Trajectory of severe COVID anxiety and predictors for recovery in an 18-month UK cohort
Jacob D. King, Aisling McQuaid, Kirsten Barnicot, Paul Bassett, Verity C. Leeson, Martina Di Simplicio, Peter Tyrer, Helen Tyrer, Richard G. Watt, Mike J. Crawford

TL;DR
Severe COVID anxiety generally decreases over 18 months, but some people continue to experience high levels, especially those with depression, health anxiety, or from high-risk minority groups.
Contribution
Identifies long-term trajectory and predictors of recovery for severe COVID anxiety in a UK cohort.
Findings
Most participants experienced significant reductions in severe COVID anxiety over 18 months.
23.7% of participants continued to worry about COVID daily, and 13% had severe symptoms post-restrictions.
Older age, minority ethnic background, health anxiety, and depression predicted slower recovery.
Abstract
People with severe COVID anxiety have significant fears of contagion, physiological symptoms of anxiety in response to a COVID stimulus and employ often disproportionate safety behaviours at the expense of other life priorities. To characterise the long-term trajectory of severe COVID anxiety, and the factors that influence recovery. This prospective cohort study followed 285 people with severe COVID anxiety in the UK over 18 months. A nested randomised feasibility trial tested an online cognitive–behavioural therapy (CBT)-based intervention (no. ISRCTN14973494). Descriptive statistics and linear regression models identified factors associated with change in COVID anxiety over 18 months. Most participants experienced major reductions in COVID anxiety over time (69.8% relative cohort mean decrease, P < 0.001), but a quarter of people (23.7%, 95% CI: 17.8–30.1) continued to worry about…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
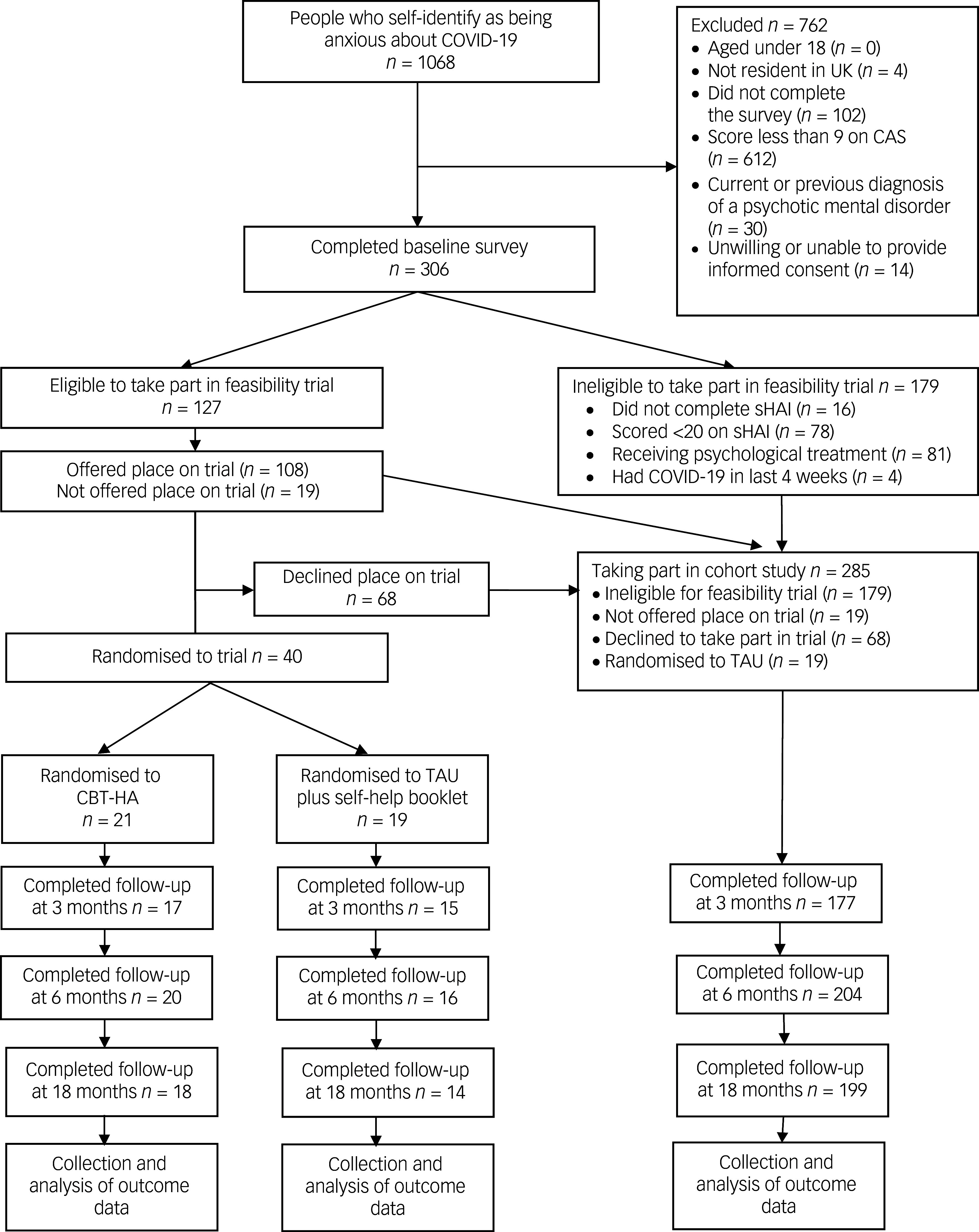 Figure 1
Figure 1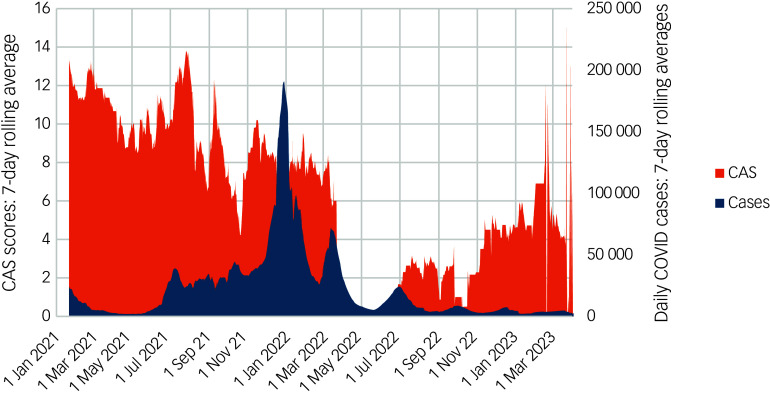 Figure 2
Figure 2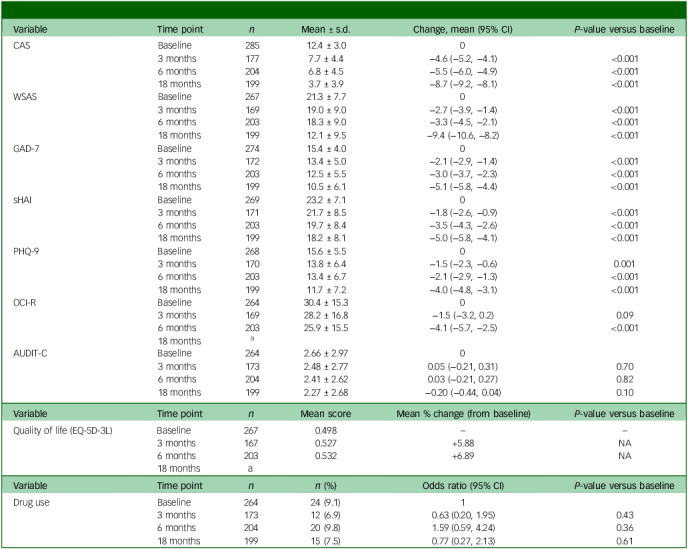 Figure 3
Figure 3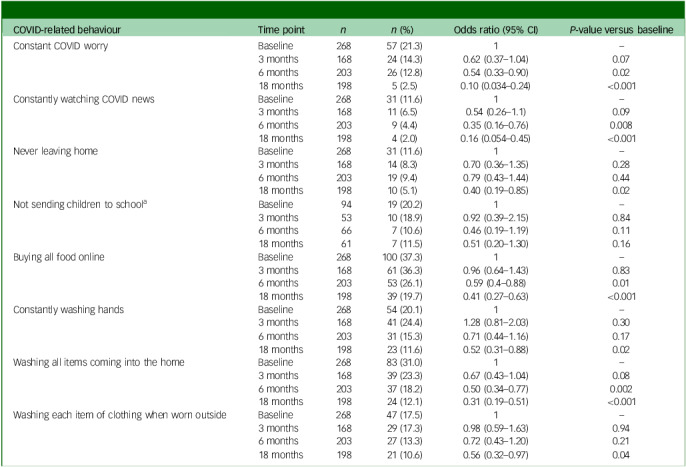 Figure 4
Figure 4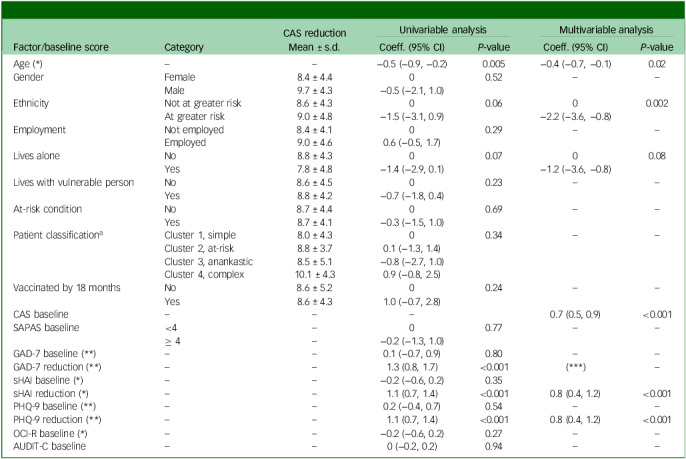 Figure 5
Figure 5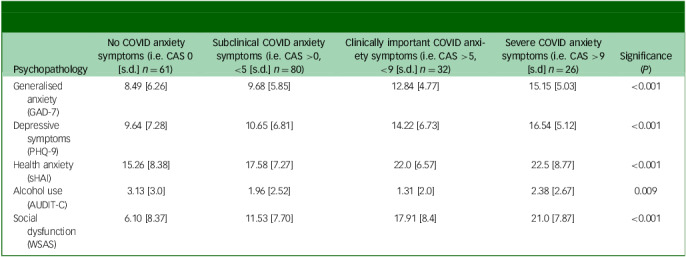 Figure 6
Figure 6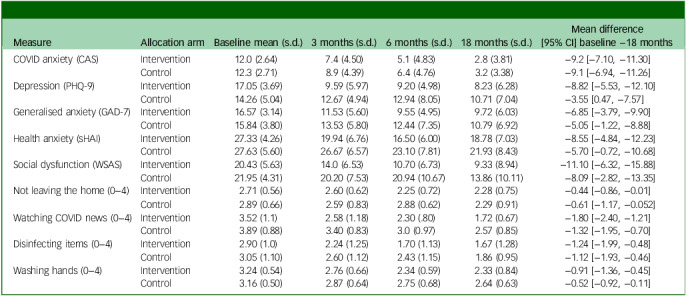 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and Mental Health · Long-Term Effects of COVID-19 · Anxiety, Depression, Psychometrics, Treatment, Cognitive Processes
Anxious thoughts and feelings about COVID-19 are common, and appropriate given the very real threats to health and well-being posed by the virus. Nonetheless, for around 5–15% of people at the height of the pandemic, fears of contagion and anticipation of adverse physical and socioeconomic consequences became overwhelming, leading to changes in behaviour that were no longer adaptive, and reinforced preoccupation with contagion.^ 1,2 ^ These included excessive hand-washing, disinfecting items brought into the home, great consumption of COVID-related news media, online symptom checking and not leaving the home to a degree disproportionate to public health guidance, which stopped people from being able to get on with other life priorities.^ 3,4 ^ Moreover, somatic symptoms of anxiety such as shortness of breath and gastrointestinal disturbance were sometimes misinterpreted as signs of COVID-19 itself, further reinforcing bodily vigilance and symptom-checking behaviours that perpetuated anxiety.^ 5,6 ^
