Results from the Survey of Antibiotic Resistance (SOAR) 2018–21 in Pakistan: data based on CLSI, EUCAST (dose-specific) and pharmacokinetic/pharmacodynamic (PK/PD) breakpoints
Didem Torumkuney, Summiya Nizamuddin, Ian Morrissey, Rendani Manenzhe, Anand Manoharan

TL;DR
This study analyzed antibiotic resistance in bacteria causing respiratory infections in Pakistan and found that many antibiotics remain effective despite concerns about misuse.
Contribution
The study provides updated antibiotic susceptibility data using multiple breakpoints for S. pneumoniae and H. influenzae in Pakistan.
Findings
Most isolates showed good susceptibility to amoxicillin, ceftriaxone, and fluoroquinolones.
Cefdinir and cefaclor had lower activity, while tetracyclines and macrolides were poorly effective.
EUCAST high-dose breakpoints showed similar or lower susceptibility for some antibiotics compared to CLSI.
Abstract
To determine the antibiotic susceptibility of Streptococcus pneumoniae and Haemophilus influenzae isolates from community-acquired respiratory tract infections (CA-RTIs) collected in 2018–21 from Pakistan. MICs were determined by CLSI broth microdilution; susceptibility data were interpreted using CLSI, EUCAST and pharmacokinetic/pharmacodynamic (PK/PD) breakpoints. S. pneumoniae (n = 57) and H. influenzae (n = 67) were collected from the Shaukat Khanum Memorial Cancer Hospital and Research Centre, Lahore, Pakistan. The proportion of penicillin-susceptible pneumococci was 28.1% by CLSI oral/EUCAST low-dose breakpoints; 98.3%/98.2% were susceptible by EUCAST high-dose/CLSI intravenous breakpoints. Good activity (≥93.0%) was observed using CLSI or PK/PD breakpoints for amoxicillin, amoxicillin/clavulanic acid, cefotaxime, cefpodoxime, ceftriaxone, cefuroxime, levofloxacin and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
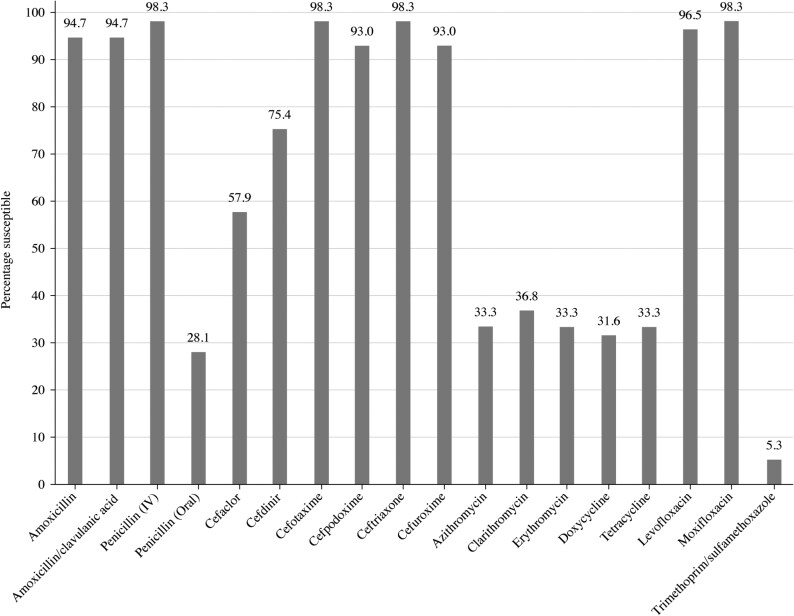 Figure 1
Figure 1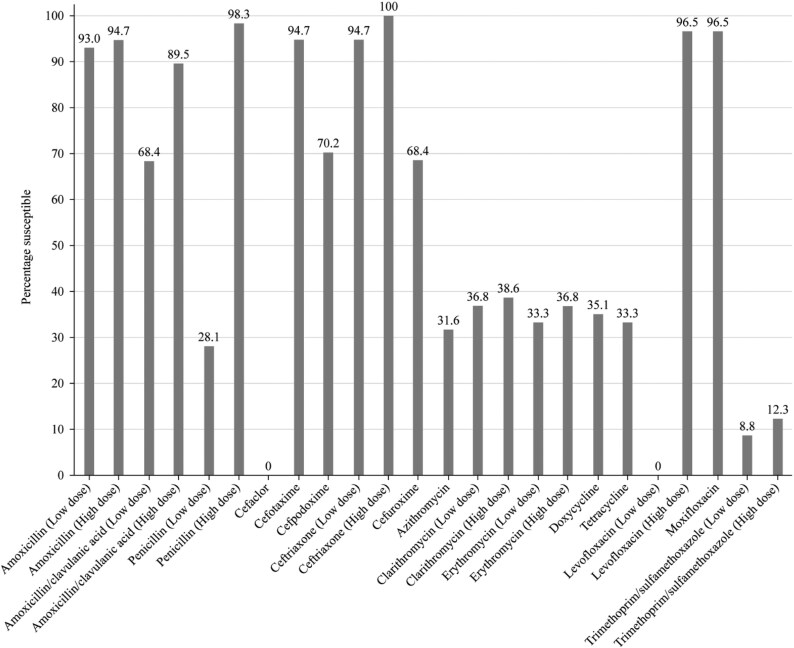 Figure 2
Figure 2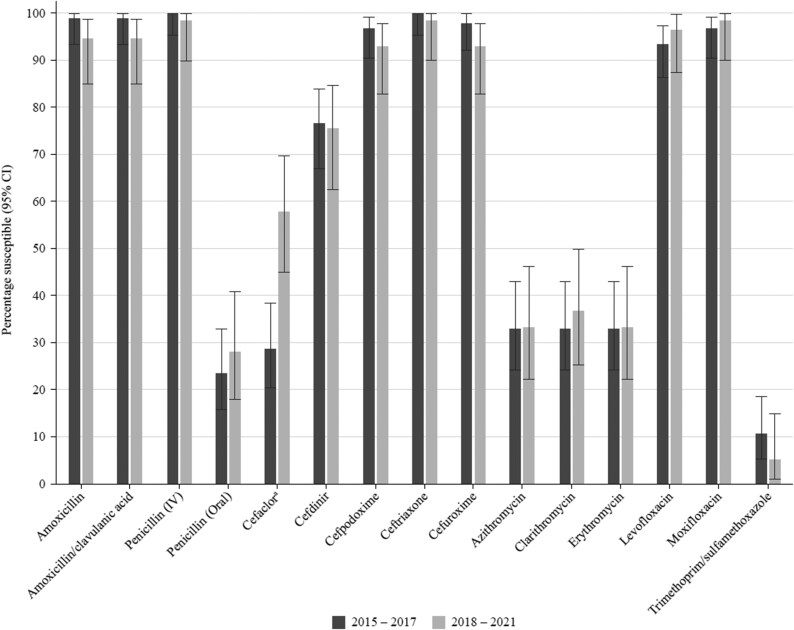 Figure 3
Figure 3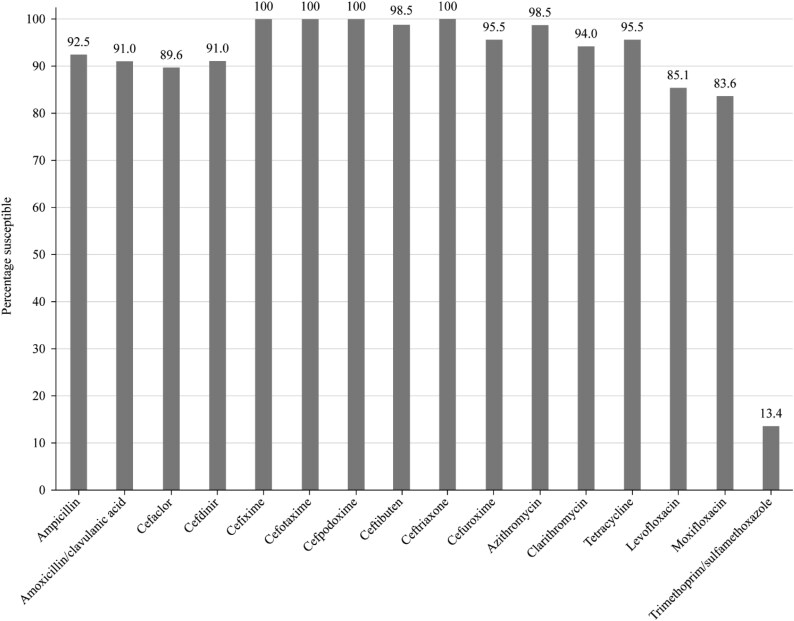 Figure 4
Figure 4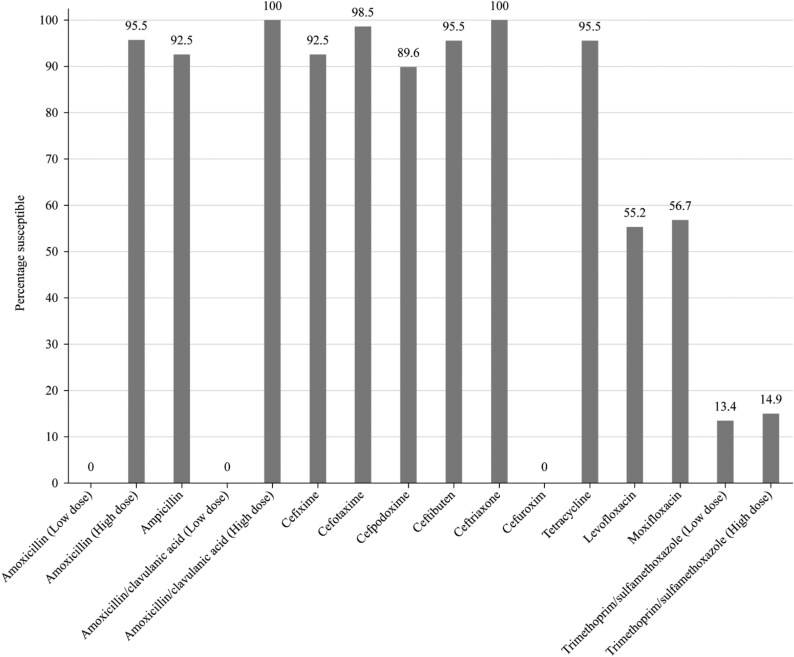 Figure 5
Figure 5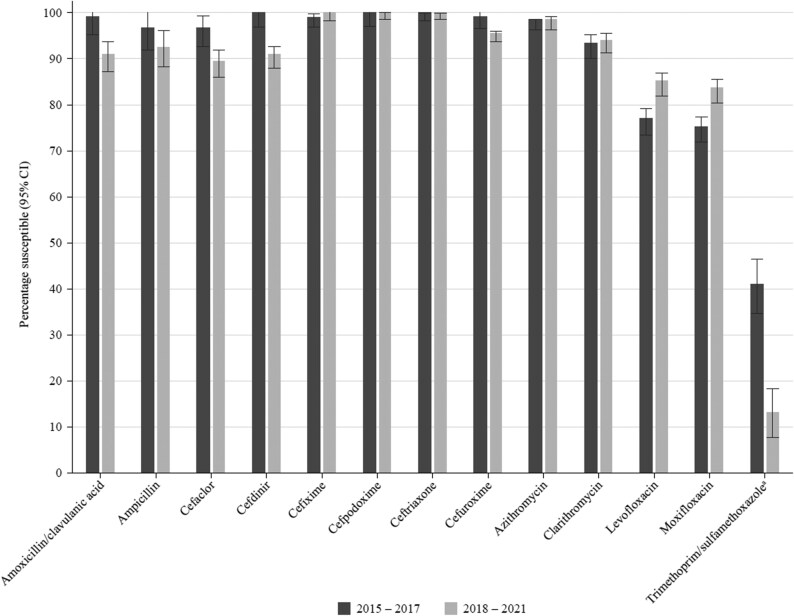 Figure 6
Figure 6|
|
| |||||
|---|---|---|---|---|---|---|
| Antimicrobial | S | I | R | S | I | R |
| Amoxicillin | ≤2 | 4 | ≥8 | — | — | — |
| Amoxicillin/clavulanic acid (2:1) | ≤2 | 4 | ≥8 | ≤2 | 4 | ≥8 |
| Ampicillin | NT | NT | NT | ≤1 | 2 | ≥4 |
| Azithromycin | ≤0.5 | 1 | ≥2 | ≤4 | — | — |
| Cefaclor | ≤1 | 2 | ≥4 | ≤8 | 16 | ≥32 |
| Cefdinir | ≤0.5 | 1 | ≥2 | ≤1 | — | — |
| Cefixime | — | — | — | ≤1 | — | — |
| Cefotaxime (non-meningitis) | ≤1 | 2 | ≥4 | ≤2 | — | — |
| Cefpodoxime | ≤0.5 | 1 | ≥2 | ≤2 | — | — |
| Ceftibuten | — | — | — | ≤2 | — | — |
| Ceftriaxone (non-meningitis) | ≤1 | 2 | ≥4 | ≤2 | — | — |
| Cefuroxime | ≤1 | 2 | ≥4 | ≤4 | 8 | ≥16 |
| Clarithromycin | ≤0.25 | 0.5 | ≥1 | ≤8 | 16 | ≥32 |
| Doxycycline | ≤0.25 | 0.5 | ≥1 | NT | NT | NT |
| Erythromycin | ≤0.25 | 0.5 | ≥1 | NT | NT | NT |
| Levofloxacin | ≤2 | 4 | ≥8 | ≤2 | — | — |
| Moxifloxacin | ≤1 | 2 | ≥4 | ≤1 | — | — |
| Penicillin (2.4 g 2 MU × 4–6 IV) | ≤2 | 4 | ≥8 | NT | NT | NT |
| Penicillin (oral) | ≤0.06 | 0.12–1 | ≥2 | NT | NT | NT |
| Tetracycline | ≤1 | 2 | ≥4 | ≤2 | 4 | ≥8 |
