Daily Cigarette Abstinence and Smoking Rate With Varenicline: Relationships With Treatment, Craving, and Affect During the First Week of the Quit Attempt
Sarah S Tonkin, Jennifer M Betts, Ashley N Dowd, Martin C Mahoney, Paul M Cinciripini, Robert A Schnoll, Tony P George, Rachel F Tyndale, Larry W Hawk Jr.

TL;DR
This study examines how smoking behavior changes in the first week of quitting, finding that varenicline and lower cravings help people stay smoke-free.
Contribution
The study introduces a new method to analyze smoking cessation by modeling both smoking probability and smoking rate.
Findings
Smoking probability increased on the quit day but remained stable in smoking rates.
Varenicline use was linked to lower smoking probability.
Craving and negative affect were associated with higher smoking probability and rates.
Abstract
Dichotomized smoking abstinence (abstinent/smoking) is the standard outcome for clinical trials, but obscures smoking behavior change. Examining both smoking probability and smoking rate as outcomes may identify unique barriers to cessation (eg, craving, affect) among individuals who are receiving treatment but unable to quit. Two-part latent growth modeling examined daily smoking probability and smoking rate during the first week of the quit attempt using self-reported cigarettes per day. Smoking trajectories and the effect of 12 weeks of varenicline (vs. placebo), craving, negative affect (NA), and positive affect (PA) on these trajectories were examined among 828 adults in a randomized smoking cessation trial (NCT01314001). On average, smoking probability was 46% on the target quit day and increased to 50% later into the week (ps < .01). Among participants continuing to smoke,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
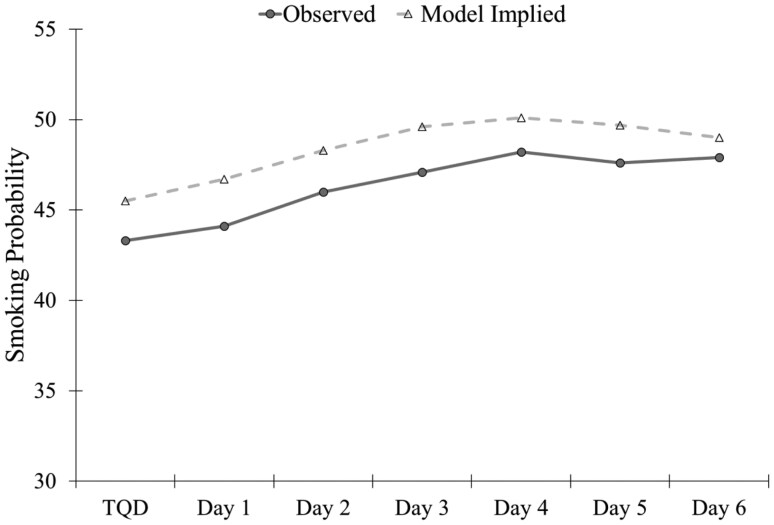 Figure 1
Figure 1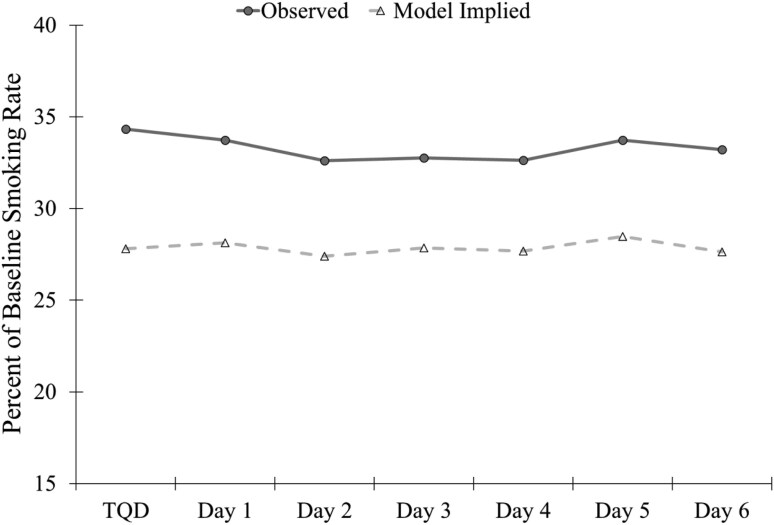 Figure 2
Figure 2- —National Institute on Drug Abuse, National Cancer Institute
- —National Institutes of Health10.13039/100000002
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSmoking Behavior and Cessation · Behavioral Health and Interventions · Mental Health Research Topics
Introduction
Over 34 million U.S. adults smoke cigarettes with about half reporting a past year quit attempt, but only 7%–8% report quitting.^1^ Though cessation yields the strongest health benefits, reducing cigarettes per day (CPD) improves the odds of abstinence in subsequent quit attempts.^2^ However, little research has evaluated treatment on daily smoking rates,^3,4^ and a call by The Society for Research on Nicotine and Tobacco advocates for clinical research to capture more detailed smoking outcomes.^5^ Traditionally, clinical trials dichotomize smoking status at one timepoint (eg, continuous abstinence at 6-month follow-up, 7-day point prevalence at end of treatment), overlooking nuanced information regarding smoking rates leading to conceptual challenges evaluating smoking behavior and methodological limitations (eg, reduced statistical power). Individuals who continue to smoke do so at varying rates, ranging from brief lapses to substantial reductions to a return to baseline smoking levels.^6^ Examining treatment effects and predictors of smoking rate versus cessation may inform interventions to lower daily smoking levels and re-initiate quit attempts.
