The Preoperative Waiting Time on Long-Term Survival Following Elderly Hip Fracture Surgery
Chunyuan X. Qiu, Priscilla H. Chan, Kathryn E. Royse, Ronald A. Navarro, Glenn R. Diekmann, Kent T. Yamaguchi, Elizabeth W. Paxton, Vimal Desai

TL;DR
This study finds that the time between admission and surgery affects elderly hip fracture patients' survival, with optimal timing depending on whether they take anticoagulant medications.
Contribution
The study identifies optimal preoperative wait times for elderly hip fracture patients based on anticoagulation status to minimize mortality.
Findings
Non-anticoagulated patients had lowest mortality when operated on within 6–15 hours of admission.
Anticoagulated patients showed uniform mortality risk across the first 24 hours of admission.
A U-shaped mortality trend was observed in anticoagulated patients, though breakpoints were not statistically significant.
Abstract
Background/Objective: The first-year postoperative mortality in elderly hip fracture patients is between 15 and 36%. Current scientific evidence indicates that morbidity and mortality are impacted by time of admission to surgery in hip fracture patients, although anticoagulation (AC) medication status specific optimization is unknown. Our objectives were to identify an ideal preoperative wait time by anticoagulation status in patients before hip fracture repair based on the incidence of postoperative morbidity and mortality. Methods: A total of 35,463 patients age ≥ 65 undergoing hip fracture repair were selected from a United States hip fracture registry (2009–2019). Patients were separated into strata (yes/no) based on whether they received anticoagulation (AC) medications ≤ 100 days prior to surgery. Multivariable logistic regression was adjusted for non-linear surgical wait time…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
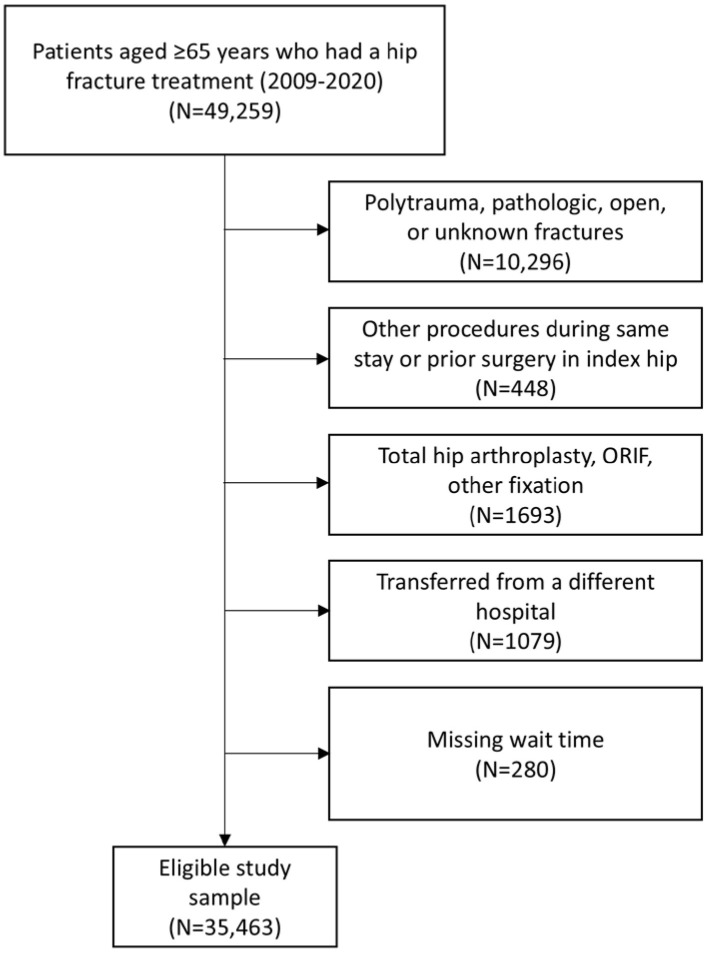 Figure 1
Figure 1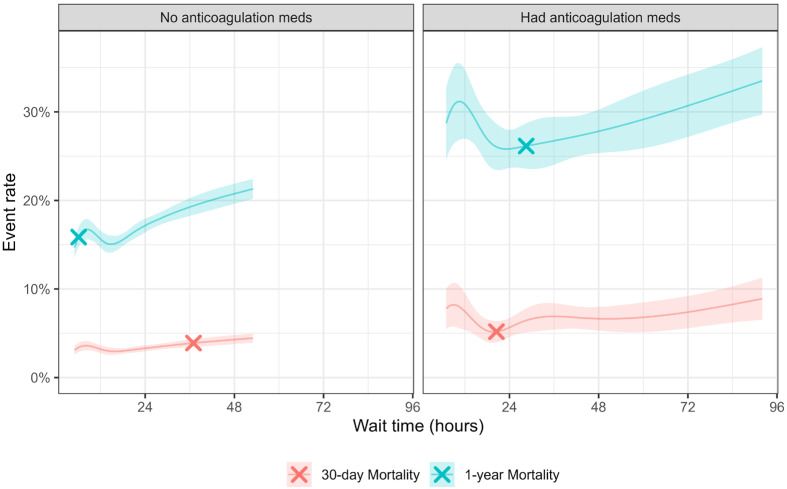 Figure 2
Figure 2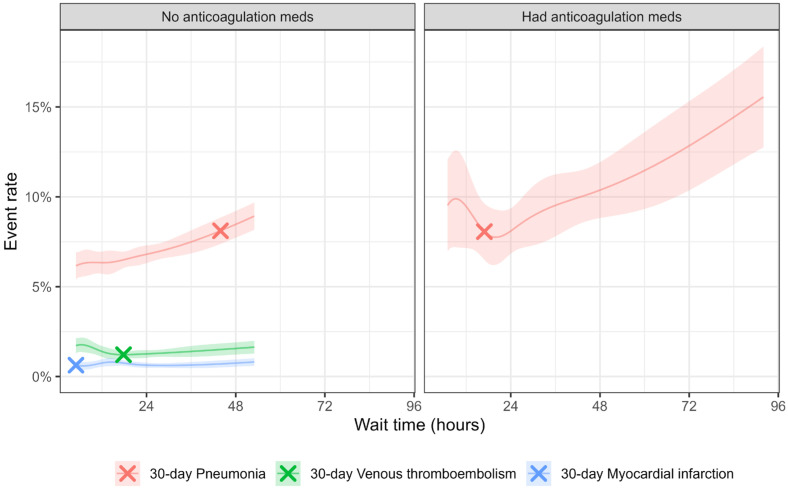 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHip and Femur Fractures · Cardiac, Anesthesia and Surgical Outcomes · Statistical Methods in Epidemiology
1. Introduction
