Iodine Deficiency-Induced Thyrotoxicosis Mimicking Graves’ Disease: A Case of Triiodothyronine (T3)-Predominant Hyperthyroidism Without Goiter
Pooja Alipuria, Atush Alipuria

TL;DR
A man with iodine deficiency developed hyperthyroidism symptoms similar to Graves’ disease but without a goiter, and recovered after switching to iodized salt.
Contribution
This case highlights iodine deficiency as a rare cause of T3-predominant thyrotoxicosis mimicking Graves’ disease.
Findings
The patient showed suppressed TSH, elevated free T3, and normal free T4 with no thyroid autoantibodies.
Switching to iodized salt and discontinuing medication led to sustained euthyroidism over 24 months.
Iodine deficiency-induced thyrotoxicosis can mimic autoimmune hyperthyroidism clinically.
Abstract
Triiodothyronine (T3)-predominant thyrotoxicosis without goiter is uncommon, with differential diagnoses including Graves’ disease, thyroiditis, and iodine deficiency-related autonomy. Diagnostic certainty can be challenging in resource-constrained settings. We describe a 41-year-old man who presented with palpitations, heat intolerance, and weight loss and reported exclusive use of non-iodized rock salt for three years. Examination revealed tachycardia and tremor without goiter or orbitopathy. Thyroid function tests showed suppressed thyroid-stimulating hormone, elevated free T3, normal free thyroxine, and negative thyroid autoantibodies. Ultrasound demonstrated a diffusely enlarged, non-nodular gland with normal echogenicity, while scintigraphy revealed diffuse homogeneous uptake. He was treated with carbimazole (20 mg/day, tapered to 5 mg) and propranolol (40 mg/day, later withdrawn)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
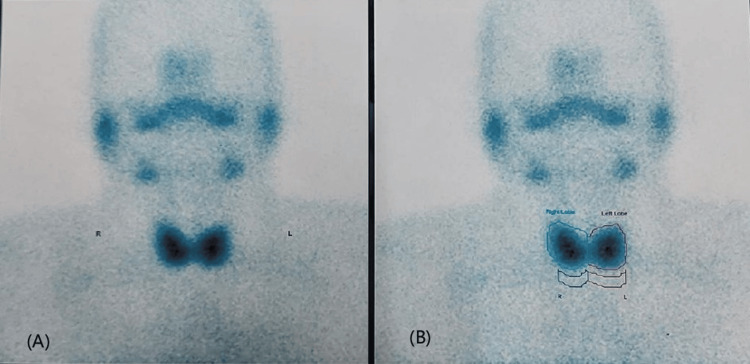 Figure 1
Figure 1| Parameter | On presentation | Repeated (to confirm) | On follow-up (after six weeks) | On follow-up (after three months) | On follow-up (after six months) | On follow-up (after one year) | On follow-up (after two years) |
| TSH (0.3-5.6 mIU/L) | <0.004 | 0.004 | 0.01 | 7.83 | 2.28 | 1.2 | 1.25 |
| FT3 (0.9-3.6 pg/mL) | 3.81 | 3.81 | 2.56 | 0.855 | 3.46 | 3.3 | - |
| FT4 (0.6-1.8 ng/dL) | 1.12 | 1.11 | 0.9 | 0.54 | 1.05 | 1.08 | 1.15 |
| TRAb (negative: <1.00 IU/L; equivocal: 1.10-1.50 IU/L; positive: >1.5 IU/L) | - | 0.91 | - | - | - | - | - |
| Anti-TPO antibodies (<5.61 IU/mL) | - | 3.41 | - | - | - | - | - |
| ESR (0-20 mm/hr) | - | 5 | - | - | - | - | - |
| Hemoglobin (13.0-17.0 g/dL) | - | 14.2 | - | 14.6 | - | - | 14.8 |
| TLC (4000-10,000 /cumm) | - | 5250 | - | 5540 | - | - | 4590 |
| Platelet (1.50-4.10 lakh/cumm) | - | 2.37 | - | 3.7 | - | - | 3.5 |
| Urea (16.60-48.50 mg/dL) | - | 23 | - | 25 | - | - | 22 |
| Creatinine (0.70-1.20 mg/dL) | - | 0.7 | - | 0.84 | - | - | 0.72 |
| Total bilirubin (0.2-1.2 mg/dL) | - | 0.3 | - | 0.5 | - | - | 0.4 |
| Direct bilirubin (<0.3 mg/dL) | - | 0.2 | - | 0.2 | - | - | 0.2 |
| AST (5-34 U/L) | - | 23 | -- | 25 | - | - | 23 |
| ALT (0-41 U/L) | - | 19 | - | 18 | - | - | 17 |
| Fasting blood sugar (<100 mg/dL) | - | 92 | - | - | - | - | 94 |
| Time (months) | Key events |
| -6 to 0 | Gradual onset of palpitations, heat intolerance, irritability, and ~5 kg weight loss. |
| 0 | Diagnosed with T3-predominant thyrotoxicosis (TRAb and anti-TPO negative). Started carbimazole 20 mg/day and propranolol 40 mg/day and advised to switch to iodized salt (~5 g/day). |
