Very Early Recurrence Following Liver Resection for Intrahepatic Cholangiocarcinoma: Is It Predictable by Clinical Preoperative Factors?
Francesco Ardito, Francesco Razionale, Andrea Campisi, Çınar Turgay, Alessandro Coppola, Simone Vani, Maria Vellone, Felice Giuliante

TL;DR
This study finds that pre-surgery clinical factors cannot reliably predict early recurrence in liver cancer patients, suggesting a need for better diagnostic methods.
Contribution
The study shows that preoperative clinical factors alone cannot accurately predict very early recurrence in intrahepatic cholangiocarcinoma patients.
Findings
Very early recurrence occurred in 20.5% of patients after liver resection for ICC.
Preoperative clinical factors failed to identify patients at high risk for very early recurrence.
Patients with very early recurrence had significantly worse 5-year survival rates (0% vs. 48.7%).
Abstract
Approximately one‐quarter of patients undergoing resection for intrahepatic cholangiocarcinoma (ICC) experience very early recurrence (within 6 months after liver resection), which is associated with a poor prognosis. Identifying factors associated with very early recurrence may help optimize patient selection for surgery and avoid futile, high‐risk hepatectomies. The aim of this study was to assess whether preoperative clinical factors alone can reliably predict very early recurrence following curative liver resection for ICC. A retrospective analysis was conducted on 83 patients who underwent liver resection between 2010 and 2020. The 5‐year overall survival (OS) rate for the entire cohort was 51.4%. Recurrence occurred in 54 patients (65.1%), with 17 (20.5%) experiencing very early recurrence. The 5‐year OS for patients with very early recurrence was significantly lower than for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
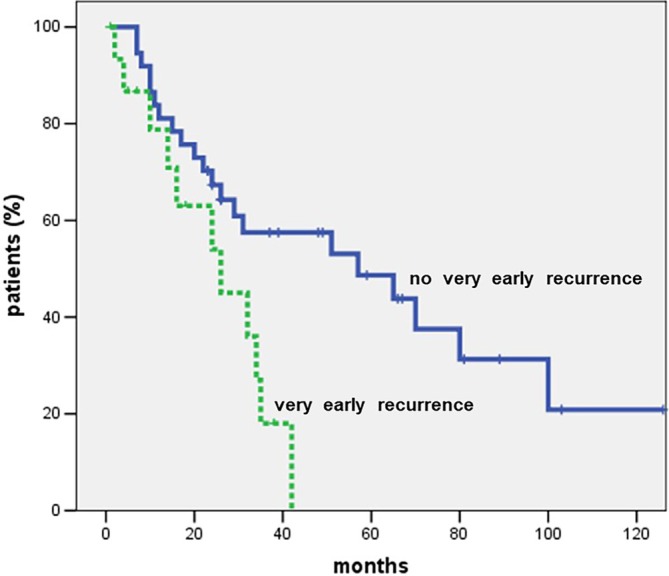 FIGURE 1
FIGURE 1| Variable | No. (%)/median [IQR range] |
|---|---|
| Age, years | 66 [60–73] |
| Male sex | 45 (54.2) |
| ASA score ≤ 2 | 62 (74.7) |
| BMI, kg/m2 | 25 [24–29] |
| Overweight patients (BMI 25–29.9) | 34 (41.0) |
| Obese patients (BMI ≥ 30) | 13 (15.7) |
| Cirrhosis | 5 (6.0) |
| HBV | 8 (9.6) |
| HCV | 4 (4.8) |
| CA19‐9 (U/mL) | 37.2 [10.6–142.6] |
| Neoadjuvant chemotherapy | 10 (12.0) |
| Variable | No. (%)/median [IQR range] |
|---|---|
| Major liver resection | 59 (71.1) |
| Laparoscopic approach | 12 (14.5) |
| Pedicle clamping | 74 (89.1) |
| Intraoperative blood transfusions | 6 (7.2) |
| Postoperative complications | 37 (44.6) |
| Severe postoperative complications | 15 (18.1) |
| Reintervention | 4 (4.8) |
| 90‐day mortality | 1 (1.2) |
| Hospital stay, days | 9 [9–12] |
| Variable | No. (%)/median [IQR range] |
|---|---|
| Tumor size, mm | 60 [60.0–87.5] |
| Pattern of distribution of nodules | |
| Type I—single | 59 (71.1) |
| Type II—single with satellites | 8 (9.6) |
| Type III—multifocal | 16 (19.3) |
| AJCC 8th edition pT stage | |
| T1a | 19 (22.9) |
| T1b | 18 (21.7) |
| T2 | 28 (33.7) |
| T3 | 11 (13.3) |
| T4 | 7 (8.4) |
| AJCC 8th edition pN stage | |
| N0 | 53 (63.9) |
| N1 | 30 (36.1) |
| Harvested lymph nodes | 5 [5–8] |
| Perineural invasion | 14 (16.9) |