Statistical techniques that simultaneously estimate the smoking probability and rates (ie, two-part latent growth modeling [LGM]) can inform how treatment uniquely affects these clinical outcomes.^7^ To date, no smoking cessation trials have used two-part LGMs to evaluate treatment effects and mechanisms on trajectories of smoking probability and rates. This study developed preliminary models to demonstrate the utility of two-part LGM via secondary analyses from a placebo-controlled varenicline trial.^5,8^ Varenicline provides an excellent initial test of this approach since it has shown efficacy for smoking abstinence and reducing smoking rates.^3^
Aim 1 characterized trajectories of smoking probability and smoking rates across the first week of the quit attempt. We focused on the first week since this is a critical window for lapse.^9,10^ Based on past research, the smoking probability was predicted to increase linearly across days,^11^ while smoking rates would either increase linearly or nonlinearly (eg, quadratic-rapid increases to stable smoking after a lapse).^6^ Aim 2 examined the effect of varenicline (vs. placebo) on trajectories of smoking probability and rates. It was predicted that participants in the varenicline group would have a lower probability of smoking and lower smoking rates based on prior clinical trials, including the parent trial for the current study.^3,8^ Additionally, work evaluating treatment mechanisms from the parent trial found that varenicline was associated with lower craving and negative affect (NA), which mediated binary smoking outcomes.^12^ However, it is unclear whether/how these processes separately impact day-level abstinence and smoking rates. Thus, Aim 3 tested whether higher craving and NA and lower positive affect (PA), were associated with higher smoking probability and smoking rates.
Materials and Methods
Participants and Procedure
Data were from a multi-site parent trial comparing smoking cessation treatments. Analyses included 828 adults randomly assigned to standard varenicline treatment or placebo. Inclusion criteria are described elsewhere (clinicaltrials.gov:NCT01314001).^8^ Procedures were approved by the institutional review board at each site and all participants provided informed consent. Of relevance to these analyses, participants answered questionnaires including timeline follow-back (TLFB) to assess the past week’s daily smoking at 1-week pre-quit (baseline), on the target quit day (TQD), and 1-week post-TQD. All participants were asked to abstain from smoking beginning the morning of their TQD.