| Trimethoprim/sulfamethoxazole | ≤0.5 | 1–2 | ≥4 | ≤0.5 | 1–2 | ≥4 |
|
|
| |||
|---|---|---|---|---|
| Antimicrobial | S | R | S | R |
| Amoxicillin (0.5 g × 3 oral) | ≤0.5 | >1 | ≤0.001 | >2 |
| Amoxicillin (0.75–1 g × 3 oral) | ≤1 | >1 | ≤2 | >2 |
| Amoxicillin/clavulanic acid (0.5 g/0.125 g × 3 oral) | ≤0.5 | >1 | ≤0.001 | >2 |
| Amoxicillin/clavulanic acid (0.875 g/0.125 g × 3 oral) | ≤1 | >1 | ≤2 | >2 |
| Ampicillin (2 g × 3 IV) | NT | NT | ≤1 | >1 |
| Ampicillin (2 g × 4 IV) | NT | NT | ≤1 | >1 |
| Azithromycin | ≤0.25 | >0.5 | — | — |
| Cefaclor | ≤0.001 | >0.5 | — | — |
| Cefdinir | — | — | — | — |
| Cefixime | — | — | ≤0.12 | >0.12 |
| Cefotaxime | ≤0.5 | >2 | ≤0.12 | >0.12 |
| Cefpodoxime | ≤0.25 | >0.5 | ≤0.25 | >0.25 |
| Ceftibuten | — | — | ≤1 | >1 |
| Ceftriaxone (1 g × 1 IV) | ≤0.5 | >2 | ≤0.12 | >0.12 |
| Ceftriaxone (2 g × 2 IV) | ≤2 | >2 | ≤0.12 | >0.12 |
| Cefuroxime | ≤0.25 | >0.5 | ≤0.001 | >1 |
| Clarithromycin (0.25 g × 2 oral) | ≤0.25 | >0.5 | — | — |
| Clarithromycin (0.5 g × 2 oral) | ≤0.5 | >0.5 | — | — |
| Doxycycline | ≤1 | >2 | NT | NT |
| Erythromycin (0.5 g × 2–4 oral or 0.5 g × 2–4 IV) | ≤0.25 | >0.5 | NT | NT |
| Erythromycin (1 g × 4 oral or 1 g × 4 IV) | ≤0.5 | >0.5 | NT | NT |
| Levofloxacin (0.5 g × 2 oral or 0.4 g × 2 IV) | ≤0.001 | >2 | ≤0.06 | >0.06 |
| Levofloxacin (0.75 g × 2 oral or 0.4 g × 3 IV) | ≤2 | >2 | ≤0.06 | >0.06 |
| Moxifloxacin | ≤0.5 | >0.5 | ≤0.12 | >0.12 |
| Penicillin (0.6 g 1 MU × 4 IV) | ≤0.06 | >2 | NT | NT |
| Penicillin (2.4 g 2 MU × 4–6 IV) | ≤2 | >2 | NT | NT |
| Tetracycline | ≤1 | >2 | ≤2 | >2 |
| Trimethoprim/sulfamethoxazole (0.16 g/0.8 g × 2 oral or IV) | ≤1 | >2 | ≤0.5 | >1 |
| Trimethoprim/sulfamethoxazole (0.24 g/1.2 g × 2 oral or IV) | ≤2 | >2 | ≤1 | >1 |
|
| |
|---|---|
| Antimicrobial | S only |
| Amoxicillin (1.5 g/day) | ≤2 |
| Amoxicillin (4 g/day) | ≤4 |
| Amoxicillin/clavulanic acid | ≤2 |
| Amoxicillin/clavulanic acid | ≤4 |
| Ampicillin | — |
| Penicillin | — |
| Cefaclor | ≤0.5 |
| Cefdinir | ≤0.25 |
| Cefditoren | — |
| Cefixime | ≤1 |
| Cefpodoxime | ≤0.5 |
| Ceftriaxone | ≤1 |
| Cefuroxime | ≤1 |
| Azithromycin | ≤0.12 |
| Clarithromycin | ≤0.25 |
| Erythromycin | ≤0.25 |
| Levofloxacin | ≤2 |
| Moxifloxacin | ≤1 |
| Trimethoprim/sulfamethoxazole | ≤0.5 |
| MIC (mg/L) | CLSI susceptibility | |||||
|---|---|---|---|---|---|---|
| Antimicrobial | Range | 50% | 90% | %S | %I | %R |
| Amoxicillin | ≤0.008–4 | 0.12 | 0.5 | 94.7 | 5.3 | 0 |
| Amoxicillin/clavulanic acid (2:1) | ≤0.008–8 | 0.12 | 0.5 | 94.7 | 3.5 | 1.8 |
| Penicillin (2.4 g 2 MU × 4–6 IV) | ≤0.008–4 | 0.12 | 0.5 | 98.2 | 1.8 | 0 |
| Penicillin (oral) | ≤0.008–4 | 0.12 | 0.5 | 28.1 | 66.7 | 5.3 |
| Cefaclor | 0.06–>4 | 1 | >4 | 57.9 | 14.0 | 28.1 |
| Cefdinir | 0.03–8 | 0.25 | 1 | 75.4 | 17.5 | 7.0 |
| Cefixime | ≤0.25–>16 | 2 | 4 | — | — | — |
| Cefotaxime | ≤0.008–2 | 0.12 | 0.5 | 98.2 | 1.8 | 0 |
| Cefpodoxime | ≤0.015–4 | 0.25 | 0.5 | 93.0 | 1.8 | 5.3 |
| Ceftibuten | 1–>16 | 16 | >16 | — | — | — |
| Ceftriaxone | 0.015–2 | 0.25 | 0.5 | 98.2 | 1.8 | 0 |
| Cefuroxime | 0.015–8 | 0.25 | 0.5 | 93.0 | 1.8 | 5.3 |
| Azithromycin | ≤0.015–>16 | 2 | >16 | 33.3 | 5.3 | 61.4 |
| Clarithromycin | ≤0.015–>16 | 1 | >16 | 36.8 | 1.8 | 61.4 |
| Erythromycin | ≤0.015–>16 | 2 | >16 | 33.3 | 3.5 | 63.2 |
