Heterogeneity in the association between retirement and cognitive function: a machine learning analysis across 19 countries
Koryu Sato, Haruko Noguchi, Kosuke Inoue

TL;DR
This study finds that retiring can improve cognitive function, but the benefits vary based on factors like gender and health.
Contribution
The study introduces a machine learning approach to analyze how retirement affects cognitive function across different populations.
Findings
Retirees recalled 1.348 more words than workers on average.
Women and those with higher socioeconomic status showed greater cognitive benefits from retirement.
Pre-retirement health and physical activity were linked to better cognitive outcomes after retirement.
Abstract
Rising state pension ages in many developed countries may influence cognitive aging by delaying retirement, yet the cognitive consequences of retirement likely vary across individuals and contexts. This study investigates the heterogeneous association between retirement and cognitive function. We analyzed harmonized data from three longitudinal studies: the Health and Retirement Study, the English Longitudinal Study on Ageing, and the Survey of Health, Ageing and Retirement in Europe. The dataset encompassed three waves across 19 counties from 2014 to 2019. Our study included 12 811 individuals who worked in the first wave, from whom each survey collected covariate information. We assessed retirement status among participants aged 50–80 years in the second wave and measured cognitive function using word recall tests in the third wave. The analysis employed instrumental variable causal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
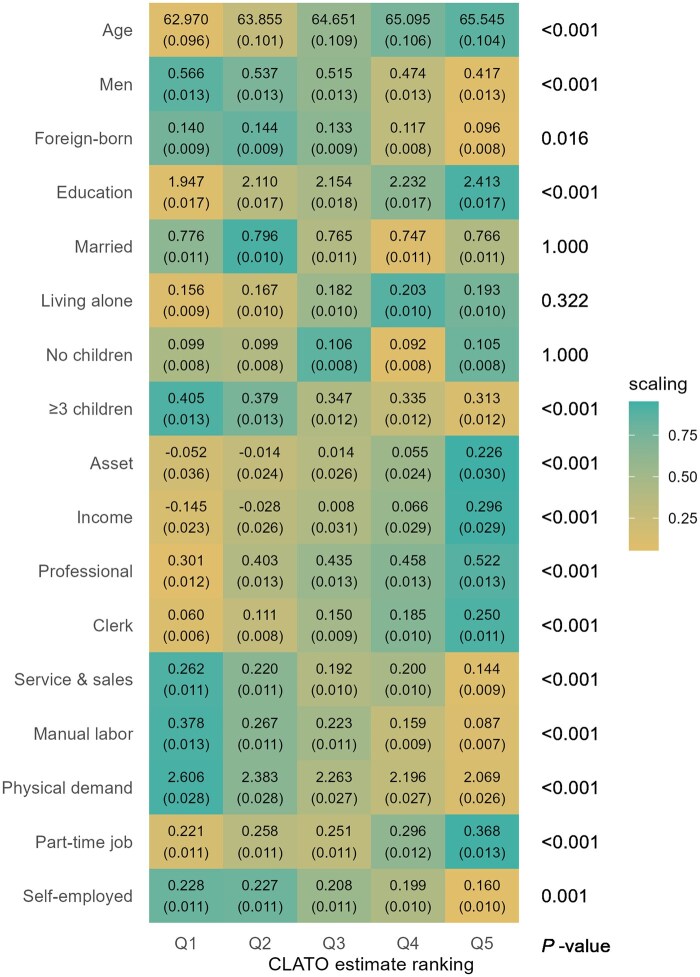 Figure 1
Figure 1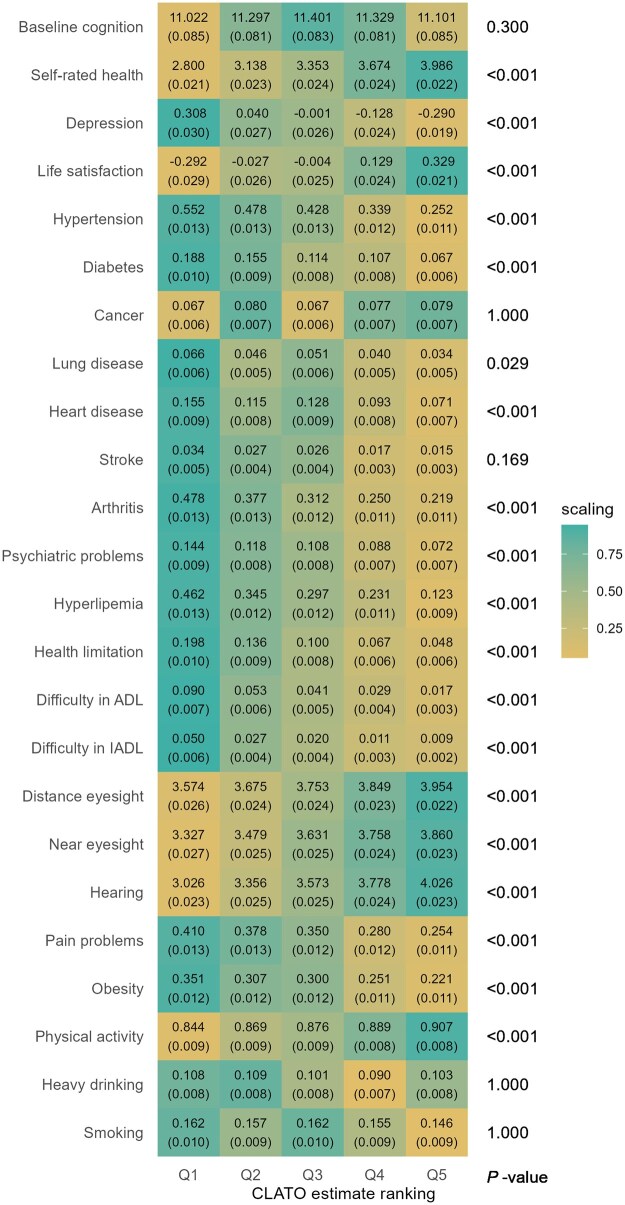 Figure 2
Figure 2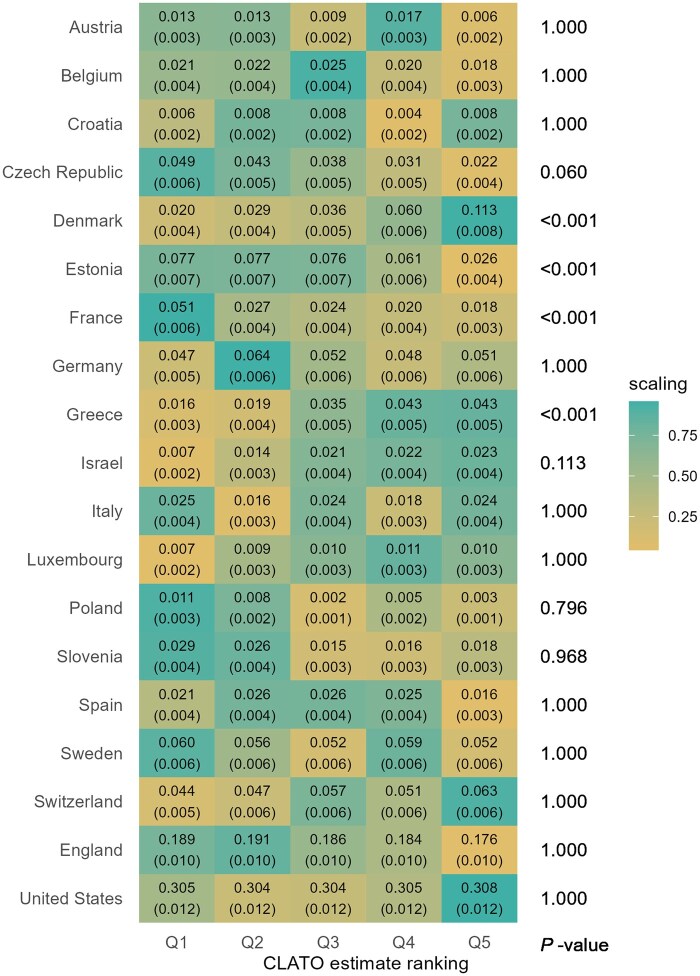 Figure 3
Figure 3| Variables, | Worker | Retiree |
|---|---|---|
| Sociodemographic characteristics | ||
| Age (years), mean (SD) | 63.9 (3.86) | 65.8 (4.27) |
| Men | 2667 (50.6) | 1063 (49.1) |
| Foreign-born | 707 (13.4) | 230 (10.6) |
| Education, mean (SD) | 2.2 (0.68) | 2.1 (0.69) |
| Married | 4059 (77.1) | 1663 (76.8) |