Measures
Smoking outcomes included self-reported smoking probability (binary daily smoking; yes/no) and percent of baseline smoking rate (continuous daily smoking) across the first week of the quit attempt. Percent of baseline smoking rate was calculated from TLFB as (cigarettes smoked that day/average baseline CPD) × 100 (eg, smoking an average of 10 CPD across the baseline week and reducing to 3 cigarettes on the TQD would equal a smoking rate of 30% for that day). Current craving was assessed using the Questionnaire on Smoking Urges-Brief^13^ and past week NA and PA were assessed using the Positive and NA Schedule.^14^
Data Analysis
LGMs conducted in Mplus (version 8.10) evaluated trajectories of smoking probability and smoking rate over the first week of the quit attempt. Satorra-Bentler scaled chi-square difference tests compared model fit for nested tests with scaling corrections for non-normality. First, individual LGMs were estimated to determine the best-fitting trajectory for the slope of smoking probability and the slope of smoking rate.^15^ For smoking probability (binary), chi-square difference tests were used for nested comparisons of model log-likelihoods. For the smoking rate (continuous), MLR chi-square difference tests were used for nested model comparisons. Next, a two-part LGM simultaneously estimated smoking probability and rate on each of the first seven days of the quit attempt.^7^ The first “part” estimated day-to-day mean changes in smoking probability. Hypothetically, over the quit attempt, the average probability of smoking on the TQD maybe 50%, then increase to 55% on Day 1, a further increase to 60% on Day 2, etc. The second “part” estimated day-to-day mean changes in the smoking rate among those reporting smoking that day. Hypothetically, the average percent of baseline smoking rate maybe 20% on the TQD, then increase to 40% on Day 1 (smoking returning closer to baseline levels). Due to high collinearity with slope parameters, the intercept was assigned to Day 3 rather than Day 0 (TQD). Models separately evaluated the effect of treatment (Aim 2), craving, NA, and PA (Aim 3) on growth model parameters. Due to non-convergence, the quadratic slope term was removed for craving and PA models.
Results
See Table S1 for participant characteristics.
Aim 1: Trajectories of Smoking Probability and Rate
LGMs evaluated the fit of linear and quadratic slopes for smoking probability and smoking rate (Table S2). Nested chi-square tests indicated a random quadratic slope fit the data best for both smoking probability and smoking rate (ps < .001). Although there was significant individual variability in the quadratic slope for smoking rate (S^2^ = 0.50, p = .03), the mean estimate of the slope was nonsignificant (m = 0.01, p = .93). Further, estimation of the two-part LGM failed to converge with the inclusion of the quadratic slope for smoking rate. Since the linear slope model for smoking rate demonstrated an excellent fit and provided a more parsimonious solution, this model was used for the two-part LGM.
The estimated probability of smoking was lowest on the TQD (46%), increased through Day 4 (50%; mLinear = 0.13, SE = 0.05, p = .008), and remained stable through Day 6 (49%; mQuadratic = −0.06, SE = 0.03, p = .01; Figure 1). There was significant individual variability in the intercept (S^2^ = 27.88, SE = 4.09, p < .001), linear (S^2^ = 0.55, SE = 0.13, p < .001), and quadratic (S^2^ = 0.19, SE = 0.08, p = .02) slope of smoking probability. The estimated mean percent of baseline smoking rate remained stable throughout the week ranging from 27% to 28% (mLinear = 0.22, SE = 0.45, p = .62; Figure 2). There was significant individual variability in the intercept (S^2^ = 805.13, SE = 75.00, p < .001) and linear slope (S^2^ = 7.44, SE = 1.67, p < .001) of the smoking rate.
Observed and model implied mean smoking probability over the first week of the quit attempt. TQD = Target quit day.
Observed and model implied percent of baseline smoking rate over the first week of the quit attempt. TQD = Target quit day.
Aim 2: Effect of Varenicline on Trajectories of Smoking Probability and Rate
Treatment with varenicline was associated with the intercept (Day 3) of smoking probability (b = −1.88, SE = 0.46, p < .001) and smoking rate (b = −5.59, SE = 2.34, p = .02; Table S3). The estimated smoking probability was lower in the varenicline group (42%) compared to the placebo group (54%). Smoking rates were similar between the varenicline group (27%) and the placebo group (29%). Treatment was not significantly related to the slopes of smoking probability or smoking rate (ps > .28).