Hip fractures affect approximately 18% of elderly women and 6% of elderly men [1]. With the rapid growth of the aging population worldwide, the number of hip fractures is projected to reach 6.26 million by 2050 [2]. Despite advances in perioperative care and team-based management, both short- and long-term outcomes remain unsatisfactory, with first-year postoperative mortality ranging from 15 to 36%, and the total annual U.S. economic burden of hip fracture surgery exceeds $30 billion [3]. These trends highlight the urgent need for strategies that improve outcomes while managing costs in an aging population.
Preoperative waiting time is a modifiable factor associated with outcomes following hip fracture surgery [4,5]. Historically, a 72 h delay for medical stabilization was considered safe [4,5], but recent evidence favors early (<24 h), super early (<12 h), or ultra-early surgery (<6 h) [6]. Current guidelines, including AAOS, recommend surgery within 24–48 h of admission, citing potentially better clinical outcomes [7]. Systematic reviews and meta-analyses have linked early surgery to lower mortality and fewer perioperative complications [8]. However, these recommendations do not fully account for patient-specific considerations. The optimal timing may vary according to comorbidities, frailty, residual functional reserve, and tolerance to surgical and anesthesia trauma, while balancing the risks of ongoing deterioration and complications from immobilization [9,10].
Coagulopathies are a particularly complex factor in elderly hip fracture patients, often arising from cardiac arrhythmias or anticoagulation therapy [11]. Correcting coagulopathies must balance surgical bleeding risk, postoperative DVT/PE risk, and potential adverse effects on underlying cardiovascular disease [12,13]. Reversal strategies are time-consuming and lack standardized guidance [14]. Some patients undergo natural reversal over several days, while others receive active reversal to enable earlier surgery and potentially improved outcomes [15]. Evidence suggests continuing antiplatelets may be safe, and early surgery after discontinuation can reduce hospital stay without increasing adverse events [16]. Large trials, including HIP ATTACK, highlight the feasibility and safety of accelerated surgery, even though mortality benefits are not definitive [17]. Interventions to improve adherence to guideline-recommended timing and early mobilization show modest improvements in early outcomes, underscoring the potential value of system-level optimization [18,19].