| Doxycycline | 0.03–>4 | 4 | >4 | 31.6 | 0 | 68.4 |
| Tetracycline | ≤0.03–>4 | >4 | >4 | 33.3 | 0 | 66.7 |
| Levofloxacin | ≤0.12–>8 | 1 | 1 | 96.5 | 0 | 3.5 |
| Moxifloxacin | ≤0.03–2 | 0.06 | 0.12 | 98.2 | 1.8 | 0 |
| Trimethoprim/sulfamethoxazole | ≤0.06–>8 | 4 | 8 | 5.3 | 7.0 | 87.7 |
| MIC (mg/L) | EUCAST susceptibility | |||||
|---|---|---|---|---|---|---|
| Antimicrobial | Range | 50% | 90% | %S | %I | %R |
| Amoxicillin (0.5 g × 3 oral) | ≤0.008–4 | 0.12 | 0.5 | 93.0 | 1.8 | 5.3 |
| Amoxicillin (0.75–1 g × 3 oral) | ≤0.008–4 | 0.12 | 0.5 | 94.7 | — | 5.3 |
| Amoxicillin/clavulanic acid (0.5 g/0.125 g × 3 oral) | ≤0.008–>8 | 0.5 | 2 | 68.4 | 21.1 | 10.5 |
| Amoxicillin/clavulanic acid (0.875 g/0.125 g × 3 oral) | ≤0.008–>8 | 0.5 | 2 | 89.5 | — | 10.5 |
| Penicillin (0.6 g 1 MU × 4 IV) | ≤0.008–4 | 0.12 | 0.5 | 28.1 | 70.2 | 1.8 |
| Penicillin (2.4 g 2 MU × 4–6 IV) | ≤0.008–4 | 0.12 | 0.5 | 98.3 | — | 1.8 |
| Cefaclor | 0.06–>4 | 1 | >4 | 0 | 19.3 | 80.7 |
| Cefdinir | 0.03–8 | 0.25 | 1 | — | — | — |
| Cefixime | ≤0.25–>16 | 2 | 4 | — | — | — |
| Cefotaxime | ≤0.008–2 | 0.12 | 0.5 | 94.7 | 5.3 | 0 |
| Cefpodoxime | ≤0.015–4 | 0.25 | 0.5 | 70.2 | 22.8 | 7.0 |
| Ceftibuten | 1–>16 | 16 | >16 | — | — | — |
| Ceftriaxone (1 g × 1 IV) | 0.015–2 | 0.25 | 0.5 | 94.7 | 5.3 | 0 |
| Ceftriaxone (2 g × 2 IV) | 0.015–2 | 0.25 | 0.5 | 100 | — | 0 |
| Cefuroxime | 0.015–8 | 0.25 | 0.5 | 68.4 | 22.8 | 8.8 |
| Azithromycin | ≤0.015–>16 | 2 | >16 | 31.6 | 1.8 | 66.7 |
| Clarithromycin (0.25 g × 2 oral) | ≤0.015–>16 | 1 | >16 | 36.8 | 1.8 | 61.4 |
| Clarithromycin (0.5 g × 2 oral) | ≤0.015–>16 | 1 | >16 | 38.6 | — | 61.4 |
| Erythromycin (0.5 g × 2–4 oral or 0.5 g × 2–4 IV) | ≤0.015–>16 | 2 | >16 | 33.3 | 3.5 | 63.2 |
| Erythromycin (1 g × 4 oral or 1 g × 4 IV) | ≤0.015–>16 | 2 | >16 | 36.8 | — | 63.2 |
| Doxycycline | 0.03–>4 | 4 | >4 | 35.1 | 10.5 | 54.4 |
| Tetracycline | ≤0.03–>4 | >4 | >4 | 33.3 | 0 | 66.7 |
| Levofloxacin (0.5 g × 2 oral or 0.4 g × 2 IV) | ≤0.12–>8 | 1 | 1 | 0 | 96.5 | 3.5 |
| Levofloxacin (0.75 g × 2 oral or 0.4 g × 3 IV) | ≤0.12–>8 | 1 | 1 | 96.5 | — | 3.5 |
| Moxifloxacin | ≤0.03–2 | 0.06 | 0.12 | 96.5 | — | 3.5 |
| Trimethoprim/sulfamethoxazole (0.16 g/0.8 g × 2 oral or IV) | ≤0.06–>8 | 4 | 8 | 8.8 | 3.5 | 87.7 |
| Trimethoprim/sulfamethoxazole (0.24 g/1.2 g × 2 oral or IV) | ≤0.06–>8 | 4 | 8 | 12.3 | — | 87.7 |
| MIC (mg/L) | PK/PD susceptibility | |||
|---|---|---|---|---|
| Antimicrobial | Range | 50% | 90% | %S |
| Amoxicillin (1.5 g/day) | ≤0.008–4 | 0.12 | 0.5 | 94.7 |
| Amoxicillin (4 g/day) | ≤0.008–4 | 0.12 | 0.5 | 100 |
| Amoxicillin/clavulanic acid (1.75 g/0.25 g/day adults; 45 mg/6.4 mg/kg/day children) | ≤0.008–8 | 0.12 | 0.5 | 94.7 |
| Amoxicillin/clavulanic acid (4 g/0.25 g/day adults; 90 mg/6.4 mg/kg/day children) | ≤0.008–8 | 0.12 | 0.5 | 98.2 |
| Penicillin | ≤0.008–4 | 0.12 | 0.5 | — |
| Cefaclor | 0.06–>4 | 1 | >4 | 19.3 |
| Cefdinir | 0.03–8 | 0.25 | 1 | 61.4 |
| Cefixime | ≤0.25–>16 | 2 | 4 | 45.6 |
| Cefotaxime | ≤0.008–2 | 0.12 | 0.5 | — |
| Cefpodoxime | ≤0.015–4 | 0.25 | 0.5 | 93.0 |
| Ceftibuten | 1–>16 | 16 | >16 | — |
| Ceftriaxone | 0.015–2 | 0.25 | 0.5 | 98.2 |
| Cefuroxime | 0.015–8 | 0.25 | 0.5 | 93.0 |
| Azithromycin | ≤0.015–>16 | 2 | >16 | 31.6 |
| Clarithromycin | ≤0.015–>16 | 1 | >16 | 36.8 |