| Living alone | 934 (17.7) | 406 (18.8) |
| No children | 544 (10.3) | 200 (9.2) |
| ≥3 children | 1885 (35.8) | 760 (35.1) |
| Asset, z-score, mean (SD) | 0.1 (1.21) | 0.0 (0.79) |
| Income, z-score, mean (SD) | 0.1 (1.14) | 0.0 (0.91) |
| Professional | 2272 (43.1) | 878 (40.6) |
| Clerk | 793 (15.1) | 329 (15.2) |
| Service and sales | 1067 (20.3) | 446 (20.6) |
| Manual labor | 1140 (21.6) | 515 (23.8) |
| Physical demand, mean (SD) | 2.3 (1.07) | 2.3 (1.05) |
| Part-time job | 1298 (24.6) | 775 (35.8) |
| Self-employed | 1151 (21.9) | 368 (17.0) |
| Health and behaviors | ||
| Baseline cognition, mean (SD) | 11.3 (3.19) | 11.0 (3.26) |
| Self-rated health, mean (SD) | 3.4 (0.98) | 3.3 (0.95) |
| Depression, z-score, mean (SD) | 0.0 (1.01) | 0.0 (0.97) |
| Life satisfaction, z-score, mean (SD) | 0.0 (1.00) | 0.1 (0.98) |
| Hypertension | 2064 (39.2) | 982 (45.4) |
| Diabetes | 626 (11.9) | 311 (14.4) |
| Cancer | 372 (7.1) | 177 (8.2) |
| Lung disease | 231 (4.4) | 122 (5.6) |
| Heart disease | 571 (10.8) | 265 (12.2) |
| Stroke | 107 (2.0) | 69 (3.2) |
| Arthritis | 1633 (31.0) | 800 (37.0) |
| Psychiatric problems | 542 (10.3) | 244 (11.3) |
| Hyperlipemia | 1534 (29.1) | 634 (29.3) |
| Health limitations in working | 526 (10.0) | 291 (13.4) |
| Difficulty in ADL | 205 (3.9) | 137 (6.3) |
| Difficulty in IADL | 129 (2.4) | 45 (2.1) |
| Distance eyesight, mean (SD) | 3.8 (0.94) | 3.8 (0.92) |
| Near eyesight, mean (SD) | 3.6 (0.98) | 3.6 (0.97) |
| Hearing, mean (SD) | 3.6 (1.00) | 3.5 (0.99) |
| Pain problems | 1702 (32.3) | 783 (36.2) |
| Obesity | 1515 (28.8) | 612 (28.3) |
| Physical activity | 4629 (87.9) | 1888 (87.2) |
| Heavy drinking | 524 (9.9) | 237 (10.9) |
| Smoking | 795 (15.1) | 369 (17.0) |
| Countries | ||
| Austria | 50 (0.9) | 37 (1.7) |
| Belgium | 99 (1.9) | 58 (2.7) |
| Croatia | 37 (0.7) | 14 (0.6) |
| Czech Republic | 147 (2.8) | 126 (5.8) |
| Denmark | 291 (5.5) | 92 (4.2) |
| Estonia | 379 (7.2) | 93 (4.3) |
| France | 123 (2.3) | 86 (4.0) |
| Germany | 262 (5.0) | 128 (5.9) |
| Greece | 182 (3.5) | 49 (2.3) |
| Israel | 100 (1.9) | 30 (1.4) |
| Italy | 121 (2.3) | 37 (1.7) |