Despite this growing evidence, there remains a lack of specific data on how preoperative anticoagulation modifies the relationship between surgical waiting time and mortality or complications. In this retrospective total joint registry study, we evaluated patients aged 65 and older who underwent hip fracture repair in an integrated healthcare system. Our objectives were to (1) identify whether preoperative anticoagulation influences short- (30-day, 90-day) and long-term (1-year) mortality in relation to waiting time for surgery and (2) determine how waiting time impacts the incidence of pneumonia, myocardial infarction, and venous thromboembolism in patients stratified by anticoagulation status.
2. Materials and Methods
2.1. Study Design and Data Source
We conducted a retrospective cohort study using a longitudinally maintained database from a US integrated healthcare system’s hip fracture registry. This registry includes all surgically treated hip fractures performed within the integrated healthcare system, which covers over 12.6 million members. Data collection, participation, and other details of hip fracture registry details have been previously published [20]. In brief, this registry identifies patients with surgically treated hip fractures and their demographics, medical comorbidities, intraoperative details, implant information, and outcomes using electronic medical records, administrative databases, and other institutional databases within the integrated healthcare system.
2.2. Inclusion and Exclusion Criteria
Patients aged 65 years and older who underwent surgery for a hip fracture between January 2009, and December 2019 were included. We did not include data on and after January 2020 due to COVID shelter-in-place policy that could influence surgical wait time and outcomes differently [21]. To maximize data integrity, we included only cases performed in the 4 main regions (Southern California, Northern California, Northwest, Hawaii) because they are mostly non-contract facilities.
Cases were excluded if they involved patients with pathological fractures, multiple fractures, open fractures (i.e., non-low energy falls or injuries from motor vehicle accidents), procedures in conjunction with other surgeries in the same hospital stay (i.e., complicated cases unrelated to the simple fall incidence), prior hip surgeries on the same side, surgery types other than nail fixation, pinning fixation, slidescrew fixation, or hemiarthroplasty. We also excluded cases if a patient was transferred from a different hospital to the hospital where the surgery took place (3% of patients), and those with missing surgical wait time (defined below, 0.8% of patients) (Figure 1).
2.3. Surgical Wait Time
Surgical wait time is defined as hours and minutes elapsed from either emergency department or inpatient admission to the surgical start time. The surgical start time is defined as a timestamp of the first document occurrence of when the patient was in the operating room, the procedure start time, or the incision time. All timestamps were documented in the electronic health record.
2.4. Outcomes of Interest
Primary outcomes were mortality at 30 days, 90 days, and 1 year. Secondary outcomes were 30-day pneumonia, 90-day myocardial infraction (MI), and 90-day venous thromboembolism (VTE).
Mortality information was obtained from the Social Security Administration, thus capturing all patients regardless of their insurance at the time of death. Medical complications included pneumonia, acute myocardial infarction (MI), deep venous thrombosis (DVT), and pulmonary embolism (PE), were defined according to the Agency for Healthcare Research and Quality (AHRQ) quality indicators [22]. DVT and PE were manually validated by clinical content experts to ensure database accuracy, including confirmation via ultrasound and/or computed tomography reports.
2.5. Anticoagulation Medication Before Surgery Leading to a Delay
Patients who have anticoagulation medications require medically necessary steps before surgery. For consistency with other pharmacoepidemiology studies and to reduce potential exposure misclassification bias, we defined anticoagulation users as those that received an anticoagulation medication dispensed in our integrated system within 100 days preop, including the following: aspirin, apixaban, betrixaban, edoxaban, fondaparinux, rivaroxaban, danaparoid, heparin flush, dalteparin, enoxaparin, tinzaparin, bivalirudin, dabigatran, desirudin, lepirudin, warfarin, abciximab, eptifibatide, tirofiban, cangrelor, caplacizumab, cilostazol, clopidogrel, dipyridamole, prasugrel, ticagrelor, ticlopidine, and vorapaxar [23,24]. We stratified patients by preop anticoagulation (AC) medication status (yes/no) in this study [3,4].