| Erythromycin | ≤0.015–>16 | 2 | >16 | 33.3 |
| Doxycycline | 0.03–>4 | 4 | >4 | 31.6 |
| Tetracycline | ≤0.03–>4 | >4 | >4 | — |
| Levofloxacin | ≤0.12–>8 | 1 | 1 | 96.5 |
| Moxifloxacin | ≤0.03–2 | 0.06 | 0.12 | 98.2 |
| Trimethoprim/sulfamethoxazole | ≤0.06–>8 | 4 | 8 | 5.3 |
| MIC (mg/L) | CLSI susceptibility | |||||
|---|---|---|---|---|---|---|
| Antimicrobial | Range | 50% | 90% | %S | %I | %R |
| Amoxicillin | ≤0.03–128 | 0.5 | 2 | — | — | — |
| Ampicillin | ≤0.03–64 | 0.25 | 1 | 92.5 | 3.0 | 4.5 |
| Amoxicillin/clavulanic acid (2:1) | 0.12–4 | 0.5 | 2 | 91.1 | 9.0 | 0 |
| Cefaclor | ≤0.25–32 | 2 | 16 | 89.6 | 6.0 | 4.5 |
| Cefdinir | ≤0.06–2 | 0.25 | 1 | 91.0 | — | — |
| Cefixime | ≤0.008–1 | 0.03 | 0.12 | 100 | — | — |
| Cefotaxime | ≤0.002–0.25 | 0.008 | 0.12 | 100 | — | — |
| Cefpodoxime | ≤0.015–2 | 0.06 | 0.5 | 100 | — | — |
| Ceftibuten | 0.015–4 | 0.06 | 1 | 98.5 | — | — |
| Ceftriaxone | ≤0.001–0.06 | 0.004 | 0.03 | 100 | — | — |
| Cefuroxime | 0.06–16 | 0.5 | 4 | 95.5 | 1.5 | 3.0 |
| Azithromycin | ≤0.12–>8 | 0.5 | 2 | 98.5 | — | — |
| Clarithromycin | ≤0.25–>32 | 4 | 8 | 94.0 | 4.5 | 1.5 |
| Tetracycline | ≤0.12–16 | 0.25 | 0.5 | 95.5 | 0 | 4.5 |
| Levofloxacin | 0.008–>8 | 0.06 | >8 | 85.1 | — | — |
| Moxifloxacin | 0.008–>8 | 0.06 | 8 | 83.6 | — | — |
| Trimethoprim/sulfamethoxazole | ≤0.008–>8 | 8 | >8 | 13.4 | 1.5 | 85.1 |
| MIC (mg/L) | EUCAST susceptibility | |||||
|---|---|---|---|---|---|---|
| Antimicrobial | Range | 50% | 90% | %S | %I | %R |
| Amoxicillin (0.5 g × 3 oral) | ≤0.03–128 | 0.5 | 2 | 0 | 95.5 | 4.5 |
| Amoxicillin (0.75–1 g × 3 oral) | ≤0.03–128 | 0.5 | 2 | 95.5 | — | 4.5 |
| Ampicillin | ≤0.03–64 | 0.25 | 1 | 92.5 | — | 7.5 |
| Amoxicillin/clavulanic acid (0.5 g/0.125 g × 3 oral) | ≤0.03–2 | 0.25 | 2 | 0 | 100 | 0 |
| Amoxicillin/clavulanic acid (0.875 g/0.125 g × 3 oral) | ≤0.03–2 | 0.25 | 2 | 100 | — | 0 |
| Cefaclor | ≤0.25–32 | 2 | 16 | — | — | — |
| Cefdinir | ≤0.06–2 | 0.25 | 1 | — | — | — |
| Cefixime | ≤0.008–1 | 0.03 | 0.12 | 92.5 | — | 7.5 |
| Cefotaxime | ≤0.002–0.25 | 0.008 | 0.12 | 98.5 | — | 1.5 |
| Cefpodoxime | ≤0.015–2 | 0.06 | 0.5 | 89.6 | — | 10.4 |
| Ceftibuten | 0.015–4 | 0.06 | 1 | 95.5 | — | 4.5 |
| Ceftriaxone | ≤0.001–0.06 | 0.004 | 0.03 | 100 | — | 0 |
| Cefuroxime | 0.06–16 | 0.5 | 4 | 0 | 67.2 | 32.8 |
| Azithromycin | ≤0.12–>8 | 0.5 | 2 | — | — | — |
| Clarithromycin | ≤0.25–>32 | 4 | 8 | — | — | — |
| Tetracycline | ≤0.12–16 | 0.25 | 0.5 | 95.5 | — | 4.5 |
| Levofloxacin | 0.008–>8 | 0.06 | >8 | 55.2 | — | 44.8 |
| Moxifloxacin | 0.008–>8 | 0.06 | 8 | 56.7 | — | 43.3 |
| Trimethoprim/sulfamethoxazole (0.16 g/0.8 g × 2 oral or IV) | ≤0.008–>8 | 8 | >8 | 13.4 | 1.5 | 85.1 |
| Trimethoprim/sulfamethoxazole (0.24 g/1.2 g × 2 oral or IV) | ≤0.008–>8 | 8 | >8 | 14.9 | — | 85.1 |
| MIC (mg/L) | PK/PD susceptibility | |||
|---|---|---|---|---|
| Antimicrobial | Range | 50% | 90% | %S |
| Amoxicillin (1.5 g/day) | ≤0.03–128 | 0.5 | 2 | 95.5 |
| Amoxicillin (4 g/day) | ≤0.03–128 | 0.5 | 2 | 95.5 |
| Amoxicillin/clavulanic acid (1.75 g/0.25 g/day adults; 45 mg/6.4 mg/kg/day children) | ≤0.03–2 | 0.25 | 2 | 95.5 |
| Amoxicillin/clavulanic acid (4 g/0.25 g/day adults; 90 mg/6.4 mg/kg/day children) | ≤0.03–2 | 0.25 | 2 | 97.0 |