| Microvascular invasion | 9 (10.8) |
| Radicality of resection | |
| R0 | 66 (79.5) |
| R1 | 17 (20.5) |
| Adjuvant chemotherapy | 18 (22.0) |
| Variable | No. (%)/median [IQR range] |
|---|---|
| Pattern of recurrence | |
| Only intrahepatic | 33 (71.1) |
| Only extrahepatic | 7 (9.6) |
| Both | 14 (19.3) |
| Timing of recurrence | |
| Very early (≤ 6 months) | 17 (20.5) |
| Early (> 6 months, ≤ 12 months) | 16 (19.3) |
| Late (> 12 months) | 21 (25.3) |
| Variable | Very early recurrence (no. 17) | Early recurrence (no. 16) | Late recurrence (no. 21) | p |
|---|---|---|---|---|
| Age ≥ 65 years | 12 (70.6%) | 5 (31.2%) | 16 (76.2%) | 0.611 |
| Male sex | 6 (35.3%) | 13 (81.2%) | 9 (42.9%) | 0.768 |
| ASA score > 2 | 7 (41.2%) | 2 (12.5%) | 3 (14.3%) | 0.057 |
| BMI ≥ 25 | 8 (47.1%) | 12 (75.0%) | 12 (57.1%) | 0.241 |
| Preop. CA 19‐9 > 54 U/mL | 5 (29.4%) | 7 (43.7%) | 5 (23.8%) | 0.364 |
| Cirrhosis | 0 | 1 (6.2%) | 3 (14.3%) | 0.096 |
| Neoadjuvant chemotherapy | 2 (11.8%) | 0 | 2 (9.5%) | 0.857 |
| Tumor size > 5 cm | 14 (82.3%) | 11 (68.7%) | 7 (33.4%) | 0.001 |
| Multifocal tumors | 8 (47.1%) | 5 (31.2%) | 0 | < 0.001 |
| Intraoperative blood transfusions | 2 (11.8%) | 1 (6.2%) | 0 | 0.118 |
| Severe postoperative complications | 1 (5.9%) | 1 (6.2%) | 4 (19.0%) | 0.192 |
| T3–T4 | 7 (41.2%) | 1 (6.2%) | 7 (33.4%) | 0.762 |
| N1 | 8 (47.1%) | 10 (62.5%) | 6 (28.6%) | 0.223 |
| Perineural invasion | 3 (17.6%) | 1 (6.2%) | 4 (19.0%) | 0.855 |
| Microvascular invasion | 3 (17.6%) | 0 | 2 (9.5%) | 0.451 |
| R1 resection | 5 (29.4%) | 4 (25.0%) | 3 (14.3%) | 0.266 |
| Adjuvant chemotherapy | 3 (17.6%) | 3 (18.7%) | 5 (23.8%) | 0.794 |
| Variable | Univariable analysis |
| Multivariable analysis |
| ||
|---|---|---|---|---|---|---|
| No. (%) | 5‐year OS | HR | 95% CI | |||
| Age (years) | 0.713 | |||||
| < 65 | 36 (43.4) | 42.7 | ||||
| ≥ 65 | 47 (56.6) | 57.5 | ||||
| Sex | 0.988 | |||||
| Male | 45 (54.2) | 55.3 | ||||
| Female | 38 (45.8) | 46.2 | ||||
| ASA score | 0.963 | |||||
| ≤ 2 | 62 (74.7) | 52.2 | ||||
| > 2 | 21 (25.3) | 49.1 | ||||
| BMI (kg/m2) | 0.867 | |||||
| < 25 | 36 (43.4) | 51.7 | ||||
| Overweight/obese patients (≥ 25) | 47 (56.6) | 49.8 | ||||
| Viral hepatitis | 0.552 | |||||
| Yes | 12 (14.5) | 62.5 | ||||
| No | 71 (85.5) | 49.9 | ||||
| Preop. CA 19‐9 > 54 U/mL | ||||||
| Yes | 22 (26.5) | 22.1 | 0.002 | |||
| No | 61 (73.5) | 64.8 | ||||
| Major liver resection | 0.066 | |||||
| Yes | 59 (71.1) | 45.7 | ||||
| No | 24 (28.9) | 64.5 | ||||
| Laparoscopic approach | 0.605 | |||||
| Yes | 12 (14.5) | 64.6 | ||||
| No | 71 (85.5) | 50.0 | ||||
| Intraoperative blood transfusions | 0.030 | |||||
| Yes | 6 (7.2) | 0 | ||||
| No | 77 (92.8) | 53.8 | ||||
| Severe postoperative complications | 0.573 | |||||
| Yes | 15 (18.1) | 67.7 | ||||
| No | 68 (81.9) | 37.7 | ||||
| Tumor size | 0.008 | |||||
| ≤ 5 cm | 39 (47.0) | 72.8 | ||||
| > 5 cm | 44 (53.0) | 29.0 | ||||
| No. of tumors | 0.003 | |||||
| Single | 59 (71.1) | 61.2 | ||||
| Single with satellites | 8 (9.6) | 28.6 | ||||
| Multifocal | 16 (19.3) | 26.9 | ||||
| T stage | 0.119 | |||||
| T1–T2 | 65 (78.3) | 54.3 | ||||
| T3–T4 | 18 (21.7) | 32.8 | ||||
|
| 0.021 | |||||
| N0 | 53 (63.9) | 55.6 | ||||
