Comparative Clinicopathological Analysis of Oral Focal Mucinosis and Solitary Cutaneous Focal Mucinosis: A Case Series and Literature-Based Analysis
Wickramasinghe Mudiyanselage Sithma Nilochana Wickramasinghe, Primali Rukmal Jayasooriya, Balapuwaduge Ranjit Rigobert Nihal Mendis, Tommaso Lombardi

TL;DR
This study compares two rare benign lesions, oral focal mucinosis and solitary cutaneous focal mucinosis, highlighting differences in age, gender, and lesion location.
Contribution
This is the first direct comparison of OFM and SCFM, using the largest OFM case series reported to date.
Findings
OFM predominantly affects younger females, mainly on the gingiva, with larger lesions.
SCFM occurs more frequently in older males on extremities and trunk.
Both lesions are often misdiagnosed due to nonspecific clinical features.
Abstract
Background/Objectives: Oral focal mucinosis (OFM) and solitary cutaneous focal mucinosis (SCFM) are rare, benign lesions characterized by localized mucin deposition in the stromal connective tissue. While both share similar histological features, they occur in distinct anatomical sites and clinical contexts and have not been directly compared in the literature. Method: This study presents a case series of 39 OFM cases diagnosed over 25 years, supplemented by a literature review of previously reported OFM cases, and compares the combined data with published cases of SCFM. The literature-based analysis included 116 OFM cases published in four articles and 138 cases of SCFM published in five articles. Demographic and clinical data were extracted and analyzed, including age, sex, lesion location, size, duration, symptoms, clinical impression, treatment, and recurrence. Results: The mean age…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
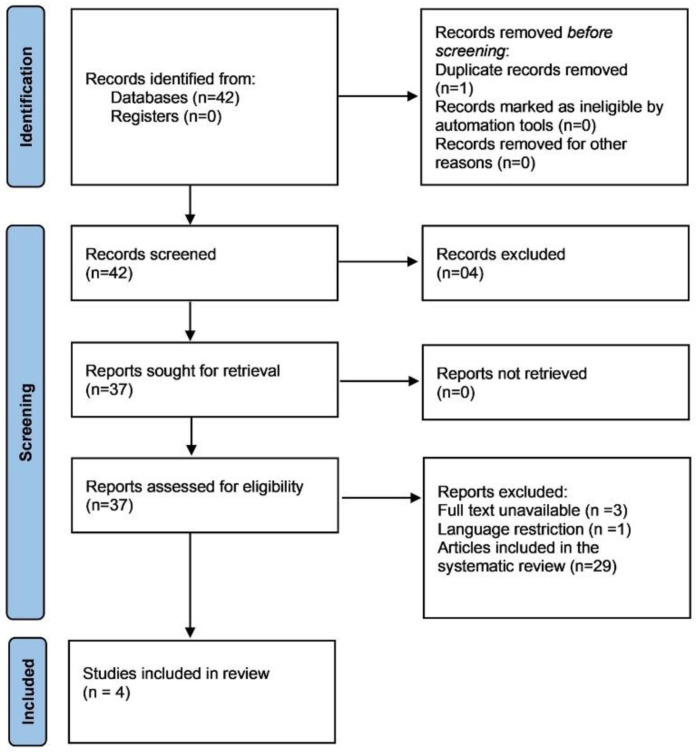 Figure 1
Figure 1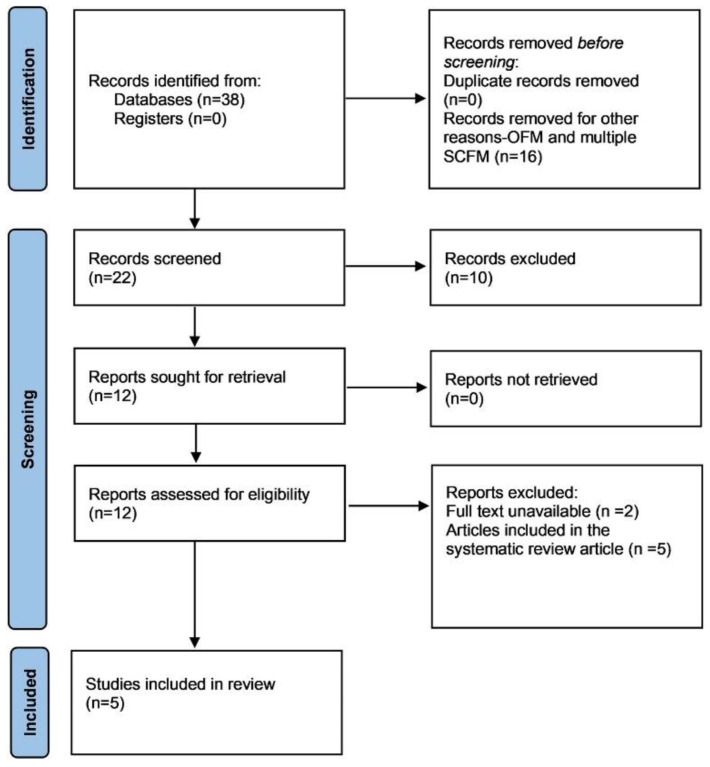 Figure 2
Figure 2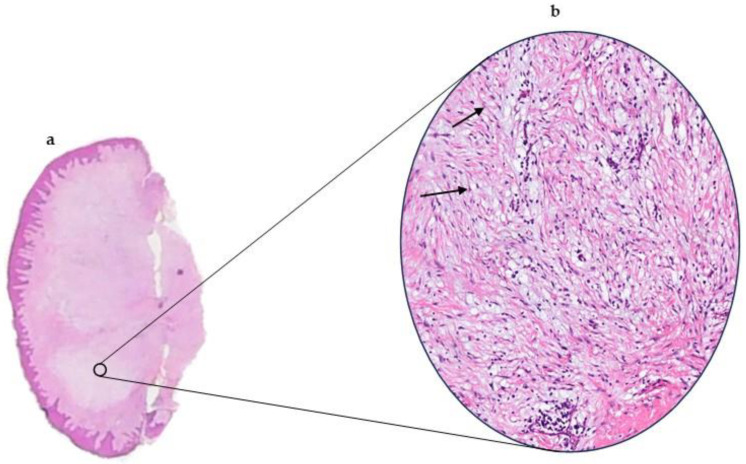 Figure 3
Figure 3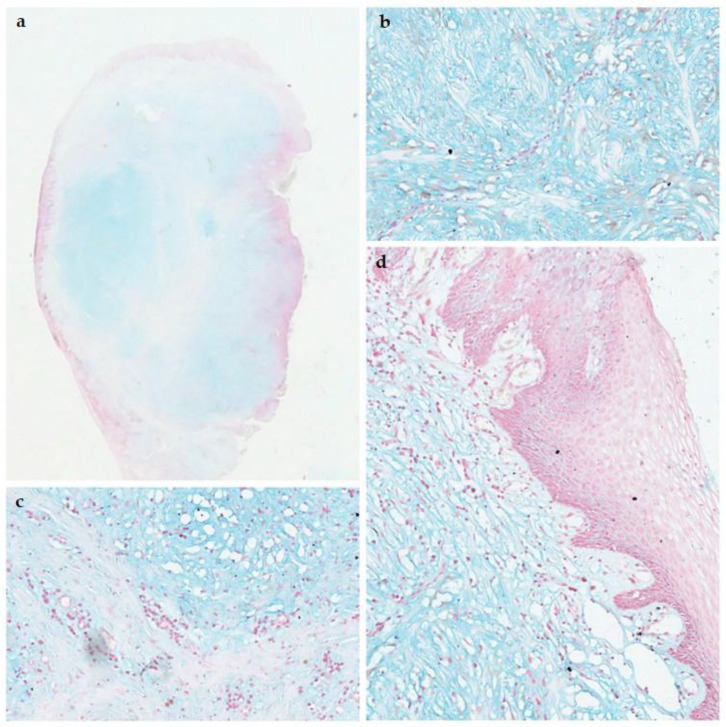 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral and Maxillofacial Pathology · Vascular Tumors and Angiosarcomas · Oral and gingival health research
1. Introduction
Mucinoses represent a group of disorders characterized by the pathological accumulation of mucin in the connective tissues of the skin or oral mucosa. These lesions can be localized or part of a systemic disorder [1]. Among the localized variants are solitary cutaneous focal mucinosis (SCFM) and oral focal mucinosis (OFM). Both entities are benign and histologically similar but differ in anatomical location, patient demographics and clinical presentation [2].