| Luxembourg | 44 (0.8) | 27 (1.2) |
| Poland | 31 (0.6) | 13 (0.6) |
| Slovenia | 94 (1.8) | 60 (2.8) |
| Spain | 108 (2.1) | 61 (2.8) |
| Sweden | 263 (5.0) | 152 (7.0) |
| Switzerland | 276 (5.2) | 115 (5.3) |
| England | 974 (18.5) | 403 (18.6) |
| United States | 1686 (32.0) | 584 (27.0) |
| Outcome | ||
| Cognitive function, mean (SD) | 11.1 (3.21) | 10.8 (3.19) |
| (1) OLSa | (2) 2SLSa | (3) Non-IV forests | (4) IV forests | |
|---|---|---|---|---|
| Retirement | −0.013 | 0.962 | −0.031 | 1.348 |
| 95% CI | (−0.150 to 0.123) | (0.287 to 1.637) | (−0.171 to 0.108) | (0.313 to 2.384) |
| Observations | 7432 | 7432 | 7432 | 7432 |
| F statistic | 163.037 | |||
| Sargan statistic | 1.177 |
- —Japan Society for the Promotion of Sciences
- —Health Care Science Institute Research
- —National Institute on Aging10.13039/100000049
- —National Institute on Aging10.13039/100000049
- —University of Michigan10.13039/100007270
- —Japan Society for the Promotion of Science10.13039/501100001691
- —Japan Science and Technology
- —Japan Agency for Medical Research and Development10.13039/100009619
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRetirement, Disability, and Employment · Financial Literacy, Pension, Retirement Analysis · Technology Use by Older Adults
Introduction
The cognitive health of older adults is a growing global concern. Cognitive decline, particularly in episodic memory, often represents an early stage in the neurodegenerative process that, if progressive and accompanied by deficits in other cognitive domains, can eventually lead to dementia [1]. In 2015, approximately 47 million people were living with dementia, with projections indicating a 1.6-fold increase to 75 million by 2030 [2]. In response to rapidly aging populations, many developed countries are raising their state pension age (SPA). These policy changes may affect cognitive health by delaying retirement, thereby altering individuals’ budgetary constraints and time allocation between work and leisure in later life [3].