| N1 | 30 (36.1) | 41.1 | ||||
| Perineural invasion | 0.267 | |||||
| Yes | 14 (16.9) | 46.2 | ||||
| No | 69 (83.1) | 53.0 | ||||
| Microvascular invasion | 0.343 | |||||
| Yes | 9 (10.8) | 33.3 | ||||
| No | 74 (89.2) | 53.3 | ||||
| Radicality of resection | < 0.001 | 3.118 | 1.467–6.627 | 0.003 | ||
| R0 | 66 (79.5) | 62.2 | ||||
| R1 | 17 (20.5) | 9.6 | ||||
| Timing of recurrence | ||||||
| Very early vs. no very early | 0.013 | 2.891 | 1.214–6.884 | 0.016 | ||
| Very early | 17 (31.5) | 0 | ||||
| No very early | 37 (68.5) | 48.7 | ||||
| Very early vs. early vs. late | < 0.001 | |||||
| Very early | 17 (31.5) | 0 | ||||
| Early | 16 (29.6) | 15.6 | ||||
| Late | 21 (38.9) | 70.9 | ||||
| Adjuvant chemotherapy | 0.762 | |||||
| Yes | 18 (21.7) | 63.2 | ||||
| No | 65 (78.3) | 54.7 | ||||
| Variable | Univariable analysis | OR (95% CI) |
|---|---|---|
| Age ≥ 65 years | 0.157 | |
| Male sex | 0.529 | |
| ASA score > 2 | 0.467 | |
| BMI ≥ 25 | 0.445 | |
| Preoperative CA 19‐9 > 54 U/mL | 0.026 | 4.817 (1.203–19.285) |
| Cirrhosis | 0.522 | |
| Neoadjuvant chemotherapy | 0.067 | |
| Tumor size > 5 cm | 0.118 | |
| Multifocal tumors | 0.177 | |
| T3‐T4 | 0.093 | |
| N1 | 0.087 | |
| Perineural invasion | 0.409 | |
| Microvascular invasion | 0.457 | |
| R1 resection | 0.700 | |
| Adjuvant chemotherapy | 0.676 |
| Variable | Univariable analysis | Multivariable analysis OR (95% CI) |
|
|---|---|---|---|
| Age ≥ 65 years | 0.336 | ||
| Male sex | 0.104 | ||
| ASA score > 2 | 0.029 | ||
| BMI ≥ 25 | 0.037 | 0.223 (0.055–0.901) | 0.035 |
| Preoperative CA 19‐9 > 54 U/mL | 0.764 | ||
| Cirrhosis | 0.999 | ||
| Neoadjuvant chemotherapy | 0.418 | ||
| Tumor size > 5 cm | 0.026 | 5.721 (1.236–26.486) | 0.026 |
| Multifocal tumors | 0.029 | ||
| T3–T4 | 0.158 | ||
| N1 | 0.793 | ||
| Perineural invasion | 0.692 | ||
| Microvascular invasion | 0.171 | ||
| R1 resection | 0.392 | ||
| Adjuvant chemotherapy | 0.712 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCholangiocarcinoma and Gallbladder Cancer Studies · Gallbladder and Bile Duct Disorders · Pancreatic and Hepatic Oncology Research
Introduction
1
Intrahepatic cholangiocarcinoma (ICC) is the second most common primary liver tumor, accounting for approximately 10%–15% of all primary liver cancers [1]. Its incidence has been steadily increasing worldwide on an annual basis [2, 3].
Currently, complete surgical resection is the only potentially curative treatment for ICC, although it is feasible in only 30%–40% of patients [4]. However, long‐term outcomes after curative liver resection remain poor, with reported 5‐year overall survival rates ranging from 20% to 40% [5, 6, 7]. These disappointing results are largely attributable to the high rate of tumor recurrence following surgery, which occurs in 50%–70% of cases [8, 9, 10].