2.6. Covariates
Patient characteristics included age, sex (male vs. female), American Society of Anesthesiologists (ASA) score (III/IV/V vs. I/II), body mass index (BMI) (per 1 increment), smoking status (current, previous vs. never), diabetes (yes vs. no), and 90-day preop acute myocardial infraction (yes vs. no). We assessed the following Elixhauser’s comorbidities [5] (yes vs. no): chronic pulmonary disease, congestive heart failure, hypertension, psychoses, and renal failure. Surgical characteristics included anesthesia type (neuraxial, others, vs. general), surgery type (pinning, slidescrew, hemi vs. nail). We adjusted for variation observed in hospital volume [6] (low (0 to 124 cases per year), medium (125 to 186 cases per year), vs. high (≥187 cases per year), region (Southern California, Northwest, Hawaii vs. Northern California), and yearly trend (operative year per 1 year increment).
2.7. Statistical Analysis
Within each AC status strata, wait time was modeled flexibly using restricted cubic splines with knots at pre-specified percentiles of the distribution at 5, 27.5, 50, 72.5, and 95th percentiles [7,25] using restricted cubic spline and multivariable logistic regression models. Non-linearity was assessed with a likelihood ratio test. Model calibration and collinearity diagnostics confirmed adequate model fit and stability. We assessed any breakpoint for any change in slope with the Davies test [26] on data with wait times within 1st to 95th percentile. The longest 5% wait time was excluded at this step to minimize the influence of extreme wait time outliers on the linear trend from extrapolation. Fitted smooth curve vs. wait time, estimated breakpoint, and the slopes before and after breakpoint were presented.
Missing values were handled using mean imputation in the following covariates: (ASA N = 2114 (6.0%), BMI N= 201 (0.6%), smoking status N= 622 (1.8%), chronic pulmonary disease N = 8 (<0.1%), congestive heart failure N = 8 (<0.1%), hypertension N = 8 (<0.1%), psychoses N = 8 (<0.1%), renal failure N = 8 (<0.1%), and anesthesia type N = 160 (0.5%). Analyses were performed using R version 3.6.2. p < 0.05 was the statistical significance threshold used for this study, and all tests were 2-sided.
2.8. Sensitivity Analysis
We repeated the analysis and further stratified by the combination of AC groups and anesthesia type (general or neuraxial); we excluded ‘other’ as an anesthesia type group due to the difficulty of interpretation due to heterogeneity in this category.
3. Results
A total of 35,463 patients were identified in the study period, and procedures were performed by 546 surgeons at 35 hospitals. For the overall cohort, the median patient age was 83 years, and 30.2% were male (Table 1).
3.1. Patients Without Preoperative Anticoagulation Medications
87.1% (N = 30,902) of the total sample were not prescribed AC preoperatively; the median patient age was 83 years, 29.4% were male, and 74.0% had an ASA score of 3 or greater (Table 1). Median surgical wait time was 20.3 h (IQR: 13–27 h). The crude mortality rate was 5.1%, 10.7%, and 20.8% at 30 days, 90 days, and 1 year, respectively. A significant positive linear trend was observed after 15.5 h wait time for 30 day mortality (log odds ratio = 0.97, 95%CI 0.30–1.64), before 43.4 h wait for 90 days mortality (log odds ratio = 1.17, 95%CI 0.74–1.61), and after 6.1 h wait for 1 year mortality (log odds ratio = 0.87, 95%CI 0.57–1.16) (Table 2, Figure 2).
For 30-day pneumonia, an increased rate was observed before 43.9 h of wait (log odds ratio = 0.69, 95%CI 0.21–1.17). A flat line trend was observed for 90-day VTE and 90-day MI, with breakpoints at 15.3 and 14.3 h, respectively, though slopes before and after breakpoints were not significantly different from zero (Figure 3).
3.2. Patients with Preoperative Anticoagulation Medications
12.9% (N = 4561) of the total sample had AC preoperatively, with a median age of 84 years, 35.5% were male, and 89.7% had an ASA score of 3 or greater. Their median wait time was 26.2 h (IQR 18–44 h). The crude mortality rate was 8.3%, 16.3%, and 30.5% at 30 days, 90 days, and 1 year, respectively.