Despite numerous studies using identical datasets, the effects of retirement on cognition remain uncertain, with no clear consensus emerging [4, 5]. For example, studies using Health and Retirement Study (HRS) data have yielded contradictory findings, with some demonstrating a detrimental association of retirement with cognitive function [6, 7], whereas others show no association [8]. Similarly, research utilizing data from the English Longitudinal Study on Ageing (ELSA) or the Survey of Health, Ageing and Retirement in Europe (SHARE) has produced inconsistent results. While several studies reported harmful associations [9, 10], others found no relationship [11–14], and some even suggested beneficial associations [15, 16].
Several factors may contribute to these inconsistencies in the literature. First, model misspecification can influence effect estimates. A review replicating previous studies demonstrated that the choice of statistical methodologies is a key determinant of findings [5]. Additionally, effect heterogeneity introduces another source of variation. Studies have shown that the association between retirement and cognitive function varies by individual characteristics such as sex, education, and pre-retirement occupation [10, 12, 17–20]. When adverse effects in one subgroup mask positive effects in others, the overall population treatment effect becomes ambiguous. Nonetheless, the full extent of heterogeneity in this relationship remains poorly understood.
To address these challenges, we applied instrumental variable causal forests (IV forests) [21] to investigate the conditional average treatment effect (ATE) of retirement on cognitive function. We employed country-specific SPA as an instrument for retirement to address the endogenous nature of retirement decisions. The IV forests method incorporates random-forest-based nonparametric estimation, offering greater robustness against model misspecification compared to conventional parametric approaches. Our analysis utilized harmonized data from 19 countries and incorporated 60 covariates as potential confounders and effect modifiers. This machine learning-based approach enables us to uncover previously hidden effect heterogeneity in the association between retirement and cognitive function.