| 1.5 to 3 | Carbimazole tapered to 10 mg/day and then to 5 mg/day based on TFTs. Propranolol tapered with heart rate monitoring and discontinued once resting HR <90 bpm and symptoms resolved. |
| 3 to 9 | Maintained carbimazole 5 mg/day with good adherence. |
| 9 | Patient self-discontinued carbimazole after nine months of therapy. |
| 11 | Thyroid function normalized; patient euthyroid. |
| 11 to 33 | Sustained euthyroidism for 24 months on iodized salt alone. |
| Feature | Graves’ disease | Iodine deficiency autonomy | Thyroiditis |
| Orbitopathy | Often present | Absent | Absent |
| Autoantibodies | Frequently positive | Negative | Negative |
| Ultrasound | Diffuse enlargement with increased vascularity and hypoechogenicity | Diffuse enlargement, nodular or non-nodular, normal echogenicity | Diffusely hypoechoic with reduced vascularity |
| Scintigraphy | High diffuse uptake | Preserved diffuse uptake | Absent uptake |
| Urinary iodine | Normal | Low | Normal |
| Hormone pattern | T3- or mixed-predominant | T3-predominant | T4-predominant (higher T4/T3 ratio) |
| Course with antithyroid drugs | Relapse likely if stopped before 12-18 months | May remit with iodine repletion ± short course of antithyroid drugs | Self-limiting |
| Long-term outcome | Often requires radioiodine or surgery | May remain euthyroid | Spontaneous resolution |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Disorders and Treatments · Thyroid Cancer Diagnosis and Treatment · Ion channel regulation and function
Introduction
Iodine deficiency remains one of the most widespread nutritional disorders globally, affecting more than two billion people and contributing substantially to thyroid dysfunction [1]. In iodine-deficient states, thyroid hormone synthesis shifts toward triiodothyronine (T3), which requires fewer iodine atoms than thyroxine (T4) [2]. This physiological adaptation explains why chronic iodine deficiency may predispose individuals to T3-predominant thyrotoxicosis [2]. Prolonged deficiency can also lead to thyroid autonomy and toxic nodular goiter, particularly in older adults [3,4]. Even minor regional differences in iodine intake can significantly influence the prevalence and patterns of thyroid disorders [5].
Despite the implementation of universal salt iodization programs, mild iodine deficiency persists in some parts of India, especially in the Himalayan foothill states and regions of North and Northwest India, such as Uttarakhand, Himachal Pradesh, and Rajasthan, where non-iodized rock salt remains commonly used due to cultural and taste preferences [6]. In contrast, most coastal regions demonstrate near-adequate iodine sufficiency. In iodine-deficient areas, thyroid hyperfunction resulting from diffuse or nodular autonomy may present with biochemical and scintigraphic features that closely mimic autoimmune thyrotoxicosis, complicating diagnosis [7,8]. Graves’ disease, the most common cause of thyrotoxicosis worldwide, is characterized by autoimmune stimulation of thyrotropin (thyroid-stimulating hormone, TSH) receptors and is typically managed with antithyroid medications, radioiodine therapy, or surgery [9].
We report a case of T3-predominant thyrotoxicosis without goiter in a middle-aged man who had exclusively used non-iodized rock salt for several years. Sustained remission following iodine repletion and early discontinuation of antithyroid therapy supports iodine deficiency-induced thyrotoxicosis as the most likely etiology.