Several studies have analyzed overall survival based on the timing of recurrence after liver resection [7, 11]. These studies demonstrated that patients experiencing early recurrence (within 24 months) have a worse prognosis and a distinct recurrence pattern compared to those with late recurrence (> 24 months) [7, 11]. However, the commonly used 2‐year cutoff to define early recurrence may not be appropriate for patients undergoing resection for ICC. In fact, the majority of these patients tend to experience recurrence within the first 12 months after surgery [10], and approximately one‐quarter present with very early recurrence (within 6 months) [11]. Very early recurrence is associated with a significantly worse prognosis and a lower likelihood of undergoing repeat resection, raising concerns about the potential futility of liver resection in this subset of patients [12, 13].
For these reasons, recent studies have focused on identifying factors associated with early recurrence (within 1 year) and very early recurrence (within 6 months) following liver resection for ICC [12, 13, 14]. Identifying patients at high risk of very early recurrence may help guide selection for liver resection versus alternative treatment strategies, may help to plan neoadjuvant chemotherapy, and enable the personalization of postoperative surveillance protocols.
The aim of this study was to evaluate whether preoperative clinical factors alone are sufficient to predict recurrence, particularly very early recurrence, after curative liver resection for ICC, and to assess how effectively these factors can be applied in real‐world clinical practice at both individual and institutional levels.
Materials and Methods
2
This study is a retrospective observational analysis conducted at a single center. It included patients who underwent liver resection for ICC between January 2010 and December 2020 at our institution. Only patients who underwent curative‐intent resection were included in the analysis. Patients with a final pathological diagnosis of combined primary liver tumors (e.g., hepatocholangiocarcinoma) were excluded. All included patients were evaluated by thoracoabdominal computed tomography (CT) and abdominal magnetic resonance imaging (MRI) [15]. In cases of preoperative suspicion of locoregional lymph node involvement, patients were considered for neoadjuvant chemotherapy with gemcitabine plus cisplatin. Radiological re‐evaluation was performed at 3 and 6 months. In cases of favorable response or stable disease, liver resection was subsequently planned. Criteria for radiologically suspicious regional lymph nodes included a short‐axis diameter greater than 1 cm and the presence of contrast enhancement on preoperative imaging. In cases with radiological suspicion of peritoneal carcinomatosis or distant metastatic lymph node involvement, a PET scan was performed. Liver resections were classified according to the terminology of the International Hepato‐Pancreato‐Biliary Association (IHPBA) [16]. Resections involving three or more liver segments were defined as major hepatectomies. The surgical technique for liver resection adopted in our unit has been previously described [17, 18]. All patients underwent regional lymphadenectomy, which included dissection of the hilar, pericholedochal, hepatic artery, periportal, and superior retropancreatic lymph nodes [19]. Regional lymphadenectomy was routinely performed in all cases, regardless of whether the liver resection was classified as major or minor. The same lymphadenectomy protocol was applied consistently in both open and laparoscopic approaches.
