Congenital Knee Dislocation: A Rare Orthopedic Enigma in Rural Nepal
Rupak Kandel, Asmita Khanal, Anita Dahal, Bibek Panthee

TL;DR
A rare case of congenital knee dislocation in a Nepali newborn was successfully treated with early conservative methods, showing good long-term results.
Contribution
Demonstrates successful conservative management of CKD in a rural, resource-limited setting with long-term follow-up.
Findings
Bilateral knee dislocation improved with serial casting to 30° flexion within four weeks.
Normal knee alignment and motor milestones were maintained at four-year follow-up.
Conservative treatment can achieve excellent outcomes in CKD without surgical intervention.
Abstract
Congenital knee dislocation (CKD) (genu recurvatum congenitum) is a rare neonatal orthopedic deformity characterized by hyperextension of the knee joint and potentially associated with intrauterine mechanical factors, quadriceps contracture, or syndromic disorders. Early recognition is essential, as prompt conservative management can prevent long-term disability and reduce the need for surgical intervention. The objective of this single case report is to describe a rare presentation of bilateral congenital knee dislocation managed successfully through early conservative treatment in a rural and resource-limited setting of Nepal, highlighting the timeline of improvement and long-term outcome. We report a full-term female neonate born via institutional delivery in a remote region of Dailekh District, Nepal, who presented within 24 hours of birth with bilateral knee hyperextension of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1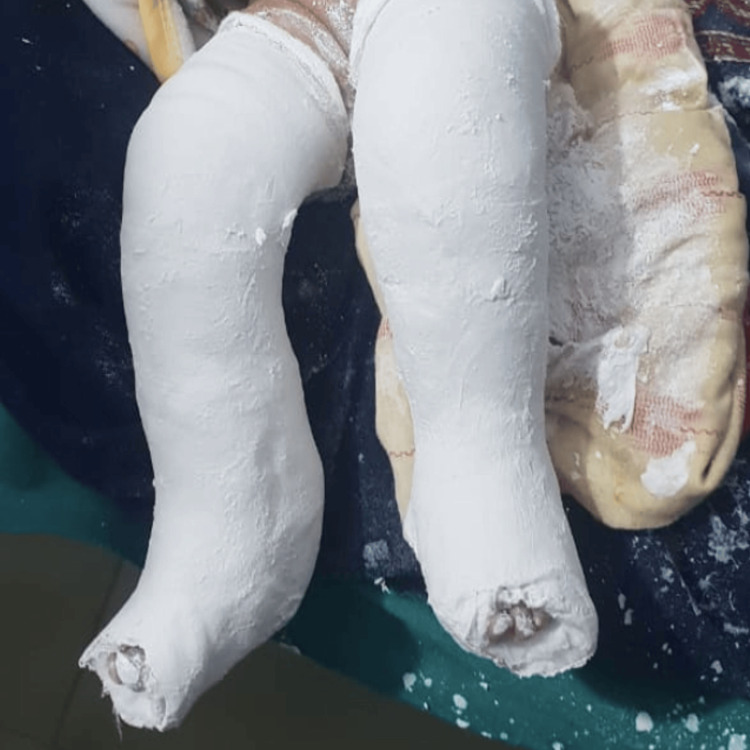 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4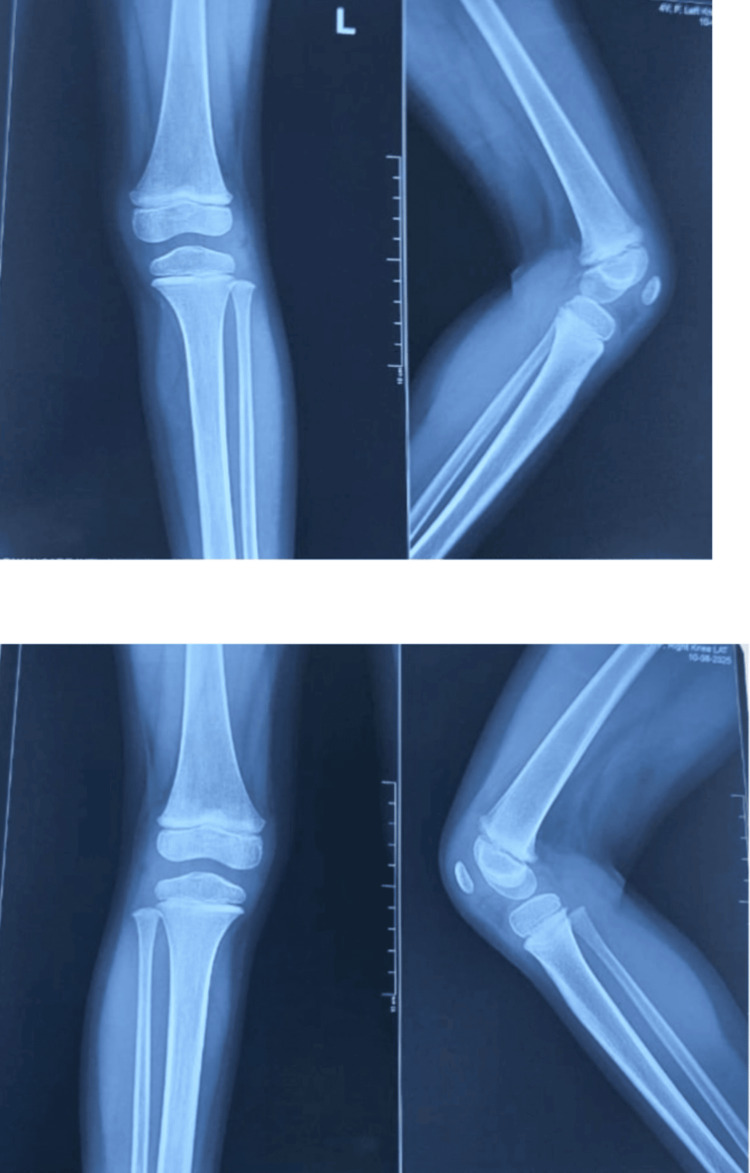 Figure 5
Figure 5 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurogenetic and Muscular Disorders Research · Immunodeficiency and Autoimmune Disorders · Orthopedic Infections and Treatments
Introduction
Congenital knee dislocation (CKD), often referred to as genu recurvatum congenitum, is a concerning and surprising discovery at birth. In the 1960s, it was agreed that the term congenital knee dislocation, which is defined by the forward displacement of the proximal tibia on the femoral condyles, encompassed all hyperextended knees present at birth [1]. It is a rare condition, occurring in approximately one in 100,000 live births, with an incidence of around 1% of congenital hip dislocation. It is more commonly seen in females than in males [1,2]. The diagnosis is typically made at birth through clinical observation of abnormal hyperextension of the knee joint [3].