After controlling for covariates, the model fitted curve showed a “U”-shaped trend in 30 day, 90 day, and 1 year mortality rates vs. wait time, with the lowest at 22.5 h (Figure 1). Breakthrough point was observed at 20.5, 22.4, and 28.5 h of wait time for 30 days, 90 days, and 1 year mortality, respectively (Table 2). All slopes before the breakpoint were negatively correlated (i.e., higher mortality rate with shorter wait time before the breakpoint), while slopes after the breakpoint were positively correlated (i.e., higher mortality rate with longer wait time after the breakpoint), though slopes before and after the breakpoint were not significantly different from zero.
For 30 days of pneumonia vs. wait time, a “U”-shaped trend was observed with a significant increase after 16.9 wait hours (log odds ratio = 0.77 for every increment of 1 h wait, 95%CI 0.13–1.41). A flat line trend was observed for VTE and MI, with breakpoints at 68.7 and 16.2 h, respectively, though slopes before and after breakpoints were not significantly different from zero.
4. Discussion
In this retrospective cohort study using a well-established total joint registry from a large integrated healthcare system, we found that the timing of hip surgery can impact patient 90 day and 1 year mortality. In non-anticoagulated patients, the 90-day mortality progressively increased when the preoperative waiting time was more than 15.5 h. A shorter preoperative waiting time (approximately 6.1 h) was associated with better 1-year survival. In anticoagulated patients, early or late surgery was associated with higher mortality, with the inflection point at 22.4 h for 90-day mortality and 28.5 h for 1-year mortality. While earlier surgical intervention can benefit some patients, especially those without coagulopathy, this approach may not be desirable for anticoagulated patients. We found that optimal preoperative waiting time was not a fixed point but a dynamic variable.
Many guidelines support early surgical intervention, defined as within 24–48 h. However, a shorter preoperative waiting time has been suggested or even preferred, as it may reduce length of hospital stay, morbidity, and mortality [18]. In a retrospective Canadian study involving 42,230 patients, surgery within 24 h demonstrated significantly lower 30-day mortality, and surgery within 6 h may benefit patients even more. However, this observation was not substantiated by the HIP ATTACK study, which was limited to outcomes up to 90 days following surgery [19]. Using long-term survival data in this study, we found that ultra-early surgical intervention close to 6 h in non-anticoagulated hip fracture patients was associated with reduced 90 day and 1 year mortality, but only in non-anticoagulated patients. This finding of long-term survival benefits for early surgery is notable because causes of death in the perioperative period and later stages often differ. Unlike 30 day mortality, which is often due to pneumonia, sepsis, and MI, later deaths are often due to decompensating chronic diseases such as cardiovascular disease, cancer, aging, or neurocognitive deterioration. Increasing evidence suggests that patients who experience eventful and prolonged perioperative courses, especially in the presence of delirium, are at accelerated risk of physical, functional, and cognitive decompensation and death in the later stage. In non-anticoagulated patients, early surgical interventions, often characterized by more frequent use of regional anesthesia and analgesia, can facilitate early ambulation, feeding, and rehabilitation. Additionally, regional anesthesia and analgesia can provide more effective pain control with reduced narcotic use. We previously reported that more frequent use of regional anesthesia and analgesia is associated with lower perioperative mortality.
The presence of anticoagulants in elderly hip fracture patients is considered a warning sign for higher perioperative morbidities and mortalities, occurring in approximately 10% of patients. This warning often reflects advanced cardiovascular disease such as atrial fibrillation, valvular disease, CHF, or recent MI. Co-management of cardiovascular disease and coagulopathy in these patients is extremely challenging. First, current guidelines for perioperative management of anticoagulants for elective surgery are often not applicable to urgent hip fracture patients; second, the process of anticoagulation to coagulation reversal to anticoagulation carries risk because both bleeding and thrombotic events can occur simultaneously. Consequently, practices are heterogeneous with varied outcomes. In our study, patients with coagulopathy had higher mortality than patients without anticoagulation (16.3% vs. 10.7% for 90-day mortality, 30.5% vs. 20.8% for 1-year mortality). Patients on anticoagulants also waited longer for surgery compared to the non-anticoagulant group (35.7 ± 33.3 vs. 23.8 ± 20.0 h), which is shorter for both groups compared to literature (47 vs. 29 h) [16]. Interestingly, preoperative waiting time in anticoagulated hip fracture patients exhibited a biphasic pattern for 90-day and 1-year mortality. The “U-shaped” curve, where early or late surgery was associated with higher mortality, implies that stress accommodation or resistance to secondary trauma imposed by mandatory surgery and anesthesia can change quickly, and the window of opportunity is narrowed in this vulnerable group. A similar pattern was observed for postoperative MI and pneumonia, with an understandable absence of VTE.