The following data were collected for each patient: demographic information, presence of underlying chronic liver disease, and use of neoadjuvant chemotherapy. The cutoff value for preoperative CA 19‐9 was set at 54 U/mL, based on a recent multicenter study by Wei T. et al. [20], which analyzed 1095 resected patients and identified CA 19‐9 > 54 U/mL as one of the strongest predictors of both overall survival (OS) and disease‐free survival (DFS). Operative details collected included the type of resection, use of pedicle clamping, and intraoperative blood transfusions. Early outcomes encompassed postoperative complications and 90‐day mortality. Postoperative complications were graded according to the Clavien‐Dindo classification system [21], with severe complications defined as Clavien‐Dindo grade ≥ 3. Late outcomes included 5‐year OS and DFS rates.
Tumor staging was performed according to the TNM classification of the UICC staging system, 8th Edition [22]. Pathological data included the presence of perineural invasion, resection margin status, and lymph node involvement. An R0 resection was defined as the absence of microscopic tumor invasion at the resection margin (tumor‐free margin ≥ 1 mm), while R1 resection indicated complete macroscopic removal with microscopic tumor invasion at the margin (tumor‐free margin = 0 mm). Following the classification proposed by Conci et al. [23], tumor nodules were categorized as: single tumor (type I); single tumor with satellite nodules within the same Couinaud liver segment (type II); and multifocal tumors involving different Couinaud liver segments (type III).
Adjuvant chemotherapy with gemcitabine was administered to patients with T3 to T4 tumors or those with lymph node metastases. Follow‐up consisted of serum CA 19‐9 measurement and thoracoabdominal CT scans every 3 months for the first 2 years, then every 6 months for the subsequent 3 years. Time to recurrence was defined as the interval between liver resection and the detection of any recurrence on radiological imaging. Very early recurrence was defined as recurrence occurring within 6 months after liver resection [13, 14]. Early recurrence was defined as recurrence occurring between 6 and 12 months post‐resection, while late recurrence referred to recurrence occurring more than 12 months after surgery.
Based on the paper by Tsilimigras et al. [14], we applied their very early recurrence calculator and scoring system to stratify the prognosis of resected patients in our analysis. Preoperative and postoperative risk scores for the likelihood of very early recurrence were calculated for each patient. The variables included in the preoperative risk score were age, race, presence of cirrhosis, tumor size, number of lesions, and suspicion of positive regional lymph nodes. The postoperative risk score incorporated age, race, tumor size, number of lesions, microvascular invasion, positive regional lymph nodes, and margin status. Patients were classified into three distinct risk groups for very early recurrence (low, intermediate, and high) based on either the preoperative or postoperative scores. According to the Tsilimigras et al. scoring system, patients were stratified into risk groups as follows: for the preoperative score, 0–3 (low risk), 4–5 (intermediate risk), and 6–9 (high risk); for the postoperative score, 0–4 (low risk), 5–6 (intermediate risk), and 7–10 (high risk).
The primary objective of this study was to evaluate whether clinical preoperative factors alone are sufficient to predict recurrence, particularly very early recurrence, following curative liver resection for ICC. The study was conducted in accordance with the Declaration of Helsinki and received approval from the Institutional Review Board of the Catholic University of the Sacred Heart on 17 March 2022 (Prot. n. 0010136/22; ID: 4832). Continuous variables are presented as medians and interquartile ranges (IQR), while categorical variables are expressed as counts and percentages. OS was calculated from the date of liver resection to the date of death or censored at the last follow‐up. Survival curves were generated using the Kaplan–Meier method and compared using the log‐rank test. Multivariable regression analyses were performed to identify independent prognostic factors for OS, recurrence, and very early recurrence. Variables with p < 0.2 in univariate analysis were included in a Cox proportional hazards model with backward elimination. A p value < 0.05 was considered statistically significant in all analyses. Statistical analyses were conducted using SPSS version 23.0 (SPSS Inc., Chicago, IL, USA). This work has been reported in accordance with the STROCSS criteria [24].