Methods
Study design and participants
This study used harmonized panel datasets from the HRS, ELSA, and SHARE provided by the Gateway to Global Aging Data project [22]. Our data encompassed three waves: covariates (excluding age) were obtained from the HRS and ELSA in 2014 and SHARE in 2015; age and labor force status were ascertained via the HRS and ELSA in 2016 and SHARE in 2017; and cognitive function outcomes were assessed in the HRS and ELSA in 2018 and SHARE in 2019. To prevent retirement from influencing covariates, we collected covariate information from the wave preceding retirement status measurement. Furthermore, we measured outcomes at least 2 years after retirement, acknowledging the potential temporal lag in retirement’s impact on cognitive function [12].
Among 94 824 individuals who participated in the first wave, 49 555 completed all three waves. We included 43 052 individuals aged 50–80 years from the second wave, but excluded 29 519 individuals who were not working in the first wave and 722 individuals who neither worked nor retired in the second wave (e.g. unemployed, disabled, or homemaker). The final sample comprised 12 811 participants for IV forests development (Supplementary Fig. S1). To assess the potential impact of attrition, we compared baseline characteristics between included and excluded individuals (12 033 individuals who aged under 78 years and worked in the first wave but were excluded from the analysis). Supplementary Table S1 shows that there was no difference in the baseline cognitive function between included retirees and excluded individuals.
Cognitive function assessment
Episodic memory was assessed as a measure of cognitive function. Episodic memory involves the ability to recall past experiences, which typically declines with age [23]. The assessment followed the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) Battery protocol [24]. Participants listened to 10 common words and were immediately asked by an interviewer to recall as many words as possible. After approximately 5 minutes, they were asked to recall the words again. Hence, the total number of words recalled, ranging from 0 to 20, represented their episodic memory function, consistent with previous studies [5–8, 10–13, 15, 16].
Retirement status classification
Labor force status was self-reported in the surveys (Supplementary Method S1). We focused on individuals who were working during the first wave. In the second wave, we defined retirees as those who self-identified as “retired” or “partly retired,” regardless of current working status, aligning with previous literature (Supplementary Table S2) [15, 17, 20, 25]. While some studies have defined retirement simply as not working [6, 10, 11, 14], we tested our findings’ robustness using this narrower definition.
State pension age implementation
To address potential endogenous retirement decision bias, we employed the SPA as an IV for retirement (Supplementary Table S3). Following previous research [11, 20, 25, 26], we used joint instruments including the early retirement age (ERA) and official retirement age (ORA). The binary ERA variable indicated whether participants had reached the earliest age for receiving reduced or full pension benefits under specific conditions. The ORA variable denoted whether participants had reached the age for receiving a minimum guaranteed or full pension without conditions. For countries without early retirement schemes, the ERA variable was set to zero.
The SPA serves as a valid IV by increasing retirement probability (relevance condition) without directly affecting cognition (exclusion restriction condition). Assuming monotonicity, the point estimate represents a local ATE among individuals who would retire upon reaching SPA. Our study leverages within-country SPA variations (institutional differences across birth cohorts and sexes) and between-country variations using harmonized data. Retirement rates demonstrably increase around the SPA (Supplementary Figs S2 and S3), supporting the relevance condition.
Statistical analysis
We compared ATEs using parametric ordinary least squares (OLS), two-stage least squares (2SLS), nonparametric causal forests without IVs (non-IV forests), and IV forests. For parametric methods, we adjusted for 10 covariates selected by importance in trained IV forests. ATEs for nonparametric methods were obtained through residual-on-residual regressions [27].
The IV forests method combines the generalized method of moments for IV estimation with random forests to identify similar treatment effects (Supplementary Method S2). The IV forests incorporated 60 harmonized covariates from the first wave (Supplementary Tables S4 and S5). To mitigate potential reverse causality, we included the baseline score of cognitive function. Missing values were imputed using a random forests-based algorithm [28], assuming data missing at random (Supplementary Table S6). After training, we restricted the analysis to 7432 individuals with retirement propensity scores between 0.1 and 0.9 [29], as extreme scores destabilize estimation. Our estimand of the IV forests represents the conditional local ATE on the overlap population (CLATO).