Greater levels of COVID anxiety are associated with poorer levels of overall mental health, socio-occupational functioning and a lower quality of life, as well a greater rates of health anxiety, post-traumatic stress, obsessive–compulsive and depressive symptoms^ 3,7 ^ and substance misuse.^ 8 ^ In previous work among people with severe levels of COVID anxiety, high levels of co-occurring psychopathology were the norm, and few people scored low on assessment tools measuring depressive, obsessive–compulsive symptoms or generalised anxiety and health anxiety.^ 3,9 ^
Put simply, COVID anxiety is best formulated as a specific anxiety syndrome response to COVID-19 stimuli.^ 10 ^ It appears to be a heterogenous experience, insofar as there have emerged different underlying psychological processes at play, including variable stimulus hypervigilance and avoidance responses, worrying and checking cycles, differential conditioning and fear generalisation, and post-traumatic-like responses. Indeed COVID anxiety has been formulated variably by different research groups, and probably represents a variety of anxiety processes different for different people: a specific phobia of the coronavirus, a stimulus within generalised or health anxiety or obsessive–compulsive processes, as the trigger for post-traumatic phenomena, or indeed a social stressor that some people with low coping skills, intolerance of uncertainty and high-trait neuroticism are unable to manage. Moreover, specific clinical clusters of severe COVID anxiety have emerged, associated with patterns of associated health behaviours, health conditions that increase risk from COVID-19, symptoms of other mental health disorders and demographic profiles.^ 11 ^ Nevertheless, whatever the clinical formulation, given the levels of distress and dysfunction, there is a case to be made that people with severe COVID anxiety might benefit from targeted mental health support.
There has now been much written on the changes in population general mental health, before, during and following the coronavirus pandemic, with near global consistence in patterns of clinically significant increases in population levels of psychological distress and specific anxiety disorders which, having peaked in the early stages of the pandemic, followed a gradual return to near pre-pandemic levels.^ 12 ^ However, specific groups of people appear to experience much slower improvements in their mental health, most notably adolescents and young people,^ 13 ^ and also individuals who had existing poor mental health states prior to the pandemic.^ 14 ^ Given that COVID anxiety is a response to a specific stimulus, it is unclear whether the trajectory of this phenomenon would follow a similar path over the pandemic as case numbers rose and fell as, for example, measures of depression or generalised anxiety do, or indeed whether similar factors influence the trajectory.