Case presentation
A 41-year-old vegetarian male with a sedentary occupation from North India presented with a six-month history of palpitations, heat intolerance, irritability, and unintentional weight loss of approximately 5 kg. His symptoms developed gradually and progressed over four months before medical evaluation. He had no history of medical or psychiatric illness, no family history of thyroid disease, and was not taking any regular medications or dietary supplements. He denied the use of herbal preparations or exposure to pesticides, industrial chemicals, or other substances known to influence thyroid function. Notably, he reported using only non-iodized rock salt for cooking and seasoning for the past three years.
On examination, his pulse rate was 96 beats per minute, and fine tremors were noted, but there was no evidence of goiter or orbitopathy. Cardiovascular, respiratory, and abdominal examinations were unremarkable. Thyroid function tests revealed suppressed TSH, elevated free T3, and normal free T4. Both the thyrotropin receptor antibody (TRAb) and anti-thyroid peroxidase antibody tests were negative. Other biochemical parameters, including liver and renal function, were within normal limits (Table 1).
Ultrasound of the thyroid demonstrated a diffusely enlarged, homogeneous gland with normal echogenicity and no nodules. Thyroid scintigraphy using technetium-99m pertechnetate revealed diffuse, homogeneous tracer uptake of 1.2%, which remained preserved despite suppressed TSH (Figure 1).
Thyroid scintigraphy with technetium-99m pertechnetate. (A) Anterior planar image showing diffuse, homogeneous tracer uptake in both lobes of the thyroid gland. (B) Same image with regions of interest drawn around each lobe for uptake quantification, showing a calculated thyroid uptake of 1.2%.
These findings initially suggested TRAb-negative Graves’ disease. The patient was started on carbimazole 20 mg/day and propranolol 40 mg/day (in two divided doses), along with dietary iodine repletion by replacing rock salt with iodized salt (~5 g/day). Carbimazole was tapered to 10 mg at six weeks and to 5 mg at three months based on thyroid function test results. Propranolol was gradually tapered and discontinued once the resting heart rate stabilized below 90 beats per minute and symptoms resolved, in accordance with the 2016 American Thyroid Association guidelines for the management of hyperthyroidism [9].
Although the patient’s clinic visits were less frequent than advised, he was compliant with carbimazole and regularly underwent thyroid function testing at each visit. At each review, he was specifically asked about medication adherence and consistently reported taking carbimazole as prescribed for nine months, after which he discontinued it on his own. Two months later, repeat thyroid function tests were normal. He remained clinically and biochemically euthyroid during 24 months of follow-up without medication, maintaining only dietary iodized salt. A summary of laboratory values and the clinical timeline is provided in Table 1 and Table 2.
Discussion
The differential diagnosis of T3-predominant thyrotoxicosis without goiter includes Graves’ disease, thyroiditis, and iodine deficiency-related autonomy [2-4]. Graves’ disease typically presents with diffuse homogeneous uptake on scintigraphy, diffuse non-nodular thyroid enlargement, and hypoechogenicity with hypervascularity on ultrasound [2]. In this patient, the absence of orbitopathy, negative thyroid antibodies, and sustained remission despite early discontinuation of carbimazole argued against Graves’ disease. In suppressed-TSH states, a pertechnetate uptake of approximately 1-2% is considered indicative of thyroid autonomy, as observed in this patient (1.2%), whereas Graves’ disease usually demonstrates uptake values exceeding 2% [7,9].
Iodine deficiency-related autonomy remained the most plausible etiology. The patient’s exclusive use of non-iodized rock salt provided a clear dietary basis for iodine deficiency, consistent with reports of persistent mild iodine deficiency in parts of India despite national iodization programs [6]. In deficiency states, a T3-predominant profile is expected because T3 synthesis requires fewer iodine atoms [2]. The preserved homogeneous uptake (1.2%) with suppressed TSH fits the pattern of diffuse or disseminated autonomy, in which the entire gland exhibits mild hyperfunction without nodularity [7,8]. Chronic iodine deficiency promotes clonal thyrocyte expansion, leading initially to diffuse autonomy that may later evolve into nodularity [10]. Sustained euthyroidism following iodine repletion and withdrawal of antithyroid therapy further supports iodine deficiency-induced thyrotoxicosis rather than Graves’ disease.