The exact etiology and pathophysiology of congenital knee dislocation (genu recurvatum) remain unclear; however, several contributing factors have been proposed. These include intrauterine mechanical influences such as oligohydramnios, uterine abnormalities, and fetal malpositioning, particularly breech presentation, as well as maternal trauma, limited intrauterine space, quadriceps contracture or fibrosis, absence of the suprapatellar pouch, and hypoplasia or deficiency of the anterior cruciate ligament [4,5]. Histological investigations have revealed fibrotic alterations in the anterior joint capsule and quadriceps tendon, corroborating the idea that soft tissue disease plays a role in joint malalignment [6].
Clinically, congenital knee dislocation usually manifests at birth as a stiff, hyperextended knee that is resistant to passive flexion. It is divided into three classes according to its severity: grade I is hyperextension without subluxation, grade II is anterior tibial subluxation, and grade III is total dislocation. Early identification is essential since conservative therapy, such as periodic casting and gentle manipulation, can usually produce great results when started promptly. Surgical procedures, such as femoral osteotomy, anterior capsule release, or quadriceps lengthening, may be required if conservative therapy is delayed or fails [7-10]. Therefore, it is essential to screen affected patients for associated anomalies.
Through this case report, we aim to raise awareness among clinicians about bilateral congenital knee dislocation, a rare congenital condition, and to strengthen their confidence in counseling parents regarding treatment options and long-term outcomes. This four-year follow-up case is particularly significant because it was managed successfully in a rural, resource-limited setting where access to specialized orthopedic care and advanced imaging is scarce. It demonstrates that early diagnosis and timely conservative management can yield excellent functional recovery and long-term stability, even in challenging healthcare environments, thereby addressing a gap in existing literature on outcomes from such settings.