A handful of longitudinal studies reporting the level of COVID anxiety (and comparable concepts including coronaphobia, COVID stress disorder/syndrome, COVID-19 fear, COVID-related worries or COVID-19 anxiety syndrome) in the same people over time have been published.^ 15–18 ^ However, none have examined which factors are predictive of a change in symptoms, nor do these studies consider specifically people with the most severe and clinically important levels of COVID anxiety. These studies ranged in their follow-up periods from between 5 and 16 months and cover a time period from February 2020 until October 2021 in Brazil, China, the Netherlands, UK and USA. Three studies assessed symptoms at more than two time points. Although all studies demonstrated meaningful reductions in the level of COVID anxiety over time, there do not appear to be studies that have assessed levels of COVID anxiety at a time after the coronavirus became endemic, when there were no longer public health restrictions in place and cases were not routinely monitored. Moreover, since the latest follow-up time point of these longitudinal studies there has been much greater uptake of vaccination, the development and availability of effective treatments and declining mortality rates, all factors likely to be associated with reducing levels of COVID anxiety.
In response to COVID anxiety, there have been a handful of interventions tested, most commonly based on cognitive–behavioural therapy (CBT),^ 19–21 ^ each showing some benefit to measures of COVID anxiety against control conditions but with very short follow-up periods – usually a matter of a few weeks. Assessing such interventions with longer-term follow-up may help inform the design and implementation of targeted pandemic mental health care in the future.
In short, the natural course of severe COVID anxiety over longer follow-up periods is unclear, as are the factors that might be associated with improvement or persistence of these symptoms over time and post-pandemic. In this study we therefore report on 18-month outcome data from a cohort of people sampled from the general UK population with severe levels of COVID anxiety, covering a period when COVID had become endemic, and examine the effect of a range of demographic and clinical factors, as well as a small trial intervention, on its trajectory.
Method
The ‘COVID Anxiety Project’ is an 18-month prospective cohort study, with a nested randomised feasibility trial of an online CBT-based intervention targeting health anxiety for a small subsample.
The project recruited adults from the UK with severe COVID anxiety during the British second and third waves (January–September 2021). This was a time more than a year after the first UK cases were identified, during which the third national lockdown had ended and social distancing restrictions were eased, vaccination was increasingly available but case rates remained high. This time period was selected in order to identify people for whom COVID anxiety symptoms were most likely to be persistent and not largely attributable to an initial, adaptive, ‘uncertainty effect’. For most of the population, uncertainty about the potential social and health impacts in the early pandemic stages was understandably worrying, but most people were able to adapt after some months, seeing major improvements in distress when the risks and solutions became more clear.^ 12 ^
Participants were followed up 3, 6 and 18 months after recruitment, with the last follow-up completed in April 2023 when there was no longer national tracking of case rates and no public health restrictions in place.
Analyses of 6-month outcome data from this cohort have previously been published, which demonstrated meaningful declines in the level of COVID anxiety of participants, albeit most continued to experience clinically important levels.^ 9 ^ While there were high rates of co-occurring mental health symptoms in this sample, there were notable decreases in almost all psychopathology measures. People who continued to report high levels of health anxiety and depressive symptoms were less likely to have experienced meaningful reductions in their levels of COVID anxiety in multivariate models. Participants received a £10 e-voucher for completion of the baseline survey and a £20 e-voucher for completion of the surveys at 6- and 18-month follow-ups.
Participants
A total of 1068 individuals who self-identified as being anxious about COVID initially responded to advertisements on social media platforms, and from text message contact made by 19 affiliated general practice (family medicine) clinics in London.^ 22 ^
Of that total, 306 people (30.4%) scored 9 or more on the 20-point COVID Anxiety Scale (CAS)^ 23 ^ indicating severe COVID anxiety, provided written consent and met other eligibility criteria, including not having a history of psychotic illness nor having had COVID-19 infection in the preceding 4 weeks.^ 22 ^ People who additionally scored >20 on the short Health Anxiety Inventory (indicating clinically significant health anxiety symptoms), and who were not currently receiving psychological treatment, were invited to participate in a nested randomised feasibility trial of CBT for Health Anxiety (CBT-HA). The cohort recruited participants until there were sufficient numbers meeting these further inclusion criteria to power the nested randomised feasibility trial.^ 9 ^ Randomisation of 40 participants at a ratio of 1:1 would be sufficient to detect a 50% uptake of CBT-HA with 95% confidence intervals of ±15%.
This sample was predominantly female (81.2%), with a median average age of 41 years (interquartile range (IQR) 28–53, range 18–83). Compared with the UK general population there was a similar median age, although the age distribution of this sample of people with severe COVID anxiety was positively skewed: while 20% of the sample was aged between 18 and 25 years, 13.9% was over 60. Of those reporting their ethnicity, 29.8% came from an ethnic minority group, about half of whom were of an ethnic group with greater risk to heath from COVID-19. This included people from a Black African, Black Caribbean and South Asian background. There were significant rates of mental health conditions in this cohort, and otherwise nationally representative rates of at-risk health conditions. A full description of baseline cohort characteristics has been reported previously.^ 3 ^ Latent profile analysis conducted on baseline data from this cohort identified four clinically distinct clusters of people with severe COVID anxiety.^ 11 ^ Clusters with significantly lower and higher burdens of co-occurring mental health symptoms emerged, along with a cluster of individuals with greater than expected rates of at-risk health conditions who were older than cohort average and abstinent of alcohol, and a fourth with prominent obsessive–compulsive symptoms and personality pathology described as ‘anankastic’ (Fig. 1).
Fig. 1. Flow diagram of trial procedure. CAS, COVID Anxiety Scale; CBT-HA, cognitive–behavioural therapy for health anxiety; sHAI, Short Health Anxiety Inventory; TAU, treatment as usual.