SCFM was first described by Johnson and Helwig in 1966 as a solitary, asymptomatic, skin-coloured papule or nodule [3]. It is characterized by the deposition of mucin in the upper dermis, and most commonly, the extremities and trunk of middle-aged male patients are affected [1]. While the etiology is undetermined, local trauma has been suggested as a possible trigger [1]. SCFM is typically managed with simple surgical excision [1].
OFM, introduced by Tomich et al. in 1974, is regarded as the oral counterpart of SCFM [4]. It is an uncommon tumour-like mass similarly characterized as SCFM by localized myxoid changes in the connective tissue. It is of unknown etiology and thought to occur as a result of over production of hyaluronic acid by fibroblasts [4]. OFM commonly presents on the gingiva of middle-aged female patients as an asymptomatic nodule or swelling [2]. Being a rare, reactive lesion, it is often misdiagnosed clinically as other reactive lesions such as epulides. Like SCFM, the treatment of choice is conservative surgical excision [5] and OFM, once excised rarely recurs.
Despite similar clinical and histological features, OFM and SCFM are rarely compared in the literature. This study aimed to present the largest OFM series to date and compare its clinicopathological features with SCFM to clarify distinctions and enhance diagnostic accuracy.
2. Materials and Methods
This study was designed as a retrospective case series and literature review. It included 39 previously unpublished cases of OFM retrieved from the archives of the Department of Oral Pathology, Faculty of Dental Sciences, University of Peradeniya, supplemented with an additional 116 published OFM cases identified from the literature. For SCFM, all available cases (138) reported in the literature were included for comparison. Studies were included if they met the following inclusion criteria. Population: human subjects diagnosed with OFM or SCFM. Diagnosis: confirmed through histopathological examination. Location: lesions located in the oral cavity (OFM) or skin (SCFM). Study design: case reports, case series, systematic reviews of case series. Language: published in English. Studies were excluded if they were not peer-reviewed (e.g., letters to the editor, conference abstracts), focused on animal models or in vitro studies, or did not provide sufficient clinical or histopathological data.
A comprehensive synthesis of the literature was conducted, focusing on clinical features: age, gender, lesion size, location, and symptoms; histopathological findings: myxoid degeneration and cellular characteristics; diagnostic methods: techniques used for diagnosis, including staining and imaging; treatment approaches: surgical excision, recurrence rates, and follow-up outcomes; and comparative analysis: differences and similarities between OFM and SCFM.
2.1. Case Series
The 39 cases of OFM retrieved from the archives of the Department of Oral Pathology, were diagnosed over a period of 25 years from 2000 to 2025. Data on patient demographics, including age, sex and lesion site, size, duration, morphology, number of lesions, symptoms, histopathology, management and recurrence, were obtained from clinical records and pathology databases and evaluated. Histopathological diagnoses of OFM were confirmed by one of the authors (PRJ) prior to its inclusion.
2.2. Study Selection and Data Extraction from the Literature
2.2.1. OMF
A literature review was conducted to compare the clinical and pathological spectrum of the present series with previously reported cases of OFM in the literature. Electronic searches without publication date restriction were undertaken in May 2025 in the following databases: PubMed/MEDLINE and Google Scholar. Search strategy included terms [“oral focal mucinosis” [Title/Abstract] OR “solitary oral focal mucinosis” [Title/Abstract] OR “OFM” [Title/Abstract] OR “oral focal myxoid lesion” [Title/Abstract] restricted to the years 2000–2025. A total of 42 publications were found in electronic searches for OFM (Figure 1). After elimination of duplicates and application of inclusion and exclusion criteria, a total of 37 full texts were assessed for eligibility. Records included in the systematic review article were excluded (n = 29), along with 4 other articles for full-text unavailability (n = 3) and language restrictions (n = 1). A total of 4 articles were included in the literature review. This included the OFM systematic review article published in 2024 and 3 other case reports from Iran, India, and Japan. Titles and abstracts of all references retrieved through the electronic searches were read. If the title and abstract met the eligibility criteria, the article was included for full-text reading.
