
- 3Feld L.G. Neuspiel D.R. Foster B.A. Leu M.G. Garber M.D. Austin K. Basu R.K. Conway E.E.Jr. Fehr J.J. Hawkins C. Clinical Practice Guideline: Maintenance Intravenous Fluids in Children Pediatrics 2018142 e 2018308310.1542/peds.2018-308330478247 · doi ↗ · pubmed ↗
- 4Toledo J.D. Morell C. Vento M. Intravenous isotonic fluids induced a positive trend in natraemia in children admitted to a general paediatric ward Acta Paediatr.2016105 e 263e 26810.1111/apa.1331626684406 · doi ↗ · pubmed ↗
- 5Padua A.P. Macaraya J.R. Dans L.F. Anacleto F.E.Jr. Isotonic versus hypotonic saline solution for maintenance intravenous fluid therapy in children: A systematic review Pediatr. Nephrol.2015301163117210.1007/s 00467-014-3033-y 25576065 · doi ↗ · pubmed ↗
- 6Kumar M. Mitra K. Jain R. Isotonic versus hypotonic saline as maintenance intravenous fluid therapy in children under 5 years of age admitted to general paediatric wards: A randomised controlled trial Paediatr. Int. Child. Health 202040444910.1080/20469047.2019.161905931138063 · doi ↗ · pubmed ↗
- 7Shukla S. Basu S. Moritz M.L. Use of Hypotonic Maintenance Intravenous Fluids and Hospital-Acquired Hyponatremia Remain Common in Children Admitted to a General Pediatric Ward Front. Pediatr.201649010.3389/fped.2016.0009027610358 PMC 4996996 · doi ↗ · pubmed ↗
- 8Milani G.P. Rocchi A. Teatini T. Bianchetti M.G. Amelio G. Mirra N. Grava A. Agostoni C. Fossali E.F. Hyponatremia in infants with new onset moderate-severe bronchiolitis: A cross-sectional study Respir. Med.2017133485010.1016/j.rmed.2017.10.02829173449 · doi ↗ · pubmed ↗