Measures
Our primary outcome was the level of COVID anxiety as measured using the self-report 5-item COVID Anxiety Scale, which was the first, and at the time only, validated assessment scale. This scale assesses the frequency of five somatic symptoms (loss of appetite, gastrointestinal disturbance, poor sleep, dizziness and feeling paralysed or frozen) experienced in response to COVID,^ 24 ^ such as watching or reading news about the pandemic. A score of 5 or more indicates the probable presence of levels of COVID anxiety associated with significant disruption to daily life, and a score of 9 or more indicates a severe degree of symptomatology.^ 25 ^ At baseline, self-completed questionnaires were used to assess for symptoms of generalised anxiety, depression, health anxiety, obsessive–compulsive symptomatology, personality disorder and drug and alcohol use. Respectively, these were the Generalised Anxiety Disorder scale – 7 items (GAD-7), the Patient Health Questionnaire – 9 items (PHQ-9), the 14 health anxiety items of the Short form Health Anxiety Inventory (sHAI), the Obsessive–Compulsive Inventory – Revised (OCI-R), the Standardised Assessment of Personality Abbreviated Scale (SAPAS), drug use with the Single Drug Use Item (SDUI) and the Alcohol Use Disorders Identification Test for Consumption (AUDIT-C). At baseline none of the assessment scales were meaningfully correlated in this cohort (r > 0.6), and other characteristics of these data are presented in the baseline paper.^ 3 ^
Additionally we collected a measure of social and occupational functioning (Work and Social Adjustment Scale, WSAS), as well as novel measures of COVID-specific health behaviours including hand-washing, staying at home, disinfecting items brought in to the home and consuming media relating to COVID-19, which were developed in association with people with lived experience of poor mental health during the pandemic.^ 3 ^ Questions assessing these behaviours were constructed on 4-point Likert-item scales ranging from 0 (behaviour not used; for example, washing hands to the same degree as before the pandemic) to 4 (dysfunctional form of the behaviour employed; for example, constantly washing one’s hands). In this study we report COVID-associated behaviours in two ways: as the proportion of people employing the dysfunctional form of the behaviour, and also as a mean cohort average score.
Demographic factors were collected including age, gender, ethnicity, employment and relationship status and household composition, as well as self-disclosed physical health conditions, which were coded using MedDRA criteria (https://www.meddra.org/) by a physician. Health conditions and participants’ ethnic background were assessed as increasing an individual’s risk to COVID-19 with the QCOVID tool (https://qcovid.org/). Twenty-one participants were excluded from these cohort analyses because they were randomised to the active arm of the feasibility trial for CBT-HA, which we anticipated would influence the natural trajectory of severe COVID anxiety, and were therefore analysed separately.^ 22 ^
At the 18-month follow-up we collected repeat measures for COVID anxiety, generalised and health anxiety, depression, drug and alcohol use and social-occupational dysfunction. All data were collected using the Qualtrics platform (Qualtrics LLC, Seattle, WA, USA; https://www.qualtrics.com/en-gb/).
Serious adverse events (SAEs), which included death, hospitalisation and life-threatening events, were collected at baseline and each of the follow-up periods. Therapists were also reminded to report SAEs that occurred during treatment.
Randomisation and trial methods
Forty participants who additionally scored over 20 on the HAI (indicating clinically significant health anxiety symptoms), and who were not already engaging in a psychological intervention, were randomised 1:1 in the feasibility trial by the ‘sealed envelope’ method. Both of these arms could continue to access treatment as usual (TAU), including having access to mental health support from primary or secondary care services. Participants were also given a short information guide on maintaining good mental health during the pandemic, developed by psychologists from Central and North West London NHS Foundation Trust. The trial was registered prospectively (https://www.isrctn.com/ISRCTN14973494). Twenty-one participants were randomised to the active arm, and 19 to TAU.
Intervention
Those 21 individuals in the active arm were offered up to 10 sessions of CBT targeting COVID health anxiety based on a published treatment manual.^ 26 ^ This was delivered remotely using a secure web-based telecoms platform. Session content included collaborative CBT formulation about COVID anxiety-specific thoughts and behaviours, symptom diary keeping, techniques to manage distress and reduce reinforcing behaviours and graded exposure techniques, among others. All therapists had a degree in a health-related subject, as well as past experience of delivering psychological interventions; they received a 90 min training session in CBT-HA from H.T., an expert in the treatment of health anxiety, and were required to attend fortnightly clinical supervision with her. A full description of the intervention has been reported in the trial protocol.^ 22 ^ Active arm participants received all assigned intervention sessions before the 6-month follow-up mark.
Data analysis
We published a statistical analysis plan in the ISRCTN registry prior to analysis (no. ISRCTN14973494). There were no within-scale missing data because the data collection platform that we used required that participants complete all items before they could progress through the survey.
We used descriptive statistics and linear regression models to assess the change in CAS scores from baseline to the 18-month follow-up. Univariate analysis first examined the unadjusted associations between change in CAS score and demographic factors, and also clinical factors both as baseline predictors and reductions in scores in the clinical measures between baseline and the 18-month time point. We used a backwards selection procedure in multivariate analysis, looking at the joint association of only those factors found to be associated with the outcome in univariate analysis (P < 0.2). The scores of feasibility trial participants were reported descriptively, and paired t-tests were used to assess the significance between baseline scores and the 18-month follow-up time point.
We also conducted ad hoc off-protocol analyses to examine the association of national daily COVID-19 cases and COVID-19-associated hospitalisations with the severity of COVID anxiety in our cohort during the study period. Seven-day rolling averages of the number of COVID-19 cases reported, and COVID-19-associated hospital admissions in England and Wales (representing 90% of UK population), were taken from publicly available UK government data (https://ukhsa-dashboard.data.gov.uk/). Scotland and Northern Ireland had stopped daily reporting of figures in May 2022. We aligned, by date, 865 unpaired CAS data points from our study to the 7-day rolling average COVID-19 cases and hospitalisations between January 2021 and April 2023. We used univariate analyses to assess the unadjusted association between these rates and CAS scores, and multivariate analysis to assess the mediating effect of other factors.
All data were managed and analysed in SPSS version 20.0 (SPSS Inc., Chicago, IL, USA; https://www.ibm.com/products/spss) and Stata version 16.1 (StataCorp LLC, College Station, TX, USA; https://www.stata.com/products/).
Ethical approval
This study was approved by the Leicester Central Research Ethics Committee and Health Regulation Authority in 2020 (reference no. 20/EM/023). The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation, and with the Helsinki Declaration of 1975 as revised in 2013. Following recruitment, all individuals were required to read and sign a consent form before participation, and received a copy.
Results
Of 285 participants, 177 (61.2%) provided responses at 3-month follow-up, 204 (71.2%) at 6 months and 199 (69.8%) at 18 months. Men (P = 0.008), people of a Black, South Asian or mixed ethnic heritage (P = 0.03), people with baseline scores indicating lower levels of personality pathology (P = 0.03) and those in the subgroup without high rates of co-occurring psychopathology (P = 0.03) were less likely to have completed follow-up at 18 months.
Cohort mean average CAS scores dropped from 12.4 (95% CI: 12.1−12.7) to 7.7 (95% CI: 7.1−8.4) at 3 months, to 6.8 (95% CI: 6.2−7.4) at 6 months and to 3.7 (95% CI: 3.2−4.2) at 18 months (69.8% relative decrease, P < 0.001); 13.1% (n = 26) of the cohort continued to score over 9 (indicating severe COVID anxiety) at 18 months, and 38.2% (n = 76) continued to score 5 or more indicating levels of COVID anxiety associated with an impact on daily life. Sixty-one (31%) people scored 0 at 18 months, indicating resolution of COVID anxiety symptoms.
The cohort demonstrated major reductions in mean generalised anxiety (−31.7%, P < 0.001), depressive symptoms (−24.5%, P < 0.001), health anxiety (−23.9%, P < 0.001) and social and occupational dysfunction (−43.0%, P < 0.001) over the 18 months (Table 1).