For each included study, the following data were extracted on a standard form: publication details, patient’s sex, age, symptoms, anatomical location of the lesion, size of the lesion, duration, clinical presentation, diagnostic hypothesis, management, and recurrence Figure 1 [5,6,7,8]. Unavailable data were defined as not available (NA).
2.2.2. SCFM
Electronic searches were undertaken in May 2025 in the following databases: PubMed/MEDLINE and Google Scholar. The following search strategy was used: “cutaneous focal mucinosis” [Title/Abstract] OR “solitary cutaneous mucinosis” [Title/Abstract] OR “solitary focal cutaneous mucinosis” [Title/Abstract] OR “SFCM” [Title/Abstract] restricted to the years 2000–2025.
A total of 38 articles were retrieved (Figure 2). Articles describing case reports or case series of SCFM published in English with enough clinical and histopathological information to confirm the diagnosis were included. Articles on oral focal mucinosis, multiple cutaneous mucinosis and unrelated articles were excluded. Five articles included in the review article were also excluded. Data was extracted from 5 articles Figure 2 [1,9,10,11,12].
2.3. Statistical Analysis
Descriptive and quantitative data analyses were performed using the Statistical Package for the Social Sciences for Windows, version 20.0 (SPSS, Inc., Chicago, IL, USA). The normality of data was assessed using the Shapiro–Wilk test. As the data were normally distributed, comparisons between the case series of OFM and literature-based OFM with respect to mean age at diagnosis, evolution times of the lesions, and lesion size were performed using the independent-samples t-test, while categorical variables (sex distribution and anatomical locations) were compared using the chi-square test. A significance threshold of p < 0.05 was applied. Corrections for multiple testing were considered unnecessary as the comparisons were limited.
3. Results
The clinical data of the 39 OFM cases of the present study are summarized in Table 1.
The present series (Table 1) comprised 20 females (51.28%) and 19 males (48.71%), with a 1.05:1 female-to-male ratio. The mean age of patients was 43.86 ± 15.80 years (range: 14–70 years). The most common anatomical location was the gingiva (22 cases, 56.41%), followed by the alveolar ridge mucosa (8 cases, 20.51%) and palate (7 cases, 17.95%). Most cases were asymptomatic (36 cases, 92.31%) although a bleeding tendency had been reported in some cases (3 cases, 7.69%). The lesion size averaged at 2.15 ± 1.36 cm. The average duration of lesions prior to diagnosis was 21.25 ± 27.75 months. Clinically, most lesions were diagnosed as reactive lesions (74.19%). The comparison of gingival lesions between maxilla and mandible showed no statistically significant difference (p = 0.79). Statistical analysis revealed significant differences in sex distribution and lesion size between the present series and the literature (p = 0.027 and p = 0.009). The literature demonstrated a marked female predominance, with 70.80% of cases reported in females and a female-to-male ratio of 2.42:1. Comparison with the literature revealed no significant differences in age distribution (p = 0.235), anatomical site (p = 0.74), and duration (p = 0.59). A single case of recurrence was observed, aligning with previously reported findings in the literature. The lesion recurred 7 months after complete surgical excision (Table 2).
3.1. Pathological Features
On macroscopic examination, the lesions presented as whitish mucosal nodules. Microscopically, a mucosal nodule covered by stratified squamous epithelium was observed. The corium contained loosely arranged fibrous tissue in a myxoid stroma. A total of 29.41% of cases (10 cases) showed an inflammatory infiltrate (Figure 3a,b). Four cases (10.2%) showed an ulcerated epithelium. Out of the 39 cases of OFM, 17 had an Alcian blue stain performed to show the mucinous material within the stroma (Figure 4a–d). All 17 cases (100%) were positive for the alcian blue stain.