Results
3
Between January 2010 and December 2020, a total of 91 liver resections were performed in 83 patients (8 of whom underwent re‐resection for liver recurrence), who constitute the study cohort. Table 1 summarizes the clinical characteristics of these 83 patients. Underlying chronic liver disease of viral etiology was documented in 12 patients (14.5%). Overall, 47 patients (56.6%) had a body mass index (BMI) ≥ 25. Of the 83 patients, 59 (71.1%) underwent major liver resection (Table 2). Twelve patients (14.5%) underwent laparoscopic liver resection. The use of the laparoscopic approach increased over time, from 8.2% (4/49) between 2010 and 2015 to 23.5% (8/34) between 2016 and 2020. This increase was statistically significant (p = 0.05). Fifty‐nine patients (71.1%) underwent resection for a single nodule. The distribution pattern of nodules is detailed in Table 3. Lymph node metastases were identified in 30 patients (36.1%). Sixty‐six patients (79.5%) achieved R0 liver resection.
After a median follow‐up of 27 months (IQR = 27–60 months), the 5‐year OS was 51.4% (median OS = 65 months). Fifty‐four patients (65.1%) experienced recurrence following liver resection. The 5‐year DFS was 33.9% (median DFS = 22 months). The pattern of recurrence is detailed in Table 4. Seventeen patients (20.5%) developed very early recurrence (within 6 months after liver resection). Among patients with recurrence within 12 months post‐resection, 69.7% (23 patients) had exclusively intrahepatic recurrence, while 30.3% (10 patients) exhibited extrahepatic recurrence with or without intrahepatic involvement. For recurrences occurring more than 12 months after surgery, 47.6% (10 patients) presented with only intrahepatic recurrence, and 52.4% (11 patients) had extrahepatic recurrence with or without intrahepatic disease. Clinical and pathological factors stratified by time of recurrence are summarized in Table 5. Timing of recurrence was significantly associated with OS; specifically, very early recurrence correlated with a markedly lower 5‐year OS compared to early or late recurrence (Figure 1). In univariate analysis, predictors of poor OS included: preoperative CA 19‐9 > 54 U/mL (p = 0.002); intraoperative blood transfusions (p = 0.030); tumor size > 5 cm (p = 0.008); multiple tumors (p = 0.003); positive lymph nodes (p = 0.021); R1 resection (p < 0.001); and occurrence of very early recurrence (p = 0.013). Multivariable analysis identified R1 resection (HR = 3.118; p = 0.003) and very early recurrence (HR = 2.891; p = 0.016) as independent predictors of poor OS (Table 6).
Five‐year OS according to the timing of recurrence (very early recurrence vs. no very early recurrence). Five‐year OS in patients with very early recurrence was signifi‐cantly lower than that observed in patients with no very early recurrence (0 vs. 48.7%, re‐spectively; p = 0.013). The median survival was 26 months in patients with very early re‐currence and 57 months in patients without very early recurrence.
In univariate regression analysis, a CA 19‐9 level > 54 U/mL was significantly associated with an increased likelihood of recurrence (OR 4.817; 95% CI 1.203–19.285) (Table 7). In multivariable regression analysis, tumor size > 5 cm was independently associated with a higher risk of very early recurrence (OR 5.721; 95% CI 1.236–26.486), while a BMI ≥ 25 was associated with a lower risk of very early recurrence (OR 0.223; 95% CI 0.055–0.901) (Table 8).