Table 1. Changes in key parameters over timeVariableTime point n Mean ± s.d.Change, mean (95% CI) P-value versus baselineCASBaseline28512.4 ± 3.003 months1777.7 ± 4.4−4.6 (−5.2, −4.1)<0.0016 months2046.8 ± 4.5−5.5 (−6.0, −4.9)<0.00118 months1993.7 ± 3.9−8.7 (−9.2, −8.1)<0.001WSASBaseline26721.3 ± 7.703 months16919.0 ± 9.0−2.7 (−3.9, −1.4)<0.0016 months20318.3 ± 9.0−3.3 (−4.5, −2.1)<0.00118 months19912.1 ± 9.5−9.4 (−10.6, −8.2)<0.001GAD-7Baseline27415.4 ± 4.003 months17213.4 ± 5.0−2.1 (−2.9, −1.4)<0.0016 months20312.5 ± 5.5−3.0 (−3.7, −2.3)<0.00118 months19910.5 ± 6.1−5.1 (−5.8, −4.4)<0.001sHAIBaseline26923.2 ± 7.103 months17121.7 ± 8.5−1.8 (−2.6, −0.9)<0.0016 months20319.7 ± 8.4−3.5 (−4.3, −2.6)<0.00118 months19918.2 ± 8.1−5.0 (−5.8, −4.1)<0.001PHQ-9Baseline26815.6 ± 5.503 months17013.8 ± 6.4−1.5 (−2.3, −0.6)0.0016 months20313.4 ± 6.7−2.1 (−2.9, −1.3)<0.00118 months19911.7 ± 7.2−4.0 (−4.8, −3.1)<0.001OCI-RBaseline26430.4 ± 15.303 months16928.2 ± 16.8−1.5 (−3.2, 0.2)0.096 months20325.9 ± 15.5−4.1 (−5.7, −2.5)<0.00118 months^ a^ AUDIT-CBaseline2642.66 ± 2.9703 months1732.48 ± 2.770.05 (−0.21, 0.31)0.706 months2042.41 ± 2.620.03 (−0.21, 0.27)0.8218 months1992.27 ± 2.68−0.20 (−0.44, 0.04)0.10VariableTime point n Mean scoreMean % change (from baseline) P-value versus baselineQuality of life (EQ-5D-3L)Baseline2670.498––3 months1670.527+5.88NA6 months2030.532+6.89NA18 monthsaVariableTime point n
n (%)Odds ratio (95% CI) P-value versus baselineDrug useBaseline26424 (9.1)13 months17312 (6.9)0.63 (0.20, 1.95)0.436 months20420 (9.8)1.59 (0.59, 4.24)0.3618 months19915 (7.5)0.77 (0.27, 2.13)0.61CAS, COVID Anxiety Scale; GAD-7, General Anxiety Disorder Assessment 7-item; PHQ-9, Patient Health Questionnaire 9-item; OCI-R, Obsessive–Compulsive Inventory Revised; sHAI, Health Anxiety Inventory Short Form; AUDIT-C, Alcohol Use Disorders Identification Test of Consumption; WSAS, Work and Social Adjustment Scale; EQ-5D-3L, EuroQol 5-Dimension 5-Level measure of health-related quality of life; NA, not applicable.a. Data not collected.
At the 18-month follow-up, almost half of the sample reported still washing their hands much more than before the start of the pandemic (47.9%, 95% CI: 40.6−55.3%), 1 in 5 continued to disinfect most items coming into their home (21.6%, 95% CI: 16.0−28.1%), another 1 in 5 reported watching COVID-related news media at least daily (22.1%, 95% CI: 16.4−28.7%) and almost a quarter (23.7%, 95% CI: 17.8−30.1) reported that they still worried about COVID every day. Of those participants with school-age children, 11.2% (n = 7) continued not to send their children to school even though they were expected to, because of concerns about COVID contagion. By the 18-month follow-up, 124 (62.9%) participants reported having been infected by the coronavirus and 9 (4.6%) reported having been hospitalised by it; 175 (88.8%) reported receiving at least one COVID vaccine (Table 2).
Table 2. Changes in COVID-related thoughts and behaviours over timeCOVID-related behaviourTime point n
n (%)Odds ratio (95% CI) P-value versus baselineConstant COVID worryBaseline26857 (21.3)1–3 months16824 (14.3)0.62 (0.37–1.04)0.076 months20326 (12.8)0.54 (0.33–0.90)0.0218 months1985 (2.5)0.10 (0.034–0.24)<0.001Constantly watching COVID newsBaseline26831 (11.6)1–3 months16811 (6.5)0.54 (0.26–1.1)0.096 months2039 (4.4)0.35 (0.16–0.76)0.00818 months1984 (2.0)0.16 (0.054–0.45)<0.001Never leaving homeBaseline26831 (11.6)1–3 months16814 (8.3)0.70 (0.36–1.35)0.286 months20319 (9.4)0.79 (0.43–1.44)0.4418 months19810 (5.1)0.40 (0.19–0.85)0.02Not sending children to school^ a ^ Baseline9419 (20.2)1–3 months5310 (18.9)0.92 (0.39–2.15)0.846 months667 (10.6)0.46 (0.19–1.19)0.1118 months617 (11.5)0.51 (0.20–1.30)0.16Buying all food onlineBaseline268100 (37.3)1–3 months16861 (36.3)0.96 (0.64–1.43)0.836 months20353 (26.1)0.59 (0.4–0.88)0.0118 months19839 (19.7)0.41 (0.27–0.63)<0.001Constantly washing handsBaseline26854 (20.1)1–3 months16841 (24.4)1.28 (0.81–2.03)0.306 months20331 (15.3)0.71 (0.44–1.16)0.1718 months19823 (11.6)0.52 (0.31–0.88)0.02Washing all items coming into the homeBaseline26883 (31.0)1–3 months16839 (23.3)0.67 (0.43–1.04)0.086 months20337 (18.2)0.50 (0.34–0.77)0.00218 months19824 (12.1)0.31 (0.19–0.51)<0.001Washing each item of clothing when worn outsideBaseline26847 (17.5)1–3 months16829 (17.3)0.98 (0.59–1.63)0.946 months20327 (13.3)0.72 (0.43–1.20)0.2118 months19821 (10.6)0.56 (0.32–0.97)0.04a. Of those respondents with school-aged children.
When adjusted for baseline CAS score, increasing age was the only demographic factor that remained significant (P = 0.005), at an alpha level of 0.05 in univariate analysis, as being predictive of slower improvements in COVID anxiety symptoms over time. While baseline levels of generalised anxiety, depression, personality pathology, obsessive–compulsive symptoms and alcohol use were also not predictive of a differing trajectory, improvements in generalised anxiety, health anxiety and depression over time were favourably and significantly associated with a CAS reduction. Other variables, including living with an at-risk health condition or living with someone vulnerable to COVID-19, were not associated with smaller reductions in COVID anxiety over time. There was no predictive effect of subgroup cluster on the magnitude of CAS reduction, nor was there an effect of vaccination status or having contracted COVID-19.
In multivariate modelling, age and coming from a Black, South Asian or mixed ethnic background were significant predictors of lesser reductions in CAS, compared with people from ethic backgrounds without an increased risk (White British/other and East Asian). Every 10-year increment increase in age was associated with a 0.4-point smaller reduction in CAS score over 18 months. Furthermore, individuals for whom depressive and health anxiety symptoms reduced more over the follow-up period also had significantly greater reductions in their COVID anxiety (Table 3).