3.2. Comparison with Solitary Cutaneous Focal Mucinosis
Comparison of the present OFM series with the literature revealed no significant differences in age distribution, lesion size, anatomical site, and duration. A statistically significant difference in the sex distribution between the present series and the literature was detected (p = 0.027). However, both revealed a female predominance. Therefore, the data of the present series was incorporated to the literature review for the comparative analysis with SCFM.
The following data were extracted from the selected SCFM studies in the literature: patient’s sex, mean age, age range, duration of lesion, number of lesions, size of lesion, symptoms, morphology, site, treatment, and recurrence [1,9,10,11,12]. Table 3 compares the demographic features and clinical characteristics of the two entities.
4. Discussion
Cutaneous focal mucinosis is a dermal degenerative primary mucinosis. The term was first introduced by Johnson and Helwig in 1966 to describe an asymptomatic solitary lesion on the skin. In 2016, Kuo et al. suggested that this skin lesion be referred to as solitary cutaneous focal mucinosis [1]. OFM is described as the oral counterpart of SCFM. OFM is a rare, benign soft tissue lesion of unknown etiology [13]. It was first described in 1974 by Tomich et al. [4]. To the best of our knowledge, the present study represents the largest series of OFM cases reported in the literature. Furthermore, it is the first clinicopathological comparison of OFM with SCFM.
The pathogenesis of SCFM remains to be determined. It is considered as a benign local reactive mucinosis. It has typically not been associated with systemic diseases. Localized trauma has been hypothesized as an etiologic factor in the development of SCFM [1]. The pathogenesis of OFM is undetermined. Studies have suggested that it is caused by the overproduction of hyaluronic acid by fibroblasts, which causes localized myxomatous changes. However, the reason for this overproduction is unknown. Some authors suggest that local trauma is the predisposing factor, but it remains controversial [4,13]. The present series did not reveal any apparent involvement of masticatory trauma or local irritation. Immunohistochemical studies indicate that these lesions are typically negative for SMA, CD34, and CD68, supporting their non-neoplastic, reactive nature and distinguishing them from other myxoid soft tissue lesions (Table 4).
The observed difference in sex distribution between our case series of OFM and the literature may reflect sampling variability, population-specific factors, and referral or reporting patterns [5,6,7,8]. Smaller sample sizes in previous studies and regional differences could have underrepresented one sex, contributing to the discrepancy with our findings. These variations highlight the need for larger, multi-centre studies to clarify possible epidemiological trends.
While SCFM is more prevalent in males with a male/female ratio of 1.46:1, OFM is more prevalent in females with a male/female ratio of 0.50:1. The mean age of patients with SCFM was 52 years compared to 41 years of OFM patients. All SCFM lesions were asymptomatic as opposed to only 89.76% of OFM lesions. The size of SCFM lesions ranged from 2 to 20 mm with a variable duration, ranging from months to years. Conversely, the OFM lesions ranged in size from 1 to 100 mm, with an average duration of 18.58 months. SCFM commonly affects the skin of extremities (55.07%), the trunk (31.88%), and the head and neck (13.04%). The most common intraoral sites of OFM are the gingiva (52.94%) and palate (16.99%), followed by the alveolar ridge mucosa (13.73%). Occurrence in the lip (1.96%) and the floor of the mouth (0.65%) are rare, with only a few published cases in the literature [5,6,7,8]. Clinically, the SCFM lesion appears as an asymptomatic, solitary nodule or papule on the skin. It is typically flesh-coloured but may also appear white or red [1]. Based on above findings this study provides new comparative insights into SCFM and OFM. While SCFM mainly affects older adults and the extremities with a slight male predominance, OFM occurs in younger individuals with a predilection for gingiva and other oral sites with a female predominance. OFM lesions were larger and more likely to be symptomatic than SCFM, and a small recurrence rate was noted for OFM but not SCFM. These findings highlight clear differences in clinical presentation, lesion size, and anatomical distribution, offering a more detailed understanding than previously available [1,5,6,7,8,9,10,11,12].