| Ampicillin | ≤0.03–64 | 0.25 | 1 | — |
| Cefaclor | ≤0.25–32 | 2 | 16 | 17.9 |
| Cefdinir | ≤0.06–2 | 0.25 | 1 | 68.7 |
| Cefixime | ≤0.008–1 | 0.03 | 0.12 | 100 |
| Cefotaxime | ≤0.002–0.25 | 0.008 | 0.12 | — |
| Cefpodoxime | ≤0.015–2 | 0.06 | 0.5 | 95.5 |
| Ceftibuten | 0.015–4 | 0.06 | 1 | — |
| Ceftriaxone | ≤0.001–0.06 | 0.004 | 0.03 | 100 |
| Cefuroxime | 0.06–16 | 0.5 | 4 | 67.2 |
| Azithromycin | ≤0.12–>8 | 0.5 | 2 | 4.5 |
| Clarithromycin | ≤0.25–>32 | 4 | 8 | 3.0 |
| Tetracycline | ≤0.12–16 | 0.25 | 0.5 | — |
| Levofloxacin | 0.008–>8 | 0.06 | >8 | 85.1 |
| Moxifloxacin | 0.008–>8 | 0.06 | 8 | 83.6 |
| Trimethoprim/sulfamethoxazole | ≤0.008–>8 | 8 | >8 | 13.4 |
- —GSK10.13039/501100002066
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Use and Resistance · Pneumonia and Respiratory Infections · Antibiotics Pharmacokinetics and Efficacy
Introduction
Community-acquired respiratory tract infections (CA-RTIs) are an important world health problem that, if treated inappropriately, or in patients with comorbidities, can result in hospitalization, with a third of patients with community-acquired pneumonia dying within 12 months after being discharged from hospital.^1^ However, age, comorbidities and other underlying risk factors may have influenced the observed mortality rate.^1^ Treatment of CA-RTIs is reliant on empiric antibiotic therapy through the use of national and international guidelines.^2^ Studies have shown that there is a high level of inappropriate antibiotic use in Pakistan, including sales without a prescription and self-medication,^3–5^ and this has been shown to be associated with the development of increasing antimicrobial resistance.^6^
Streptococcus pneumoniae and Haemophilus influenzae are the major bacteria associated with CA-RTIs.^7,8^ Both pathogens have shown increasing resistance to first-line antibiotics such as penicillin and ampicillin.^9,10^ As rates of resistance vary over time and from country to country, up-to-date surveillance data are essential to guide local antibiotic policies.^11^
The Survey of Antibiotic Resistance (SOAR), an international antibiotic resistance surveillance study, focuses on key respiratory pathogens that cause community-acquired infections and has been running since 2002 in the Middle East, Africa, Latin America, Asia-Pacific, Europe and the Commonwealth of Independent States countries.^12^ For this study, recent SOAR data from hospitals in Pakistan have been analysed to provide a picture of the current state of antibiotic susceptibility of S. pneumoniae and H. influenzae associated with CA-RTIs.
Materials and methods
Ethics
SOAR studies are not human subject studies. During the study, only microorganisms were examined.
Clinical isolates
Isolates of H. influenzae and S. pneumoniae from CA-RTIs (isolated within 48 h of hospitalization) were collected between 2018 and 2021 from the Shaukat Khanum Memorial Cancer Hospital, Lahore, Pakistan, and sent to a central laboratory (IHMA Europe, Monthey, Switzerland), where they were sub-cultured and re-identified. H. influenzae were re-identified by MALDI-TOF MS methodology, and S. pneumoniae identity was confirmed by optochin susceptibility and bile solubility. β-lactamase production was determined for each H. influenzae isolate by a chromogenic cephalosporin (nitrocefin) disc method. Duplicate isolates from the same patient were not accepted.