Table 3. Associations between demographic and clinical factors, and reduction in CAS scores from baseline to 18-month follow-upFactor/baseline scoreCategoryCAS reductionUnivariable analysisMultivariable analysisMean ± s.d.Coeff. (95% CI) P-valueCoeff. (95% CI) P-valueAge ()––−0.5 (−0.9, −0.2)0.005−0.4 (−0.7, −0.1)0.02GenderFemale8.4 ± 4.400.52––Male9.7 ± 4.3−0.5 (−2.1, 1.0)EthnicityNot at greater risk8.6 ± 4.300.0600.002At greater risk9.0 ± 4.8−1.5 (−3.1, 0.9)−2.2 (−3.6, −0.8)EmploymentNot employed8.4 ± 4.100.29––Employed9.0 ± 4.60.6 (−0.5, 1.7)Lives aloneNo8.8 ± 4.300.0700.08Yes7.8 ± 4.8−1.4 (−2.9, 0.1)−1.2 (−3.6, −0.8)Lives with vulnerable personNo8.6 ± 4.500.23––Yes8.8 ± 4.2−0.7 (−1.8, 0.4)At-risk conditionNo8.7 ± 4.400.69––Yes8.7 ± 4.1−0.3 (−1.5, 1.0)Patient classification^ a ^ Cluster 1, simple8.0 ± 4.300.34––Cluster 2, at-risk8.8 ± 3.70.1 (−1.3, 1.4)Cluster 3, anankastic8.5 ± 5.1−0.8 (−2.7, 1.0)Cluster 4, complex10.1 ± 4.30.9 (−0.8, 2.5)Vaccinated by 18 monthsNo8.6 ± 5.200.24––Yes8.6 ± 4.31.0 (−0.7, 2.8)CAS baseline–––0.7 (0.5, 0.9)<0.001SAPAS baseline<4–00.77––≥ 4–−0.2 (−1.3, 1.0)GAD-7 baseline ()––0.1 (−0.7, 0.9)0.80––GAD-7 reduction ()––1.3 (0.8, 1.7)<0.001()–sHAI baseline ()––−0.2 (−0.6, 0.2)0.35sHAI reduction ()––1.1 (0.7, 1.4)<0.0010.8 (0.4, 1.2)<0.001PHQ-9 baseline ()––0.2 (−0.4, 0.7)0.54––PHQ-9 reduction ()––1.1 (0.7, 1.4)<0.0010.8 (0.4, 1.2)<0.001OCI-R baseline ()––−0.2 (−0.6, 0.2)0.27––AUDIT-C baseline––0 (−0.2, 0.2)0.94––CAS, COVID Anxiety Scale; GAD-7, General Anxiety Disorder Assessment 7-item; PHQ-9, Patient Health Questionnaire 9-item; OCI-R, Obsessive–Compulsive Inventory Revised; sHAI, Health Anxiety Inventory Short Form; AUDIT-C, Alcohol Use Disorders Identification Test of Consumption; SAPAS, Standardised Assessment of Personality Abbreviated Scale. Univariate analyses adjust for baseline CAS score.aClusters were established using latent profile analysis.^ 3 ^ () Regression coefficients reported for a 10-unit change in variable.() Regression coefficients reported for a 5-unit change in variable.(***) GAD-7 reductions were no longer associated with reducing CAS scores in multivariable analysis, and were thus not included in the final model.
Those 61 people who no longer reported symptoms of COVID anxiety also scored lower than individuals who continued to experience symptoms of COVID anxiety on their measures of generalised and health anxiety, depressive symptoms and social dysfunction. There was a gradient between the level of severity of COVID anxiety and co-occurring mental health symptoms (Table 4).
Table 4. Comparisons of co-occurring psychopathology scores by severity level of COVID anxiety at 18 months, using analysis of variance significance testingPsychopathologyNo COVID anxiety symptoms (i.e. CAS 0 [s.d.] n = 61)Subclinical COVID anxiety symptoms (i.e. CAS >0, <5 [s.d.] n = 80)Clinically important COVID anxiety symptoms (i.e. CAS >5, <9 [s.d.] n = 32)Severe COVID anxiety symptoms (i.e. CAS >9 [s.d] n = 26)Significance (P)Generalised anxiety (GAD-7)8.49 [6.26]9.68 [5.85]12.84 [4.77]15.15 [5.03]<0.001Depressive symptoms (PHQ-9)9.64 [7.28]10.65 [6.81]14.22 [6.73]16.54 [5.12]<0.001Health anxiety (sHAI)15.26 [8.38]17.58 [7.27]22.0 [6.57]22.5 [8.77]<0.001Alcohol use (AUDIT-C)3.13 [3.0]1.96 [2.52]1.31 [2.0]2.38 [2.67]0.009Social dysfunction (WSAS)6.10 [8.37]11.53 [7.70]17.91 [8.4]21.0 [7.87]<0.001CAS, COVID Anxiety Scale; GAD-7, GAD-7, General Anxiety Disorder Assessment 7-item; PHQ-9, Patient Health Questionnaire 9-item; sHAI, Short Health Anxiety Inventory; AUDIT-C, Alcohol Use Disorders Identification test for Consumption; WSAS, Work and Social Adjustment Scale.
Of 21 people allocated to the CBT-HA treatment arm, 18 (85.7%) provided follow-up responses at the 18-month time point, as did 14 of 19 (73.7%) randomised to the control arm. This feasibility trial was not designed to be powered to detect a difference between groups in outcome measures, because we assessed changes between baseline and 18-month follow-up scores within groups. Akin to the cohort at large, we observed reductions in all measures of poor mental health at 3 and 6 months sustained at 18 months from baseline. In the active arm, 5 of 18 (27.8%) participants continued to report symptoms of COVID anxiety consistent with an impact on daily life (CAS score >5) 18 months later, compared with 5 of 14 (35.7%) in the control arm. There were significant decreases in co-occurring measures of social dysfunction and generalised and health anxiety symptoms in both groups, but significant improvements in depression scale scores in the intervention arm only. For both groups there were significant reductions in the intensity of hand-washing, disinfecting items and COVID media consumption. There were no SAEs recorded from either group (Table 5).