According to the preoperative very early recurrence score described by Tsilimigras et al. [14], 77 patients (92.8%) were classified as low risk, 5 patients (6.0%) as intermediate risk, and 1 patient (1.2%) as high risk. Five‐year OS differed significantly among the three groups: 51.0% in the low‐risk group, 8.0% in the intermediate‐risk group, and 0% in the high‐risk group (p = 0.047). The rate of very early recurrence was 21.0% (16/77) in low‐risk patients, 20.0% (1/5) in intermediate‐risk patients, and 0% in high‐risk patients. Five‐year recurrence‐free survival (RFS) rates, however, were not significantly different across the groups: 34.7% (low risk), 40.0% (intermediate risk), and 0% (high risk) (p = 0.788). The preoperative scoring system stratified patients into three groups based on scores of 0–3, 4–5, and 6–9. The corresponding 5‐year RFS rates were 40.6%, 24.7%, and 20.0%, respectively, with no statistically significant difference (p = 0.124). Using the postoperative very early recurrence score, 61 patients (73.5%) were classified as low risk, 14 (16.9%) as intermediate risk, and 8 (9.6%) as high risk. Five‐year OS significantly differed among these groups: 40.0% for low risk, 34.1% for intermediate risk, and 0% for high risk (p = 0.006). The rates of very early recurrence were 18.0% (11/61) in the low‐risk group, 28.6% (4/14) in the intermediate‐risk group, and 25.0% (2/8) in the high‐risk group. Five‐year RFS rates showed a trend toward difference but did not reach statistical significance: 39.5% (low risk), 17.5% (intermediate risk), and 0% (high risk) (p = 0.062). The postoperative scoring system also categorized patients into three groups based on scores of 0–4, 5–6, and 7–10. The corresponding 5‐year RFS rates were 39.5%, 17.5%, and 0%, respectively, without reaching statistical significance (p = 0.062).
Discussion
4
This study confirmed that curative liver resection for ICC can be achieved in approximately 80% of selected patients (rate of R0 resections: 79.5%). The perioperative outcomes were acceptable, with a 90‐day mortality rate of 1.2% and a severe complication rate of 18.1%. The majority of patients (71.1%) underwent major hepatectomies, reflecting the typically advanced stage of ICC at presentation. The median tumor size was 6 cm, and the cohort showed a high prevalence of overweight and obesity (41.0% and 15.7%, respectively), consistent with recognized ICC risk factors [25]. Long‐term outcomes were comparable to existing literature, with a 5‐year overall survival (OS) rate of 51.4% [25]. Importantly, R1 resection and very early recurrence (within 6 months) were identified as independent predictors of poor OS (HR = 3.118, p = 0.003; HR = 2.891, p = 0.016). Recurrence occurred in 65.1% of patients, and 20.5% experienced very early recurrence, which was associated with a 0% 5‐year OS. Predictive factors for recurrence included preoperative CA 19‐9 > 54 U/mL and predictive factors for very early recurrence included tumor size > 5 cm. The prognostic scoring system by Tsilimigras et al. [14] was validated, but its practical utility was limited due to the retrospective selection bias and the predominance of resected patients who belong to the low‐risk group (92.8%).
The findings emphasize the critical prognostic role of resection margin status [26, 27] and recurrence timing [28]. Achieving R0 resection remains essential for improving long‐term survival, and careful patient selection is key. However, the high rate of very early recurrence (21.0%) even among patients classified preoperatively as low risk suggests that conventional clinicopathological criteria are insufficient to guide surgical decisions.
Given the limitations of clinical predictors, the study supports the integration of radiomics features and molecular data to enhance prognostication. Preoperative CT‐based radiomics models and molecular subtyping have demonstrated promise in identifying patients at high risk for recurrence [29, 30, 31]. These tools could help refine treatment algorithms, identify candidates for neoadjuvant therapy, or consider alternative strategies in borderline cases. Moreover, metrics like sarcopenia may further aid in developing tailored approaches that move beyond one‐size‐fits‐all surgery [32].
A key strength of this study lies in its comprehensive analysis of recurrence dynamics and prognostic factors within a relatively large and well‐characterized cohort. However, its retrospective design introduces potential selection bias, especially regarding the preoperative risk stratification. The limited proportion of patients classified as intermediate‐ or high risk preoperatively may have reduced the generalizability of the Tsilimigras score in real‐world settings. Future prospective studies should incorporate radiomics, molecular, and functional parameters (e.g., sarcopenia, performance status) to develop more robust predictive models. Research should also explore the potential benefit of neoadjuvant therapies in high‐risk subsets to mitigate very early recurrence.