We then categorized observations into quintiles from Q1 (the lowest CLATO; least retirement benefits) to Q5 (highest CLATO; most retirement benefits), and compared sociodemographic characteristics, health and behaviors, and countries across quintiles. P-values were adjusted using the Bonferroni method. All analyses were performed using R 4.1.3 (R Foundation for Statistical Computing, Vienna, Austria).
Sensitivity analyses
We performed several sensitivity analyses to confirm the robustness of our findings. These included: restricting the sample to ages 55–75, excluding partially retired individuals, analyzing only full-time employees, and excluding US data with the largest number of samples.
Results
Descriptive statistics
The study population comprised 7432 individuals, of whom 2165 (29.1%) were retirees in the second wave (Table 1). On average, workers could recall 11.1 words, while retirees could recall 10.8 words in the third wave. The outcome showed a normal distribution (Supplementary Fig. S4).
Association between retirement and cognitive function
Initial analyses using OLS and non-IV forests revealed no evidence of the association between retirement and cognitive function (Table 2). However, 2SLS presented a positive association between retirement and word recall (0.962, 95% confidence interval [CI]: 0.287–1.637). The validity of our IVs was supported by an F statistic of 163.037 (*P *< .0001) and a Sargan statistic of 1.177 (*P *= .28). IV forests corroborated these findings, indicating that retirees recalled 1.348 more words than workers (95% CI: 0.313–2.384). Variable importance metrics from the IV forests are presented in the Supplementary Fig. S5.
Heterogeneity across individual characteristics and countries
The distribution of conditional ATEs, detailed in the Supplementary Fig. S6, showed marked differences between non-IV and IV forests. While non-IV forest estimates clustered around zero, IV forest estimates exhibited heterogeneous distribution. The ATEs increased monotonically with CLATO ranking from Q1 to Q5, suggesting that IV forests captured heterogeneity in retirement’s effect on cognitive function (Supplementary Fig. S7).
Analysis of sociodemographic characteristics across CLATO quintiles shown in Fig. 1 revealed distinct patterns. Individuals in the highest CLATO group (Q5) were more likely to be older, female, native-born, and have fewer than three children compared to those in the lowest group (Q1). They also demonstrated higher education levels and greater assets and income. Occupationally, clerks, professionals, and part-time workers were more prevalent in the highest group, whereas service workers, sales personnel, manual laborers, those in physically demanding jobs, and the self-employed were more commonly represented in the lowest group.
Heterogeneity in sociodemographic characteristics. Q1 represents the group with the lowest conditional local average treatment effect on the overlap population (CLATO), whereas Q5 represents the group with the highest CLATO. Each tile indicates the mean value of a covariate within the group, with its standard deviation in parentheses. “Scaling” assigns 1 (green) to the maximum value and 0 (yellow) to the minimum value for each variable with a color gradient. Compared to the group with the lowest benefit from retirement (Q1), the group with the highest benefit (Q5) includes more older people (mean age: 65.5 vs. 63.0) and fewer men (% of men: 0.42 vs. 0.57). Asset and income are standardized to z-scores. P-values of F-statistics are adjusted using the Bonferroni method.
Health and well-being metrics also showed variation across CLATO groups (Fig. 2). The highest CLATO group reported better self-rated health, life satisfaction, eyesight, and hearing. Conversely, the lowest CLATO group showed a higher prevalence of various health conditions, including depressive symptoms, hypertension, diabetes, lung and heart diseases, arthritis, psychiatric problems, hyperlipidemia, work limitations, difficulties in activities of daily living (ADL) and instrumental ADL (IADL), and pain-related problems. Obesity was more common in the lowest CLATO group, while regular physical activity was associated with the highest group.