Table 5. Outcomes and safety behaviours by intervention armMeasureAllocation armBaseline mean (s.d.)3 months (s.d.)6 months (s.d.)18 months (s.d.)Mean difference[95% CI] baseline −18 monthsCOVID anxiety (CAS)Intervention12.0 (2.64)7.4 (4.50)5.1 (4.83)2.8 (3.81)−9.2 [−7.10, −11.30]Control12.3 (2.71)8.9 (4.39)6.4 (4.76)3.2 (3.38)−9.1 [−6.94, −11.26]Depression (PHQ-9)Intervention17.05 (3.69)9.59 (5.97)9.20 (4.98)8.23 (6.28)−8.82 [−5.53, −12.10]Control14.26 (5.04)12.67 (4.94)12.94 (8.05)10.71 (7.04)−3.55 [0.47, −7.57]Generalised anxiety (GAD-7)Intervention16.57 (3.14)11.53 (5.60)9.55 (4.95)9.72 (6.03)−6.85 [−3.79, −9.90]Control15.84 (3.80)13.53 (5.80)12.44 (7.35)10.79 (6.92)−5.05 [−1.22, −8.88]Health anxiety (sHAI)Intervention27.33 (4.26)19.94 (6.76)16.50 (6.00)18.78 (7.03)−8.55 [−4.84, −12.23]Control27.63 (5.60)26.67 (6.57)23.10 (7.81)21.93 (8.43)−5.70 [−0.72, −10.68]Social dysfunction (WSAS)Intervention20.43 (5.63)14.0 (6.53)10.70 (6.73)9.33 (8.94)−11.10 [−6.32, −15.88]Control21.95 (4.31)20.20 (7.53)20.94 (10.67)13.86 (10.11)−8.09 [−2.82, −13.35]Not leaving the home (0−4)Intervention2.71 (0.56)2.60 (0.62)2.25 (0.72)2.28 (0.75)−0.44 [−0.86, −0.01]Control2.89 (0.66)2.59 (0.83)2.88 (0.62)2.29 (0.91)−0.61 [−1.17, −0.052]Watching COVID news (0−4)Intervention3.52 (1.1)2.58 (1.18)2.30 (.80)1.72 (0.67)−1.80 [−2.40, −1.21]Control3.89 (0.88)3.40 (0.83)3.0 (0.97)2.57 (0.85)−1.32 [−1.95, −0.70]Disinfecting items (0−4)Intervention2.90 (1.0)2.24 (1.25)1.70 (1.13)1.67 (1.28)−1.24 [−1.99, −0.48]Control3.05 (1.10)2.60 (1.12)2.43 (1.15)1.86 (0.95)−1.12 [−1.93, −0.46]Washing hands (0−4)Intervention3.24 (0.54)2.76 (0.66)2.34 (0.59)2.33 (0.84)−0.91 [−1.36, −0.45]Control3.16 (0.50)2.87 (0.64)2.75 (0.68)2.64 (0.63)−0.52 [−0.92, −0.11]CAS, COVID Anxiety Scale; GAD-7, General Anxiety Disorder Assessment 7-item; PHQ-9, Patient Health Questionnaire 9-item; sHAI, Short Health Anxiety Inventory; AUDIT-C, Alcohol Use Disorders Identification test for Consumption; WSAS, Work and Social Adjustment Scale.
In ad hoc univariate analyses, the number of 7-day rolling COVID-19 cases (coefficient 0, P < 0.0001), but not hospitalisations, was positively associated with severity scores of COVID anxiety. For daily case rates, the addition of an ordinal time point variable (representing follow-up collection time point: 3, 6 or 18 months) to the model tempered the association of daily case rates with COVID anxiety severity to non-significance (coefficient 0, P = 0.41) (Fig. 2).
Fig. 2. All participant COVID Anxiety Scale (CAS) responses (n = 884) by date compared with 7-day rolling average daily cases. England and Wales case rates only, because Scotland and Northern Ireland stopped reporting daily cases in May 2022.
Discussion
This study has shown that, among a sample of people with severe COVID anxiety, there were meaningful improvements in COVID anxiety symptoms over time and, for around 1 in 3, a complete resolution 18 months later. There were corresponding declines in co-occurring mental health symptoms and in the unhelpful forms of COVID protective behaviours. However, for almost 4 in 10 there remained a degree of COVID anxiety that had an impact on daily life, and more than 1 in 10 continued to experience a severe degree of symptoms 18 months later. This was the situation, at a time more than 1 year after the ending of all social restrictions and public health enforcement in the UK.
COVID anxiety, mental health and daily functioning
Despite significant improvements in co-occurring mental health scores over time, this population’s 18-month PHQ-9 and GAD-7 mean scores were still more than double the nationally representative figures over this period.^ 27 ^ Indeed the 61 people in this cohort who no longer reported any symptoms of COVID anxiety also continued to report co-occurring mental health symptoms on average to a greater degree than the general population.^ 27 ^ This might suggest that people who at one time experienced severe levels of COVID anxiety may also be a population with longer-standing mental health difficulties, or who developed persistent mental health difficulties after their severe COVID anxiety improved. Despite much being written on COVID and mental health, there is little robust evidence to support either of these positions. Studies exploring the associations between COVID anxiety and symptoms of other mental health disorders appear to show a complex connection, probably bidirectional between COVID anxiety and other anxiety states.^ 10,28 ^ In some longitudinal studies, COVID-related fear at the beginning of the pandemic was predictive of subsequent poor mental health,^ 29 ^ but the evidence which established that mental health disorders were predictive of COVID anxiety is seemingly limited.^ 30 ^ There is much more evidence from these studies that existing mental health disorders predicted poorer mental health and stress during the pandemic, although this is rarely demonstrated specifically to be COVID anxiety.
The cohort average level of impairment in socio-occupational functioning (as reported by WSAS) also remained in the ‘moderate impairment’ range at 18 month follow-up, and of particular concern were the 11% of parents in this cohort who continued not to send their children to school, despite being required to do so, due to fears around COVID-19. In the UK, school attendance declined notably after the pandemic and has not yet returned to pre-pandemic levels.^ 31 ^ The present study provides some evidence therefore that, in a small number of cases, parental fear of COVID might continue partly to explain this phenomenon.
Predictors of the trajectory of severe COVID anxiety
This is the first study to have examined the trajectory and factors associated with changes in COVID anxiety over a long follow-up period among people with the most severe levels of COVID anxiety, and corroborates other studies’ findings that COVID-related anxiety improves progressively over time.^ 15–18 ^ Previous studies have identified a host of factors that appear to be associated with the severity of COVID anxiety during the pandemic, including older age, non-White ethnicity, personality traits, female gender and general levels of both physical and mental health.^ 15,16 ^ Our study builds on this by suggesting that increasing age and being from a heightened-risk ethnic minority background also appear to prolong the severity of COVID anxiety. It is possible that perceived risk accounts for these observations, but we note that other factors contributing to individuals’ objective COVID-19 risk profile, including having an at-risk health condition and vaccination status, do not appear to affect the trajectory of severe COVID anxiety in this study. Furthermore, the level of perceived threat in some studies has been shown to be associated with levels of COVID anxiety,^ 32 ^ and for some researchers it therefore stood to reason that greater numbers of reported daily cases, hospitalisations or deaths might create the impression of greater threat for some people, and therefore high COVID anxiety. Indeed, cross-sectional studies from a number of countries, including the UK, showed correlation between daily COVID cases and levels of depressive, generalised anxiety and trauma-related symptoms.^ 33 ^ Contrary to this trend, we did not identify an association between 7-day rolling COVID-19 cases or hospitalisations and COVID anxiety in the UK. This complements the one other longitudinal study examining the association of COVID-19-associated daily death rate and COVID anxiety, where there was no association observed.^ 18 ^
We previously conducted analysis on this same cohort at the 6-month time point,^ 9 ^ which identified that older age, higher baseline levels of generalised and health anxiety and greater reductions in health anxiety and depressive symptoms were significantly associated in multivariable models with greater reductions in COVID anxiety. These findings were again demonstrated 1 year later at the 18-month follow-up time point; however, the effect of baseline mental health scores no longer became predictive of the longer-term trajectory of severe COVID anxiety. Taken together, we suggest that older adults and people from minority ethnic backgrounds at heightened risk ought be accorded special consideration for any targeted support, given that these demographics appear to be associated with both increased severity of COVID anxiety and its persistence.
