A Woman With Abdominal Pain
Fu Chi, Cheng-Han Chen

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
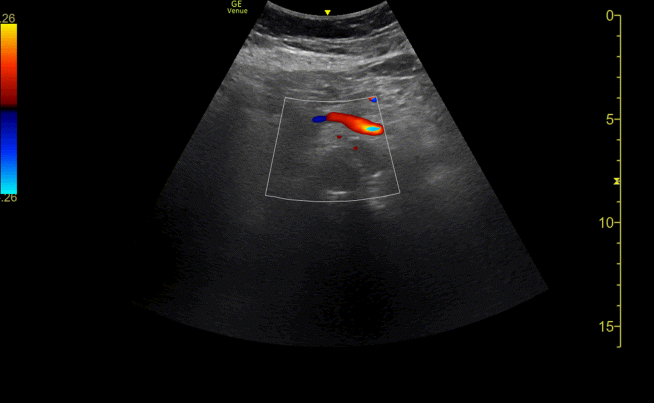 Figure 1
Figure 1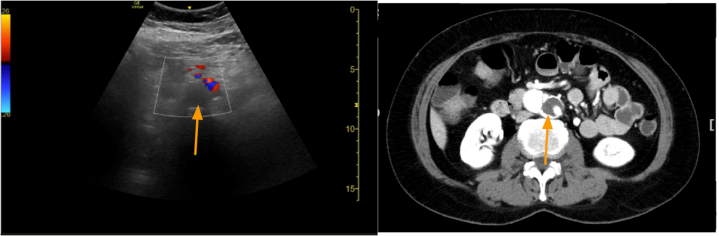 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntestinal and Peritoneal Adhesions · Appendicitis Diagnosis and Management · Abdominal vascular conditions and treatments
Patient Presentation
1
A 67-year-old woman presented to the emergency department with a 2-day history of intermittent chest tightness radiating to the back, accompanied by abdominal pain. On arrival, she was hemodynamically stable (blood pressure, 147/70 mm Hg; heart rate, 95 beats per minute). Abdominal examination was unremarkable. Laboratory evaluation revealed a white blood cell count of 6040/μL and a serum lactate level of 21.9 mg/dL.
Point-of-care ultrasonography with color Doppler demonstrated a filling defect in the abdominal aorta (Video 1). Computed tomographic angiography confirmed a Stanford type B aortic dissection with radiologic malperfusion of the true lumen (Fig 1). She was admitted with a diagnosis of type B aortic dissection complicated by bowel angina, attributed to compression of the true lumen at the level of the abdominal aorta and ostial stenosis of the superior mesenteric artery.Video 1Point-of-care ultrasonography with color Doppler shows a filling defect in the abdominal aorta.Figure 1. Point-of-care ultrasonography with color Doppler (left) showed a filling defect in the abdominal aorta (arrow), compatible with the findings in computed tomography angiography (right).
Type B aortic dissection with malperfusion: Type B aortic dissection (TBAD) occurs in 0.5 to 6.3 per 100,000 person-years.1 Malperfusion syndrome, present in 20% to 30% of cases, significantly increases morbidity and mortality.2^,^3 Early recognition is crucial as it transforms uncomplicated TBAD into a surgical emergency requiring immediate intervention.4
Point-of-care ultrasonography can provide rapid bedside assessment of aortic pathology. Although computed tomography angiography remains the gold standard, ultrasonography offers real-time evaluation of flow dynamics and can detect filling defects suggesting true lumen compression.4 In this case, the elevated lactate (21.9 mg/dL) indicated tissue hypoperfusion,2 prompting urgent imaging.
Complicated TBAD with malperfusion requires emergent endovascular or surgical intervention as optimal medical therapy alone is insufficient. Early ultrasonographic detection enables timely recognition of this life-threatening condition, potentially improving outcomes through rapid therapeutic intervention.2
Funding and Support
This work was supported by the National Science and Technology Council, Taiwan (Grant No. NSTC 114-2221-E-075-006), and by Taipei Veterans General Hospital, Taiwan (Grant No. V114B-001).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brooks M.Review of studies reporting the incidence of acute type B aortic dissection Hearts 132020152165
- 2Norton E.L.Williams D.M.Kim K.M.Management of acute type B aortic dissection with malperfusion via endovascular fenestration/stenting J Thorac Cardiovasc Surgery 1605202011511161.e 110.1016/j.jtcvs.2019.09.065PMC 710352031669033 · doi ↗ · pubmed ↗
- 3Chandra V.Norton E.L.Khaja M.S.Herrera D.G.Williams D.M.Yang B.Surgical and endovascular repair for type B aortic dissections with mesenteric malperfusion syndrome: a systematic review of in-hospital mortality JTCVS Open 12202237503659071610.1016/j.xjon.2022.07.012PMC 9801243 · doi ↗ · pubmed ↗
- 4Sobocinski J.Delloye M.Hongku K.Malperfusions in acute type B aortic dissection-predictors of outcomes Ann Vasc Surg 5920191191263103495010.1016/j.avsg.2019.01.030 · doi ↗ · pubmed ↗