Thyroiditis was unlikely, as it typically produces T4-predominant thyrotoxicosis with low or absent uptake on scintigraphy [8,9]. In this case, preserved uptake excluded thyroiditis. Occupational or environmental exposure to thyroid-disrupting pesticides such as organochlorines, organophosphates, and pyrethroids was also ruled out based on history. These compounds have been shown to interfere with thyroid hormone synthesis, metabolism, and receptor signaling [11].
This case highlights the importance of obtaining a detailed dietary history in patients presenting with atypical thyrotoxicosis, particularly regarding iodized salt use in regions where mild iodine deficiency persists. It illustrates how iodine deficiency can mimic autoimmune hyperthyroidism, presenting with T3-predominant thyrotoxicosis, diffuse homogeneous uptake, and negative antibodies. Regular monitoring and structured follow-up are essential to confirm remission and prevent overtreatment, while awareness of iodine intake variability can help avoid unnecessary prolonged antithyroid or radioiodine therapy.
The main limitation of this report is the absence of urinary iodine concentration measurement, which would have objectively confirmed iodine deficiency. Ultrasound images were not archived, and repeat scintigraphy to calculate TSH-normalized uptake was not performed. Nevertheless, integration of dietary history, biochemical profile, imaging findings, and long-term follow-up provides a coherent and plausible diagnosis of iodine deficiency-induced thyrotoxicosis.
Table 3 summarizes the distinguishing clinical, imaging, biochemical, and hormonal features of Graves’ disease, iodine deficiency-related autonomy, and thyroiditis.
Conclusions
This case illustrates how iodine deficiency can mimic autoimmune hyperthyroidism, presenting as T3-predominant thyrotoxicosis with diffuse homogeneous uptake despite negative antibodies. Sustained remission following dietary iodine repletion underscores the diagnostic value of follow-up, as such a course is uncommon in Graves’ disease. Although universal salt iodization has reduced iodine deficiency globally, pockets of risk persist due to dietary practices and cultural factors. Clinicians should therefore consider iodine deficiency in the differential diagnosis of atypical thyrotoxicosis and obtain a thorough dietary history before initiating long-term antithyroid therapy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global, regional, and national burdens of common micronutrient deficiencies from 1990 to 2019: a secondary trend analysis based on the Global Burden of Disease 2019 study E Clinical Medicine Han X Ding S Lu J Li Y 1012994420223519892310.1016/j.eclinm.2022.101299 PMC 8850322 · doi ↗ · pubmed ↗
- 2Williams Textbook of Endocrinology, 14th Edition Melmed S Koenig R Rosen CJ Auchus RJ Goldfine AB Philadelphia, PA Elsevier 2019
- 3Iodine deficiency and thyroid disorders Lancet Diabetes Endocrinol Zimmermann MB Boelaert K 2862953201512559146810.1016/S 2213-8587(14)70225-6 · doi ↗ · pubmed ↗
- 4Iodine intake as a determinant of thyroid disorders in populations Best Pract Res Clin Endocrinol Metab Laurberg P Cerqueira C Ovesen L 13272420102017246710.1016/j.beem.2009.08.013 · doi ↗ · pubmed ↗
- 5Comparative study of thyroid function and types of thyroid dysfunction in two areas in Denmark with slightly different iodine status Eur J Endocrinol Knudsen N Bülow I Jørgensen T Laurberg P Ovesen L Perrild H 48549114320001102219410.1530/eje.0.1430485 · doi ↗ · pubmed ↗
- 6Usage of non-iodized salt in North West India Thyroid Res Pract Kalra S Kalra B Sawhney K 12141020131
- 7Integrated thyroid imaging: ultrasound and scintigraphy Integrated Diagnostics and Theranostics of Thyroid Diseases Schenke SA Groener D Grunert M Stahl AR Cham Springer 2023
- 8Scintigraphic manifestations of thyrotoxicosis Radiographics Intenzo CM de Papp AE Jabbour S Miller JL Kim SM Capuzzi DM 8578692320031285366110.1148/rg.234025716 · doi ↗ · pubmed ↗