The effect of psychological interventions on the trajectory of severe COVID anxiety
There is some evidence from this cohort to signal that, in the long term, COVID anxiety reduces notably over time for most people irrespective of a CBT intervention (although co-occurring mental health measures and COVID-associated safety behaviours may change differentially). Other CBT interventions have demonstrated small but significant benefits towards COVID anxiety at short follow-up periods.^ 19,21 ^ We suspect that, in the long term, any potential benefit of a psychological intervention on levels of COVID anxiety may be overshadowed by the greater benefit of time. However, this does not mean that short-term improvements in COVID anxiety, or improvement in co-occurring psychopathology by other means, are not important exercises for reducing distress and improving the functioning and quality of life among people with severe pandemic anxiety.
Habituation, and implications for the treatment of severe COVID anxiety
Unlike other recent pandemics that have been studied for their effects on mental health and in formulating pandemic anxiety, principally H1N1 (swine flu), the SARS-CoV-2 coronavirus became endemic. The stimulus for COVID anxiety has not disappeared. Given the findings of this and other studies, that COVID anxiety appears to improve in time despite the maintained presence of stimuli, we agree with other authors that evidence supports a habituation process being at play for most people with COVID anxiety.^ 18 ^ Indeed, there is some evidence from care workers of reduced post-traumatic responses after repeated outbreaks,^ 34 ^ and in Germany COVID news consumption followed case rates in-step early in the pandemic but became increasingly disassociated as time went on, demonstrating, as those authors suggest, a habituation effect.^ 35 ^ In line with this, we have shown that symptoms of COVID anxiety and COVID-19-specific safety behaviours both steadily decline over time, despite variable rates of national COVID cases during this time.
A ‘regression to the mean’ explanation has been postulated by some authors to explain these repeated findings of improving mental health scores.^ 12 ^ Naturally we are unable to demonstrate a causal association as to whether reducing safety behaviours contributed to diminished COVID anxiety symptoms or vice versa. Nonetheless the process of habituation, towards response extinction, necessitates a reduction in safety behaviours^ 36 ^ and, notably with COVID anxiety, the behaviour of self-isolation, while potentially effective, when followed so strictly and out of keeping with public health guidance is a perpetuating factor of anxiety.^ 37 ^ There is evidence that lockdown periods were associated with greater levels of distress in part for this reason.^ 38 ^
Trial interventions supporting people with severe COVID anxiety have been attempted with a handful of psychological approaches, but many other therapeutic opportunities, such as improving a sense of being socially supported, went untested. Mechanistic therapeutic studies are lacking. Supporting the habituation to extinction process by improving distress tolerance,^ 39 ^ reducing propagative and ineffective safety behaviours and graded exposure out of self-isolation may therefore be appropriate targets in the treatment of pandemic anxiety.^ 32,37 ^
Given our findings that greater decreases in depressive and health anxiety symptoms were associated with greater declines in COVID anxiety, we might suggest that there is cause to believe that established mental health interventions proven to reduce these symptoms have a theoretical basis for also improving persistent COVID anxiety. In addition, of note reciprocally, randomised clinical trials of interventions specifically targeting COVID anxiety, particularly online CBT-based interventions,^ 9,19,21 ^ appear to improve other mental health outcomes too.
Limitations
This study is limited in several ways. First, given our recruitment procedure, the generalisability of the study may be limited: using mainly online and text message-based advertisements and an online platform may have posed a barrier to certain groups, perhaps older adults and those without access to the internet, in hearing of the study and engaging with it. Second, we could not account for changes in participants’ mental health prior to the start of the pandemic, nor the trajectory their mental health may have been on before recruitment. Third, some factors likely to partially explain our findings went uncollected. For example, we did not collect data on levels of social support and connectedness, which appeared to play a role in predicting the severity of COVID anxiety in other studies.^ 40 ^ Finally, while our nested trial was able to demonstrate the feasibility of the intervention, it was not powered ex ante to detect changes in clinical or behavioural outcomes.
Future directions
In conclusion, almost 40% of people with debilitating thoughts and feelings about COVID-19 in this sample during the British third wave of the pandemic continued to experience levels of COVID anxiety associated with social and occupational dysfunction 18 months later and, for 13%, this remained severe. Older adults and people from minority ethnic backgrounds that conferred greater risk from COVID-19 were significantly slower to recover, and ought to be considered for targeted support. Reducing co-occurring health anxiety and depressive symptoms with established interventions might be a target for supporting adults with pandemic-related anxiety in the future.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hajek A , König H-H. Prevalence and correlates of coronavirus anxiety in Germany: results of a nationally representative survey. Death Stud 2022; 47: 287–95.35412446 10.1080/07481187.2022.2059722 · doi ↗ · pubmed ↗
- 2Taylor S , Landry CA , Paluszek MM , Fergus TA , Mc Kay D , Asmundson GJG. COVID stress syndrome: concept, structure, and correlates. Depress Anxiety 2020; 37: 706–14.32627255 10.1002/da.23071 PMC 7362150 · doi ↗ · pubmed ↗
- 3King JD , Mc Quaid A , Leeson VC , Samuel O , Grant J , Imran Azeem MS , et al. The association of severe COVID anxiety with poor social functioning, quality of life, and protective behaviours among adults in United Kingdom: a cross-sectional study. BMC Psychiatry 2023; 23: 117.36810010 10.1186/s 12888-023-04595-1PMC 9943584 · doi ↗ · pubmed ↗
- 4Taylor S , Landry CA , Paluszek MM , Fergus TA , Mc Kay D , Asmundson GJG. Development and initial validation of the COVID Stress Scales. J Anxiety Disord 2020; 72: 102232.32408047 10.1016/j.janxdis.2020.102232 PMC 7198206 · doi ↗ · pubmed ↗
- 5Shevlin M , Nolan E , Owczarek M , Mc Bride O , Murphy J , Gibson Miller J , et al. COVID-19-related anxiety predicts somatic symptoms in the UK population. Br J Health Psychol 2020; 25: 875–82.32458550 10.1111/bjhp.12430 PMC 7283836 · doi ↗ · pubmed ↗
- 6Tyrer P. COVID-19 health anxiety. World Psychiatry 2020; 19: 307–8.32931105 10.1002/wps.20798 PMC 7491644 · doi ↗ · pubmed ↗
- 7Menzies RE , Menzies RG. Death anxiety in the time of COVID-19: theoretical explanations and clinical implications. Cogn Behav Therap 2020; 13: e 19.10.1017/S 1754470 X 20000215 PMC 730859634191938 · doi ↗ · pubmed ↗
- 8Taylor S , Paluszek MM , Rachor GS , Mc Kay D , Asmundson GJG. Substance use and abuse, COVID-19-related distress, and disregard for social distancing: a network analysis. Addict Behav 2021; 114: 106754.33310690 10.1016/j.addbeh.2020.106754 PMC 8164919 · doi ↗ · pubmed ↗