Heterogeneity in health and behaviors. Q1 represents the group with the lowest conditional local average treatment effect on the overlap population (CLATO), whereas Q5 represents the group with the highest CLATO. Each tile indicates the mean value of a covariate within the group, with its standard deviation in parentheses. “Scaling” assigns 1 (green) to the maximum value and 0 (yellow) to the minimum value for each variable with a color gradient. Compared to the group with the lowest benefit from retirement (Q1), the group with the highest benefit (Q5) includes more people with higher self-rated health (mean score: 4.0 vs. 2.8) and fewer people with hypertension (% of having hypertension: 0.25 vs. 0.55). Depression and life satisfaction are standardized to z-scores. P-values of F-statistics are adjusted using the Bonferroni method.
In Fig. 3, geographic analysis revealed that individuals from Denmark and Greece were more likely to fall into higher CLATO groups, whereas those from Estonia and France typically belonged to lower CLATO groups. Age-related analysis showed CLATO estimates increased until age 65 before plateauing. Individuals with average or below-average assets and income showed greater CLATO variations, while those with higher assets and income typically maintained higher CLATO values (Supplementary Fig. S8).
Heterogeneity in countries. Q1 represents the group with the lowest conditional local average treatment effect on the overlap population (CLATO), whereas Q5 represents the group with the highest CLATO. Each tile indicates the mean value of a covariate within the group, with its standard deviation in parentheses. “Scaling” assigns 1 (green) to the maximum value and 0 (yellow) to the minimum value for each variable with a color gradient. Compared to the group with the lowest benefit from retirement (Q1), the group with the highest benefit (Q5) includes more people from Denmark (% of Danish: 0.11 vs. 0.02) and fewer people from France (% of French: 0.02 vs. 0.05). P-values of F-statistics are adjusted using the Bonferroni method.
Sensitivity analyses
Sensitivity analyses maintained the robustness of our findings across various specifications (Supplementary Table S7). These included: restricting the sample to ages 55–75 (Model 1), excluding partially retired individuals (Model 2), analyzing only full-time employees (Model 3), and excluding US data with the largest number of samples (Model 4). ATE estimates remained consistent with our main findings across all specifications.
Discussion
This study examined the heterogeneous relationship between retirement and cognitive function using harmonized data from 19 countries. Our findings revealed enhanced cognitive function among retirees compared to workers, with conditional ATEs varying according to individual characteristics and countries.
The association observed in our study contrasts with previous research suggesting cognitive decline post-retirement [6, 7, 9, 10], while aligning with studies indicating beneficial associations [15, 16]. The absence of associations in OLS and non-IV forests analyses highlights the importance of methodological choice, suggesting potential negative bias due to health-related selection into retirement. The IV forests method, with its data-driven, nonparametric features, offers greater robustness against model misspecification compared to conventional parametric approaches. The observed improvement of 1.348 words in IV forests represents a substantial effect, corresponding to a 0.42 SD in outcome distribution. According to a systematic review for the effect size of educational interventions on cognition, that of over 0.2 SD is meaningful from a public health perspective [30]. Several mechanisms may explain cognitive enhancement post-retirement. Job strain, a recognized risk factor for cognitive decline [31], is eliminated upon retirement, reducing psychosocial stress. Additionally, retirees can dedicate more time to health-promoting behaviors, such as increased physical activity, improved sleep quality, and smoking cessation [32], which are protective against cognitive decline.
The association between retirement and cognitive function demonstrated notable heterogeneity. Women showed greater cognitive benefits from retirement than men, consistent with evidence indicating women’s higher likelihood of maintaining physical and mental health through post-retirement exercise [17, 20]. Similarly, individuals who exercised before retirement were more likely to experience cognitive benefits, suggesting the importance of pre-existing health behaviors maintained into retirement.
Our findings align with the Grossman model [3], particularly regarding socioeconomic factors. Individuals with higher education, assets, and income demonstrated greater retirement benefits. The model suggests that while retirees have more time but reduced budgets for health investments, those with high socioeconomic status can better afford cognitive health investments. Additionally, better pre-retirement health correlated with enhanced post-retirement cognitive function, consistent with the model’s prediction that healthier individuals have more time for health investments. This relationship between pre-retirement health limitations and post-retirement cognitive function supports previous empirical research [33].