Conclusions
5
In summary, approximately one in five patients undergoing curative‐intent liver resection for ICC experiences very early recurrence, which is strongly associated with dismal long‐term outcomes. Conventional clinical parameters alone are inadequate for guiding treatment decisions in this population. Incorporating radiomics, molecular, and functional markers holds the potential to improve risk stratification, personalize care, and ultimately enhance survival in resectable ICC.
Author Contributions
Francesco Ardito: conceptualization, methodology, project administration, supervision, writing – review and editing. Francesco Razionale: data curation, formal analysis, investigation, writing – original draft. Andrea Campisi: data curation, formal analysis, investigation, writing – original draft. Çınar Turgay: data curation, formal analysis, investigation, writing – original draft. Alessandro Coppola: methodology, validation, writing – original draft, writing – review and editing. Simone Vani: data curation, formal analysis, resources, software. Maria Vellone: conceptualization, supervision, validation, writing – original draft, writing – review and editing. Felice Giuliante: conceptualization, supervision, validation, writing – review and editing.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cholangiocarcinoma Working Group , “Italian Clinical Practice Guidelines on Cholangiocarcinoma—Part I: Classification, Diagnosis and Staging,” Digestive and Liver Disease 52, no. 11 (2020): 1282–1293.32893173 10.1016/j.dld.2020.06.045 · doi ↗ · pubmed ↗
- 2L. Wu , D. I. Tsilimigras , A. Z. Paredes , et al., “Trends in the Incidence, Treatment and Outcomes of Patients With Intrahepatic Cholangiocarcinoma in the USA: Facility Type Is Associated With Margin Status, Use of Lymphadenectomy and Overall Survival,” World Journal of Surgery 43, no. 7 (2019): 1777–1787.30820734 10.1007/s 00268-019-04966-4 · doi ↗ · pubmed ↗
- 3J. M. Banales , J. J. G. Marin , A. Lamarca , et al., “Cholangiocarcinoma 2020: The Next Horizon in Mechanisms and Management,” Nature Reviews. Gastroenterology & Hepatology 17, no. 9 (2020): 557–588.32606456 10.1038/s 41575-020-0310-z PMC 7447603 · doi ↗ · pubmed ↗
- 4Cholangiocarcinoma Working Group , “Italian Clinical Practice Guidelines on Cholangiocarcinoma—Part II: Treatment,” Digestive and Liver Disease 52, no. 12 (2020): 1430–1442.32952071 10.1016/j.dld.2020.08.030 · doi ↗ · pubmed ↗
- 5G. Nuzzo , F. Giuliante , F. Ardito , et al., “Intrahepatic Cholangiocarci‐Noma: Prognostic Factors After Liver Resection,” Updates in Surgery 62, no. 1 (2010): 11–19.20845096 10.1007/s 13304-010-0007-x · doi ↗ · pubmed ↗
- 6M. N. Mavros , K. P. Economopoulos , V. G. Alexiou , and T. M. Pawlik , “Treatment and Prognosis for Patients With Intrahepatic Cholan‐Giocarcinoma: Systematic Review and Meta‐Analysis,” JAMA Surgery 149, no. 6 (2014): 565–574.24718873 10.1001/jamasurg.2013.5137 · doi ↗ · pubmed ↗
- 7A. Doussot , M. Gonen , J. K. Wiggers , et al., “Recurrence Patterns and Disease‐Free Survival After Resection of Intrahepatic Cholangiocarcinoma: Preoperative and Postoperative Prognostic Models,” Journal of the American College of Surgeons 223, no. 3 (2016): 493–505.27296525 10.1016/j.jamcollsurg.2016.05.019PMC 5003652 · doi ↗ · pubmed ↗
- 8J. Bridgewater , P. R. Galle , S. A. Khan , et al., “Guidelines for the Diagnosis and Man‐Agement of Intrahepatic Cholangiocarcinoma,” Journal of Hepatology 60, no. 6 (2014): 1268–1289.24681130 10.1016/j.jhep.2014.01.021 · doi ↗ · pubmed ↗