This study derives from a well-recognized, longitudinally maintained total joint registry based on a comprehensive electronic medical record rather than an administrative database from an integrated healthcare delivery system. To our knowledge, this is the first study to illustrate the dynamic characteristics of preoperative waiting time on long-term mortality and morbidity following elderly hip fracture surgery.
Our study has several limitations. Although we adjusted for many potential confounders, residual confounding due to unmeasured variables may remain due to the retrospective design. We used admission time rather than fractured time, which is often unknown. The cause of death was not investigated, which may further elucidate the impact of preoperative waiting time. Preoperative waiting time may also serve as a surrogate for the quality of patient-centered multidisciplinary teamwork rather than simple surgical decisions. Additionally, this study lacks external validation, and institutional factors—including operating room (OR) availability, surgical scheduling, and anesthesia provider availability—may have influenced outcomes.
5. Conclusions
Preoperative waiting time following an elderly hip fracture is linked to long-term survival. However, this window of opportunity for optimal outcomes is short and dynamic, dependent on baseline medical conditions and anticoagulation status. In non-anticoagulated patients, the window is between 6 and 15 h. In anticoagulated patients, it is shorter, between 22 and 29 h. These findings, which should be confirmed by future research studies, highlight the importance of individualized timing for hip fracture surgery, considering medical comorbidities, anticoagulation status, and institutional factors such as OR and anesthesia provider availability, to optimize both short- and long-term outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cooper C. Campion G. Melton L.J.3rd Hip fractures in the elderly: A world-wide projection Osteoporos. Int.1992228528910.1007/BF 016231841421796 · doi ↗ · pubmed ↗
- 2Cooper C. Cole Z.A. Holroyd C.R. Earl S.C. Harvey N.C. Dennison E.M. Melton L.J. Cummings S.R. Kanis J.A. Secular trends in the incidence of hip and other osteoporotic fractures Osteoporos. Int.2011221277128810.1007/s 00198-011-1601-621461721 PMC 3546313 · doi ↗ · pubmed ↗
- 3Morri M. Ambrosi E. Chiari P. Magli A.O. Gazineo D. Alessandro F.D. Forni C. One-year mortality after hip fracture surgery and prognostic factors: A prospective cohort study Sci. Rep.201991871810.1038/s 41598-019-55196-631822743 PMC 6904473 · doi ↗ · pubmed ↗
- 4Bhatti U.F. Shah A.A. Williams A.M. Biesterveld B.E. Okafor C. Ilahi O.N. Alam H.B. Delay in Hip Fracture Repair in the Elderly: A Missed Opportunity Towards Achieving Better Outcomes J. Surg. Res.202126614214710.1016/j.jss.2021.03.02733992000 · doi ↗ · pubmed ↗
- 5Van Voorden T.A. Hartog D.D. Soesman N.M. Jakma T.S. Waleboer M. Staarink M. Bruijninckx M.M. Nijman F. Knops S.P. Van Lieshout E.M. Effect of the Dutch Hip Fracture Audit implementation on mortality, length of hospital stay and time until surgery in elderly hip fracture patients; a multi-center cohort study Injury 2020511038104410.1016/j.injury.2020.02.08432115205 · doi ↗ · pubmed ↗
- 6Viamont-Guerra M.-R. Guimarães R. Bridges C. Antonioli E. Lenza M. Ultra-early versus early surgery for hip fracture Cochrane Database Syst. Rev.20242024 CD 01569710.1002/14651858.cd 015697 PMC 1117067839804112 · doi ↗ · pubmed ↗
- 7O’C Onnor M.I. Switzer J.A. AAOS Clinical Practice Guideline Summary: Management of Hip Fractures in Older Adults J. Am. Acad. Orthop. Surg.202230 e 1291 e 129610.5435/JAAOS-D-22-0012536200817 · doi ↗ · pubmed ↗
- 8Klestil T. Röder C. Stotter C. Winkler B. Nehrer S. Lutz M. Klerings I. Wagner G. Gartlehner G. Nussbaumer-Streit B. Impact of timing of surgery in elderly hip fracture patients: A systematic review and meta-analysis Sci. Rep.201881393310.1038/s 41598-018-32098-730224765 PMC 6141544 · doi ↗ · pubmed ↗