Occupational characteristics influenced retirement outcomes. Professionals showed greater cognitive benefits compared to those retiring from manual labor and physically demanding jobs, supporting previous research linking retirement from complex, mentally demanding occupations to slower cognitive decline [18, 19]. Conversely, retirement from physically demanding jobs showed fewer cognitive benefits, aligning with studies associating such occupations with increased dementia risk [34, 35]. This pattern may reflect the combination of high physical demands with low job control, resulting in reduced cognitive stimulation [14], suggesting workplace cognitive stimulation influences post-retirement cognitive outcomes.
Several limitations warrant consideration. First, our analysis focused on short-term effects, measuring cognitive function two years post-retirement. While previous SHARE research showed early retirement benefits, it also indicated potential negative effects of late [16]. Further research on long-term effects is needed. Second, our heterogeneity analysis was exploratory, with potential confounding between variables, such as education and occupation. Third, despite including 60 candidate variables, unmeasured factors like traumatic brain injury, social isolation, and air pollution might influence retirement’s effect on cognitive function [36]. Fourth, self-reported data may introduce measurement errors though word recall tests have demonstrated predictive validity for dementia onset [37]. Fifth, findings may not generalize beyond Western countries, highlighting the need for comparable studies in rapidly aging Asian nations. Sixth, despite expert harmonization, inter-survey discrepancies may persist. Seventh, our causal inference relies on the validity of the IV. Although the SPA has been widely used as an IV for retirement [4, 5], the assumption of exclusion restriction is not testable. The SPA makes individuals anticipate retirement and may affect their behaviors and mental health, such as starting exercise, undergoing preventive care, or experiencing financial stress. A study using data from the SHARE demonstrated that individuals planning to retire in the next two years had a reduced risk of depression compared with other workers [26]. If such changes in behaviors and mental health before anticipated retirement affect cognitive function, the exclusion restriction assumption can be violated. However, the overidentification test in our 2SLS estimation did not show evidence of its violation.
In conclusion, our findings demonstrate that retirement’s impact on cognitive function varies with individual characteristics and countries. This heterogeneity suggests policymakers should consider incorporating flexible early retirement options into pension systems, allowing individuals to make retirement decisions based on personal circumstances. A machine-learning-based prediction tool could enable individuals to determine optimal retirement timing by evaluating their specific characteristics.
Ethics approval
Our study used publicly available data that have obtained with informed consent from all participants and ethical approval from relevant local ethics committees. Thus, the Ethics Committee of Kyoto University exempted this study from review.
Supplementary Material
dyaf201_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Albert MS , De Kosky ST, Dickson D et al The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 2011;7:270–9.21514249 10.1016/j.jalz.2011.03.008PMC 3312027 · doi ↗ · pubmed ↗
- 2World Health Organization. Global Action Plan on the Public Health Response to Dementia 2017–2025. WHO, 2017.
- 3Grossman M. On the concept of health capital and the demand for health. J Polit Econ 1972;80:223–55.
- 4Garrouste C , Perdrix E. Is there a consensus on the health consequences of retirement? A literature review. J Econ Surv 2022;36:841–79.
- 5Nishimura Y , Oikawa M, Motegi H. What explains the difference in the effect of retirement on health? Evidence from global aging data. J Econ Surv 2018;32:792–847.
- 6Bonsang E , Adam S, Perelman S. Does retirement affect cognitive functioning? J Health Econ 2012;31:490–501.22538324 10.1016/j.jhealeco.2012.03.005 · doi ↗ · pubmed ↗
- 7Ebeid M , Oguzoglu U. Short-term effect of retirement on health: evidence from nonparametric fuzzy regression discontinuity design. Health Econ 2023;32:1323–43. 10.1002/hec.466936862580 · doi ↗ · pubmed ↗
- 8Coe NB , von Gaudecker H-M, Lindeboom M et al The effect of retirement on cognitive functioning. Health Econ 2012;21:913–27.21818822 10.1002/hec.1771 · doi ↗ · pubmed ↗