Aim 3: Effects of Craving and Affect on Trajectories of Smoking Probability and Rate
Craving
Higher pre-quit craving predicted a slightly less steep increase in the probability of smoking across the week (bLinear = −0.06, SE = 0.03, p = .051), while higher TQD craving predicted a higher probability of smoking on Day 3 (bIntercept = 0.63, SE = 0.19, p = .001) and higher smoking rates at Day 3 (bIntercept = 3.24, SE = 0.94, p = .001).
NA
Higher pre-quit NA marginally predicted higher smoking probability on Day 3 (bIntercept = 1.15, SE = 0.60, p = .054), while higher TQD NA predicted higher smoking rates on Day 3 (bIntercept = 5.55, SE = 2.70, p = .04) and an acceleration in the increasing probability of smoking across the week (bQuadratic = 0.19, SE = 0.05, p < .001).
PA
Higher pre-quit PA predicted a steeper increase in the probability of smoking across the week (bLinear = 0.11, SE = 0.05, p = .03), while higher TQD PA predicted lower smoking rates at Day 3 (bIntercept = −2.91, SE = 1.41, p = .04) and a less steep increase in the probability of smoking across the week (bLinear = −0.13, SE = 0.05, p = .01).
Additional models examined the effect of growth model parameters on NA and PA at 1 week post quit (Section S1).
Discussion
This study addresses the call to expand the assessment of clinical outcomes in tobacco cessation clinical trials beyond dichotomous smoking abstinence^5^ by conducting preliminary two-part LGMs to evaluate treatment effects and predictors of outcomes on both smoking probability and smoking rate. Less than half of the sample (46%) self-reported smoking on the TQD, which increased and then stabilized around 50% by the middle of the week. Among those who continued smoking, CPD reduced to approximately a quarter of baseline rates and remained stable over the week. While light use (1–4 CPD) is related to smoking-associated illnesses, there is a dose–response relationship between smoking rate and health outcomes.^16^ Further, light smoking is associated with future cessation; therefore, reduction may be an important step towards abstinence.^2^
This study provides novel insights into smoking occurring early into the quit attempt. Using 7-day point prevalence abstinence at 1-week post-quit, this study found the majority of participants lapsed (69% for the varenicline and 84% placebo group, respectively). However, the present results detail that day-to-day nearly half of participants self-reported abstinence and, among those reporting smoking, CPD was greatly reduced. These data suggest day-level factors, including craving and affect, influence short-term abstinence and reduced smoking rate, which may inform strategies for re-initiating abstinence (eg, identification/avoidance of high craving contexts).
Consistent with prior work,^3^ varenicline treatment was associated with a higher probability of smoking abstinence; however, smoking rates were similar between the treatment groups. Further, varenicline did not significantly influence trajectories of smoking behavior over the first week of the quit attempt. Effects may have been attenuated since smoking was assessed retrospectively and was not bio-verified. Varenicline has been shown to increase time to first lapse,^17^ but relying on self-reported smoking may have attenuated treatment effects on smoking probability trajectories within this study. Future work will face challenges with bioverification (eg, carbon monoxide) since most are not suitable for evaluating differences in the smoking rate, although novel methods (eg, nicotine metabolite panels) may have potential.^18^
Focusing on the first week of the quit attempt may have further obfuscated changes in smoking behavior and treatment effects. While early lapses are predictive of relapse, time to relapse after a lapse event is variable with relapse risk peaking 5–10 days post-TQD.^19^ Longer time intervals would allow for the identification of high lapse risk periods and variables associated with long-term maintenance of reduced smoking rates. Although one solution is to include more timepoints, increased computational demand may prevent model estimation, especially when multiple predictors and/or nonlinear changes are included.^20^ Model development decisions (eg, timeframes, predictors) should occur a priori. Although there was little change in smoking trajectories, there was significant variability, suggesting key individual differences may contribute to changes in smoking behavior. Future work utilizing this approach can evaluate participant factors (eg, cigarette availability, cue exposure) that contribute to differences in smoking trajectories.