The most commonly considered clinical diagnoses of the SCFM lesion were basal cell carcinoma (31%) and nevus (26%). Other differential diagnoses included cyst (12%), seborrheic keratosis (8.5%), and fibroma (7%) [1]. Interestingly, SCFM had never been included in the diagnoses by the clinicians. This suggests the unfamiliarity of dermatologists with this lesion, possibly because it is a very rare condition [3]. Recognizing SCFM is crucial to prevent misdiagnosis as common lesions like molluscum, warts, milia, and cysts [14]. Therefore, it is important to draw attention to include solitary CFM in clinical differential diagnosis of polypoid skin lesions [3].
However, the clinical features of OFM are not specific [2]. Most cases (89.76%) present as asymptomatic solitary nodules or lumps with a fibrous or hyperplastic appearance. The majority of cases (122 cases, 92.42%) had been diagnosed clinically as reactive lesions, such as fibrous epulis, fibroepithelial polyp, pyogenic granuloma, peripheral giant cell granuloma, etc. Furthermore, none of the clinical diagnoses of the present series or those reported in the literature included OFM.
SCFM and OFM share similar histopathological features. A well-circumscribed region of myxoid connective tissue can be observed in both with delicate collagen fibres and scattered spindle shaped fibroblasts. The principal pathological feature of SCFM is the deposition of mucin in the upper dermis. This can extend into the deeper dermis and rarely into the superficial subcutaneous fat [1]. It appears well-localized but unencapsulated. The mucinous change appears lightly basophilically stained on hematoxylin-and-eosin-stained sections (Figure 3). Special stains, such as Alcian blue, have been used to confirm the mucinous material as hyaluronic acid [1]. Fibroblasts are scattered within the mucinous stroma along with reduced amounts of collagen fibres, elastic fibres, and reticulum fibres. The overlying epidermis may be normal, atrophic, or hyperplastic [1]. Table 4 summarizes the diagnostic criteria of OFM and SCFM.
Histopathologically, OFM must be distinguished from odontogenic myxoma, myxoid solitary fibrous tumour, myxoid neurofibroma, and fibrous hyperplasia with myxoid degeneration [2]. Odontogenic myxoma differs by its odontogenic origin, intraosseous location, and aggressive behaviour, necessitating radiological exclusion before confirming OFM. Although OFM lacks specific immunohistochemical markers, IHC is useful for excluding other myxoid lesions—S-100 helps rule out neural tumours, while CD34, STAT6, and BCL2 assist in excluding myxoid solitary fibrous tumour [14,15].
The main histopathological differential diagnoses of SCFM include intramuscular myxoma, superficial angiomyxoma, nodular fasciitis, myxoid dermatofibroma, and dermatofibrosarcoma (DFSP) with myxoid change [1,14,15]. Superficial angiomyxoma shows prominent vasculature, neutrophil-rich stroma, a lobular growth pattern, and CD34-positive spindle cells; multiple lesions require exclusion of Carney complex. Nodular fasciitis is SMA-positive with fascicular spindle cells, whereas SCFM is SMA-negative. Myxoid dermatofibroma is CD68-positive, and DFSP shows CD34-positive spindle cells, both features absent in SCFM. Other mucin-rich dermal lesions that may require exclusion include lupus erythematosus (tumid variant), mucinous nevus, mucinous fibroma, myxoid cyst, and self-healing juvenile cutaneous mucinosis [14,15].