Susceptibility testing
Isolates were evaluated for antibiotic susceptibility using broth microdilution methodology recommended by CLSI.^13^ Amoxicillin, amoxicillin/clavulanic acid (2:1 ratio as per CLSI guidelines^13,14^), amoxicillin/clavulanic acid (fixed clavulanic acid at 2 mg/L as per EUCAST guidelines^15^), azithromycin, cefaclor, cefdinir, cefixime, cefotaxime, cefpodoxime, ceftibuten, ceftriaxone, cefuroxime, clarithromycin, levofloxacin, moxifloxacin, tetracycline and trimethoprim/sulfamethoxazole (1:19 ratio) were tested against both respiratory pathogens. In addition, doxycycline, erythromycin and penicillin were tested against S. pneumoniae only, and ampicillin was tested against H. influenzae only. Susceptibility to the study drugs was calculated based on CLSI, EUCAST (dose-specific) and pharmacokinetic/pharmacodynamic (PK/PD) breakpoints.^14–16^ These breakpoints are given in Tables 1–3. To fully assess antibiotics where high-dose therapies are available, susceptibility using EUCAST criteria was also calculated by combining percentage susceptible and susceptible, increased exposure into the susceptible category as well as dose-dependent PK/PD breakpoints.^15,16^ The antibiotics with high-dose availability assessed in this way were as follows: amoxicillin (0.75–1 g oral, 3× daily), amoxicillin/clavulanic acid (0.875 g amoxicillin/0.125 g clavulanic acid oral, 3× daily), ampicillin (2 g intravenous [IV], 4× daily), penicillin (2.4 g IV, 2 MU 4–6× daily), ceftriaxone (2 g IV, 2× daily), clarithromycin (0.5 g oral, 2× daily), erythromycin (1 g oral or IV, 4× daily), levofloxacin (0.75 g oral 2× daily or 0.4 g IV 3× daily) and trimethoprim/sulfamethoxazole (0.24 g trimethoprim/1.2 g sulfamethoxazole oral or IV, 2× daily).^15^
Quality control and data analysis
Quality control strains S. pneumoniae ATCC 49619, H. influenzae ATCC 49247, H. influenzae ATCC 49766 and E. coli ATCC 32518 were included on each day of testing. The results of susceptibility testing were only accepted if the results of the quality control strains were within the published acceptable range. Differences in susceptibility (using CLSI criteria) across penicillin-susceptible isolates (S. pneumoniae only) were assessed for statistical significance with Fisher's exact test using XLSTAT version 2023.1.1.1399. A P value <0.05 was considered statistically significant. A similar statistical analysis was performed to compare the susceptibility of isolates from 2018 to 2021 with Pakistan SOAR data from 2015 to 2017 (using CLSI criteria).^17^
Results
S. pneumoniae isolates
A total of 57 S. pneumoniae isolates were collected from the Shaukat Khanum Memorial Cancer Hospital between 2018 and 2021. Most isolates came from sputum (n = 21, 36.8%), blood (n = 19, 33.3%), bronchoalveolar lavage (n = 3, 5.3%) and endotracheal aspirate (n = 2, 3.5%). The remaining isolates were from unidentified specimens (n = 12, 21.1%). The majority of isolates (n = 39, 68.4%) came from adolescent and adult patients (aged 13–64 years), and 10 (17.5%) isolates were from elderly patients (aged ≥65 years) and 8 (14.0%) isolates from paediatric patients (aged ≤12 years).