In addition to treatment effects, common mediators of varenicline efficacy^12^ predicted smoking probability and smoking rate. Higher pre-quit craving was associated with less change in smoking probability, while those experiencing higher cravings on the TQD were more likely to smoke and report higher smoking rates. Individuals experiencing a consistently high craving, both pre- and post-quit, may have been more likely to maintain daily smoking, resulting in less change in smoking probability, higher smoking probabilities, and higher smoking rates. The increasing probability of smoking throughout the week was accelerated with higher NA and lower PA, suggesting a more rapid return to daily smoking. Further, those experiencing more NA and less PA on the TQD reported higher smoking rates. Unexpectedly, higher PA prior to the quit attempt was associated with increased smoking probability over time. Prior work suggests situations associated with higher PA (eg, social alcohol use) contribute to relapse and being in these situations more often (across pre- and post-quit) may increase the likelihood of smoking.^21^ However, elucidating such daily dynamics requires frequent assessments (eg, ecological momentary assessment) and momentary modeling (eg, dynamic structural equation models).
This work demonstrates the utility of two-part LGM to examine daily smoking probability and rates within a smoking cessation clinical trial and provides a preliminary evaluation of the effects of varenicline on smoking abstinence and rate following the call by The Society for Research on Nicotine and Tobacco.^5^ Varenicline reduced the probability of smoking but was largely unrelated to smoking rates and daily changes in smoking behavior early into the quit attempt. Craving and affect may be barriers to both smoking abstinence and rate. Future work can leverage information about barriers to smoking abstinence and reduction to improve outcomes.
Supplementary Material
ntaf095_suppl_Supplementary_Material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adams JM. Smoking cessation-progress, barriers, and new opportunities: the surgeon general’s report on smoking cessation. JAMA. 2020;323(24):2470–2471. doi: https://doi.org/10.1001/jama.2020.664732432659 · doi ↗ · pubmed ↗
- 2Hughes JR, Carpenter MJ. Does smoking reduction increase future cessation and decrease disease risk? A qualitative review. Nicotine Tob Res. 2006;8(6):739–749. doi: https://doi.org/10.1080/1462220060078972617132521 · doi ↗ · pubmed ↗
- 3Ebbert JO, Hughes JR, West RJ, et al Effect of varenicline on smoking cessation through smoking reduction: a randomized clinical trial. JAMA. 2015;313(7):687–694. doi: https://doi.org/10.1001/jama.2015.28025688780 PMC 4883651 · doi ↗ · pubmed ↗
- 4Wennike P, Danielsson T, Landfeldt B, Westin A, Tønnesen P. Smoking reduction promotes smoking cessation: results from a double blind, randomized, placebo‐controlled trial of nicotine gum with 2‐year follow‐up. Addiction. 2003;98(10):1395–1402.14519176 10.1046/j.1360-0443.2003.00489.x · doi ↗ · pubmed ↗
- 5Kypriotakis G, Bernstein SL, Bold KW, et al An introduction and practical guide to strategies for analyzing longitudinal data in clinical trials of smoking cessation treatment: beyond dichotomous point-prevalence outcomes. Nicotine Tob Res. 2024;26(7):796–805. doi: https://doi.org/10.1093/ntr/ntae 00538214037 PMC 11190044 · doi ↗ · pubmed ↗
- 6Conklin CA, Perkins KA, Sheidow AJ, et al The return to smoking: 1-year relapse trajectories among female smokers. Nicotine Tob Res. 2005;7(4):533–540. doi: https://doi.org/10.1080/1462220050018537116085524 · doi ↗ · pubmed ↗
- 7Olsen MK, Schafer JL. A Two-Part Random-Effects Model for semicontinuous longitudinal data. J Am Stat Assoc. 2001;96(454):730–745. doi: https://doi.org/10.1198/016214501753168389 · doi ↗
- 8Lerman C, Schnoll RA, Hawk LW, Jr, et al; PGRN-PNAT Research Group. Use of the nicotine metabolite ratio as a genetically informed biomarker of response to nicotine patch or varenicline for smoking cessation: a randomised, double-blind placebo-controlled trial. Lancet Respir Med. 2015;3(2):131–138. doi: https://doi.org/10.1016/S 2213-2600(14)70294-225588294 PMC 4480925 · doi ↗ · pubmed ↗