Case presentation
This case involved a full-term neonate diagnosed with type II congenital knee dislocation, presenting with severe bilateral knee hyperextension at birth. The case was identified in Dailekh District, a remote region of Nepal. The neonate received early conservative management, including gentle manipulation and serial above-knee casting.
A full-term female neonate was delivered via spontaneous vaginal delivery, with the mother having received regular antenatal care and an uneventful delivery. At birth, the neonate transitioned well with no systemic complications; however, physical examination revealed severe bilateral knee hyperextension of approximately 100°, consistent with type II congenital knee dislocation (Figure 1).
Clinical image showing congenital knee dislocation at birth
Initial gentle manipulation achieved partial reduction, but sustained flexion could not be maintained, indicating persistent joint instability. Early conservative management was initiated at a regional medical facility under orthopedic supervision, using serial above-knee plaster casting with casts changed at regular intervals to gradually increase knee flexion from 0° to 30°, while the toes were left exposed to monitor circulation and swelling. This approach was selected due to the remote location of the patient’s family, which limited access to frequent hospital follow-up (Figure 2).
Post-reduction casting in bilateral congenital knee dislocation
Over the course of the treatment, the hyperextension deformity improved markedly, and at cast removal, both knees rested in a near-neutral to mildly flexed position, demonstrating improved alignment and stability, with intact skin and no pressure sores or other complications. The feet maintained normal alignment, confirming the absence of secondary deformities (Figure 3).
Lower limbs of the neonate following plaster cast removal for type II bilateral congenital knee dislocation
Follow-up radiographs obtained on March 10, 2023, approximately one and a half years after the initial assessment on October 14, 2021, demonstrated well-aligned femorotibial articulations with preserved bony morphology and joint spaces, without subluxation, deformity, or growth plate abnormalities, confirming excellent medium-term outcomes (Figure 4).
Anteroposterior and lateral radiographs of the right and left knee at two years of age
Subsequent radiographs, including the last one obtained in August 2025, approximately four years after the initial case on October 14, 2021, demonstrated stable knee alignment, normal joint congruency, and intact epiphyseal plates, with no evidence of recurrent dislocation, deformity, or degenerative changes, confirming long-term joint stability (Figure 5).
Follow-up radiographs at four years showing well-aligned knees with normal joint congruency and intact growth plates
At the most recent clinical evaluation, the child’s lower limbs appeared normal, with proper knee alignment and no residual hyperextension or deformity, demonstrating complete recovery and highlighting the efficacy of early diagnosis, gentle manipulation, and serial casting in achieving excellent long-term outcomes for congenital knee dislocation, even in resource-limited settings (Figure 6).
Clinical appearance of the child’s lower limbs at follow-up, showing well-aligned knees in a normal position
This four-year follow-up report demonstrates the effectiveness of early conservative management in achieving complete anatomical and functional recovery in a resource-limited setting during the COVID-19 pandemic. Serial casting improved knee flexion from 0° to 30° within six weeks. No syndromic or systemic abnormalities were detected, and growth and developmental assessments confirmed normal milestone attainment. Comparative pre- and post-treatment details have been incorporated into the figures for greater clarity and clinical relevance.
Discussion
Congenital knee dislocation (CKD) is a rare limb malformation, usually noticeable at birth. Initial clinical evaluation should focus on assessing the extent of knee hyperextension, identifying anterior skin creases, and determining the reducibility of the dislocation. These characteristics are crucial for guiding treatment decisions and predicting outcomes [1]. Plain radiographs, including lateral and anteroposterior views of the knee, remain the preferred diagnostic modality. They help confirm the diagnosis by showing anterior displacement of the proximal tibia relative to the femoral condyles and can detect associated fractures or bony abnormalities [2].
CKD may present as an isolated condition or as part of a broader set of skeletal abnormalities. Mechanical (extrinsic) factors contributing to CKD include congenital absence of the cruciate ligaments, quadriceps fibrosis, or intrauterine positional issues such as prolonged extended breech positioning [3]. CKD may also be associated with intrinsic or genetic disorders, including Larsen syndrome, Desbuquois syndrome, Collins-Pope syndrome, Marfan syndrome, Down syndrome, Ehlers-Danlos syndrome, and Golgi-resident 3'-phosphoadenosine-5'-phosphate phosphatase (GPAPP) deficiency [4-6]. In this case, maternal and neonatal evaluations did not reveal any syndromic or genetic abnormalities, suggesting a mechanical etiology likely related to intrauterine positional factors.