Summary MIC, susceptibility, and MIC distribution data for all S. pneumoniae isolates are given in Tables 4–6 and S1 (available as Supplementary data at JAC Online) and shown in Figures 1 and 2.
Antibiotic susceptibility rates of S. pneumoniae isolates (n = 57) from Pakistan based on CLSI breakpoints.
Antibiotic susceptibility rates of S. pneumoniae isolates (n = 57) from Pakistan based on EUCAST (dose-specific) breakpoints.
S. pneumoniae susceptibility
The proportion of penicillin-susceptible pneumococci from Pakistan following CLSI oral or EUCAST low-dose IV breakpoints was 28.1% but increased to 98.3% and 98.2% with EUCAST high-dose and CLSI IV breakpoints, respectively. The rates of penicillin-intermediate and penicillin-resistant pneumococci using CLSI oral or EUCAST low-dose breakpoints were 66.7% and 5.3%, respectively. Following CLSI and PK/PD breakpoints, amoxicillin, amoxicillin/clavulanic acid, second-generation cephalosporins (cefpodoxime and cefuroxime) and third-generation cephalosporins (ceftriaxone and cefotaxime) showed similar activity with susceptibility ≥93.0%, but the second-generation and third-generation cephalosporins cefaclor and cefdinir were less active (57.9% and 75.4% susceptible, respectively, by CLSI and 19.3% and 61.4% susceptible, respectively, by PK/PD breakpoints). The use of EUCAST breakpoints produced similar susceptibility (≥89.5%) for amoxicillin and amoxicillin/clavulanic acid (high dose only), cefotaxime and ceftriaxone, but susceptibility to cefaclor (0%), cefpodoxime (70.2%) and cefuroxime (68.4%) was lower than that obtained with CLSI or PK/PD breakpoints. Poor activity (5.3%–38.6% susceptibility) was observed for the macrolides (azithromycin, clarithromycin and erythromycin), tetracyclines (doxycycline and tetracycline) and trimethoprim/sulfamethoxazole by CLSI, EUCAST and PK/PD interpretation. Moxifloxacin susceptibility was 96.5% by EUCAST and 98.2% by CLSI and PK/PD, and levofloxacin susceptibility was 96.5% by CLSI, PK/PD and EUCAST high dose (Tables 4–6 and Figures 1 and 2).
Comparative susceptibility of S. pneumoniae collected in 2015–17 and 2018–21
Data for the period 2015–17 have previously been published from the SOAR surveillance study and were compared for mutually tested antibiotics with the current study (2018–21) (Figure 3). There was no significant change in susceptibility except for an increased level of susceptibility to cefaclor (26.7% versus 57.9%). However, this improved activity would still be considered inadequate for therapeutic consideration.
Comparison of antibiotic susceptibility rates of S. pneumoniae isolates from Pakistan collected in 2015–17 with isolates collected in 2018–21 (CLSI breakpoints). aSusceptibility was significantly higher in 2018–21 than in 2015–17 (P = 0.0006).
H. influenzae isolates
A total of 67 H. influenzae isolates were collected from the Shaukat Khanum Memorial Cancer Hospital between 2018 and 2021. Most isolates originated from sputum (n = 44, 65.7%). The remaining isolates were from bronchoalveolar lavage (n = 4, 6.0%), endotracheal aspirate (n = 3, 4.5%), blood (n = 1, 1.5%), middle ear (n = 1, 1.5%) and unidentified specimens (n = 14, 20.9%). Most isolates (n = 44, 65.7%) came from adolescent and adult patients (aged 13–64 years), 17 (25.4%) isolates were from paediatric patients (aged ≤12 years), and six (9.0%) isolates were from elderly patients (aged ≥65 years).
Summary MIC, susceptibility and MIC distribution data for all 67 H. influenzae isolates are shown in Tables 7–9 and S2 and Figures 4 and 5.
Antibiotic susceptibility rates of H. influenzae isolates (n = 67) from Pakistan based on CLSI breakpoints.
Antibiotic susceptibility rates of H. influenzae isolates (n = 67) from Pakistan based on EUCAST (dose-specific) breakpoints.
H. influenzae susceptibility
Virtually all isolates of H. influenzae were β-lactamase negative (64/67, 95.5%). Within this population, two isolates were β-lactamase negative ampicillin-resistant (BLNAR) by EUCAST breakpoints (ampicillin MIC ≥2 mg/L) and none by CLSI breakpoints (ampicillin MIC ≥4 mg/L). Isolates from Pakistan test antibiotics were ≥83.6% susceptible to all antibiotics according to CLSI and PK/PD breakpoints, except for cefaclor (17.9% by PK/PD), cefdinir (68.7% by PK/PD), cefuroxime (67.2% by PK/PD), macrolides (azithromycin 4.5% and clarithromycin 3.0% by PK/PD) and trimethoprim/sulfamethoxazole (13.4% susceptible by CLSI and PK/PD). Similar results were obtained when using EUCAST breakpoints, provided high-dose regimens were used for amoxicillin and amoxicillin/clavulanate. Susceptibility rates of 0% and 55.2%/56.7% were found for cefuroxime and fluoroquinolone (levofloxacin/moxifloxacin), respectively, using EUCAST breakpoints (Tables 7–9 and Figures 4 and 5). Macrolide breakpoints are not provided by EUCAST against H. influenzae.