Dermoscopic observations of the SCFM lesion revealed a non-specific homogenous whitish pattern possibly due to the birefringent properties of mucin or reduced number of melanocytes in the epidermis above the dermal mucin, or both [1,16]. Electron microscopy confirmed the presence of stellate fibroblasts scattered in the mucinous stroma along with reduced number of collagen, elastic and reticulum fibres [1]. It is important to emphasize the solitary nature of the lesion of both SCFM and OFM. Thus, avoiding the erroneous use of the terms SCFM and OFM to describe multiple lesions associated with mucinosis-related systemic diseases such as Hashimoto thyroiditis, Birt–Hogg–Dubé syndrome, and Graves’ disease [2]. This differentiation is essential, as the management strategies differ. It has been confirmed that SCFM and OFM patients do not present with any mucinosis-related systemic conditions [2,3]. Therefore, additional laboratory investigations for patient evaluation are not required. Simple surgical excision is the treatment of choice [2,16,17]. In contrast, the presence of multiple lesions should prompt evaluation for an underlying systemic condition [3]. In the present series, all lesions were confined to the oral cavity, and systemic involvement was excluded. Recurrence of the SCFM lesion has not been reported [1]. Only two recurrences of OFM cases have been reported in the literature. The present series also highlighted one recurrence.
The comparative analysis between OFM and SCFM improves diagnostic accuracy by clarifying subtle clinicopathological differences between these two morphologically overlapping entities. By highlighting distinctions in demographics, site, clinical presentation, and histopathological patterns, this study provides practical diagnostic criteria that help prevent misdiagnosis.
5. Conclusions
In conclusion, the present study reports the largest series of OFM cases to date, provides the first direct clinicopathological comparison between OFM and SCFM, identifies distinct demographic and site-related patterns (SCFM in older males on extremities; OFM in younger females on gingiva), and emphasizes practical implications for awareness, diagnostic accuracy, and clinical management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cohen P.R. Erickson C.P. Calame A. Case report and review of solitary cutaneous focal mucinosis: A unique primary cutaneous mucinosis unrelated to mucinosis-associated systemic diseases Dermatol. Online J.20202610.5070/D 326804988332941712 · doi ↗ · pubmed ↗
- 2Cunha J.L.S. Leite A.A. Abrantes T.d.C. Vervloet L.P. Morais T.M.d.L. Neto G.d.O.P. Kimura T.N.L. Ferreira S.M.S. de Albuquerque-Júnior R.L.C. Abrahão A.C. Oral focal mucinosis: A multi-institutional study and literature review J. Cutan. Pathol.202048243310.1111/cup.1381333410541 · doi ↗ · pubmed ↗
- 3Kuo K. Lee L. Kuo T. Solitary cutaneous focal mucinosis: A clinicopathological study of 11 cases of soft fibroma-like cutaneous mucinous lesions J. Dermatol.20164433533810.1111/1346-8138.1352327450934 · doi ↗ · pubmed ↗
- 4Tomich C.E. Oral focal mucinosis Oral Surg. Oral Med. Oral Pathol.19743871472410.1016/0030-4220(74)90392-24140487 · doi ↗ · pubmed ↗
- 5Fuchs L.D. Kirschnick L.B. Gabriel A.d.F. Silveira F.M. Lopes M.A. Wagner V.P. Schuch L.F. Martins M.D. Oral focal mucinosis: A systematic review Br. J. Oral Maxillofac. Surg.20246266967510.1016/j.bjoms.2024.05.01439107146 · doi ↗ · pubmed ↗
- 6Kumar V.V. Krishanappa S.J. Channabasaviah G.H. Kamat M.S. Prakash S.G. Oral Focal Mucinosis Int. J. Infect. Dis.20252812913110.34172/aim.3127340062502 PMC 11892092 · doi ↗ · pubmed ↗
- 7Das S. Chatterjee A. Chatterjee R.P. Sinha S. Sultana M. Shah N. Pal M. Mahmud S.A. Myxomatous Mysteries: Decoding the Oral Focal Mucinosis Cureus 202416 e 6792110.7759/cureus.6792139328633 PMC 11425983 · doi ↗ · pubmed ↗
- 8Kobayashi R. Hirai H. Maruyama S. Tanuma J.-I. Tomihara K. Oral Focal Mucinosis of the Tongue: Case Report and Review of the Literature Cureus 202416 e 6788210.7759/cureus.6788239328598 PMC 11425988 · doi ↗ · pubmed ↗