In the present case, early diagnosis facilitated prompt initiation of conservative management through gentle manipulation and serial casting. This approach resulted in excellent functional and radiological outcomes, supporting existing literature that early intervention can often prevent the need for surgical correction [7,8]. Although initial radiographs were lost due to technical issues, follow-up clinical examinations and imaging at two and four years demonstrated normal femorotibial alignment with no evidence of recurrent dislocation, joint instability, or growth plate abnormality. After treatment, the child began walking at the normal developmental age of one year and, by four years, was able to walk and run independently without assistance, achieving age-appropriate gross motor milestones and remaining asymptomatic.
This case reinforces that early recognition and conservative management of CKD can achieve optimal outcomes, even in resource-limited settings. Continuous follow-up and community education are essential to ensure adherence to treatment protocols and to dispel misconceptions regarding the management of rare congenital conditions [9,10].
Conclusions
Congenital knee dislocation (CKD) is a rare but correctable neonatal orthopedic condition. Early diagnosis and prompt initiation of conservative treatment, such as gentle manipulation and serial casting, can result in excellent functional and radiological outcomes, even in resource-limited settings. In this single case, timely intervention allowed the child to achieve normal growth and development without long-term complications, avoiding the need for surgical correction. However, these findings may not be generalizable to all CKD cases, particularly those associated with syndromic or severe presentations.
Equally important is the parental experience, which highlights the emotional impact of such a diagnosis. The initial anxiety and uncertainty gradually transformed into relief and confidence as treatment progressed successfully. Over time, the positive outcome not only reassured the family but also helped raise awareness within the community that rare congenital conditions are treatable with appropriate care. This underscores the need for early recognition, parental counseling, and community education in managing rare congenital deformities such as CKD.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Congenital dislocation of the knee Acta Orthop Scand Jacobsen K Vopalecky F 17561985 https://www.tandfonline.com/doi/abs/10.3109/17453678508992968398469610.3109/17453678508992968 · doi ↗ · pubmed ↗
- 2Congenital dislocation of the knee at birth - part I: clinical signs and classification Orthop Traumatol Surg Res Mehrafshan M Wicart P Ramanoudjame M Seringe R Glorion C Rampal V 6316331022016 https://www.sciencedirect.com/science/article/pii/S 18770568163004572726661910.1016/j.otsr.2016.04.008 · doi ↗ · pubmed ↗
- 3Management of congenital dislocation of the knee J Pediatr Orthop Soc N Am Ellsworth BK Dawkins BJ Perea SH Green DW 27232021 https://www.jposna.com/article/S 2768-2765%2824%2900162-7/fulltext
- 4Unilateral congenital knee and hip dislocation with bilateral clubfoot - a rare packaging disorder J Orthop Case Reports Tiwari M Sharma N 212432013 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 4719237/2729890110.13107/jocr.2250-0685.096PMC 4719237 · doi ↗ · pubmed ↗
- 5Distal humeral fracture with associated triceps tendon avulsion in a renal transplant recipient Orthopedics Gupta RR Murthi AM 332010 https://journals.healio.com/doi/10.3928/01477447-20100129-2610.3928/01477447-20100129-2620349880 · doi ↗ · pubmed ↗
- 6Pediatric Orthopaedic Society of North America (POSNA): Congenital Knee Dislocation 8 2025 82025 https://posna.org/physician-education/study-guide/congenital-knee-dislocation
- 7Congenital snapping knee. Habitual anterior subluxation of the tibia in extension J Bone Joint Surg Br Ferris BD Jackson AM 453456721990 https://pubmed.ncbi.nlm.nih.gov/2341447234144710.1302/0301-620X.72B 3.2341447 · doi ↗ · pubmed ↗
- 8Chondrodysplasia and abnormal joint development associated with mutations in IMPAD 1, encoding the Golgi-resident nucleotide phosphatase, g PAPP Am J Hum Genet Vissers LE Lausch E Unger S 6086158820112154934010.1016/j.ajhg.2011.04.002PMC 3146727 · doi ↗ · pubmed ↗