Comparative susceptibility of H. influenzae collected in 2015–17 and 2018–21
Generally, there was no significant change in susceptibility when comparing data from 2015 to 2017 with 2018–21 using CLSI breakpoints, with the exception of trimethoprim/sulfamethoxazole, where susceptibility significantly reduced since 2015–17 (Figure 6).
Comparison of antibiotic susceptibility rates of H. influenzae isolates from Pakistan collected in 2015–17 with isolates collected in 2018–21 (CLSI breakpoints). aSusceptibility was significantly lower in 2018–21 than in 2015–17 (P < 0.0001).
Discussion
SOAR is an ongoing global surveillance study focusing on the two main CA-RTIs pathogens, S. pneumoniae and H. influenzae, that has monitored numerous countries since 2002, including Pakistan. The data presented here are an analysis of the antibiotic susceptibility of S. pneumoniae and H. influenzae isolates collected from the Shaukat Khanum Memorial Cancer Hospital, Lahore, Pakistan, between 2018 and 2021. A potential limitation of this study is the national antibiotic resistance representation as the samples were collected from only one centre; however, as most isolates were from community-acquired infections and presumably unrelated, this is likely representative of the broader Pakistani community. This centre was one of two that participated in the previous SOAR surveillance from 2015 to 2017,^17^ and a direct statistical comparison between the two study periods is presented here.
The penicillin susceptibility results for S. pneumoniae in Pakistan from 2018 to 2021 confirm that oral penicillin or low-dose IV penicillin is not an appropriate therapy for CA-RTIs, as only 28.1% of pneumococci were susceptible using EUCAST low-dose IV or CLSI oral breakpoints. Although this shows a numerical increase compared with SOAR 2015–17 data (23.4% susceptible), the increase was not statistically significant.^17^ It is possible that susceptibility to oral penicillin reached a plateau after the decline since SOAR 2002–03, when oral penicillin susceptibility in Pakistan was 90.0%.^18,19^ Both CLSI and EUCAST guidelines, on the other hand, indicate that higher-dose IV penicillin is a superior option, with susceptibility at 98.3%. CLSI and PK/PD breakpoints indicate a comparably high level of susceptibility to amoxicillin, amoxicillin/clavulanic acid and cephalosporins (excluding cefaclor and cefdinir). Susceptibility using EUCAST breakpoints for most β-lactams was also in keeping with CLSI if high-dose amoxicillin/clavulanic acid was used. However, cefaclor, cefpodoxime and cefuroxime susceptibility was lower following EUCAST guidelines. Susceptibility according to either guideline indicated poor activity for macrolides, tetracyclines and trimethoprim/sulfamethoxazole, but good activity for fluoroquinolones against S. pneumoniae from Pakistan. Outside of the SOAR study, published antimicrobial susceptibility data for CA-RTI isolates from Pakistan are rare, but one recently published longitudinal study from 1993 to 2016 at a tertiary hospital in Karachi confirmed high resistance to trimethoprim/sulfamethoxazole over the whole period, and a trend of increased resistance to tetracycline and erythromycin, with low fluoroquinolone resistance in pneumococci.^20^ It is interesting that although the authors found no change in penicillin resistance for non- CSF isolates, there was a marked increase in penicillin resistance for CSF isolates of S. pneumoniae since 2008.
We compared the susceptibility of pneumococci using CLSI breakpoints for isolates previously collected in 2015–17 from Pakistan with susceptibility from the current study (2018–21). As noted above for oral penicillin, there was no significant difference in susceptibility between the two study periods, except for cefaclor, where susceptibility increased. Although this increase was statistically significant (P = 0.0006), the per cent susceptibility remained low.
All but three H. influenzae isolates from Pakistan were β-lactamase negative (95.5%), with two being BLNAR according to EUCAST breakpoints. Susceptibility to antibiotics was ≥83.6% by CLSI breakpoints, except for trimethoprim/sulfamethoxazole (13.4% susceptible). SOAR surveillance from 2002 to 2015 also indicated generally high antibiotic susceptibility with H. influenzae, except trimethoprim/sulfamethoxazole and chloramphenicol; the latter antibiotic was not tested in the current study.^18^ The only statistically significant difference between 2015–17 and 2018–21 susceptibility by CLSI breakpoints was a reduction in trimethoprim/sulfamethoxazole susceptibility. However, there were differences in susceptibility between CLSI and EUCAST in 2019–21 for cefuroxime (0% EUCAST susceptible versus 95.5% CLSI susceptible), macrolides (due to no EUCAST breakpoints given), levofloxacin (85.1% susceptible by CLSI versus 55.2% by EUCAST) and moxifloxacin (83.6% versus 56.7%). The lower fluoroquinolone susceptibility by EUCAST compared with CLSI was also observed in the previous SOAR surveillance for 2015–17 in Pakistan: levofloxacin (33.6% versus 77.1% susceptible) and moxifloxacin (34.4% versus 75.4% susceptible).^17^ Data from the ATLAS surveillance interactive database for H. influenzae collected from 2018 to 2021 and originating from 57 countries (3896 isolates in total) showed that levofloxacin susceptibility by EUCAST breakpoints was 95.2% overall.^21^ Therefore, the large difference in fluoroquinolone susceptibility between CLSI and EUCAST is unexpected. The ATLAS database for 2018–21 does not include Pakistan, but isolates from India were only 25% levofloxacin-susceptible by EUCAST breakpoints.^21^ The levofloxacin-resistant isolates by EUCAST breakpoints are so-called non-wild type, but most would still be considered susceptible by CLSI. It is possible, therefore, that dominant levofloxacin-non-wild-type (but levofloxacin-susceptible by CLSI breakpoints) isolates have been circulating in Asia since 2015.
In summary, although some resistance was observed, there are many suitable therapeutic options for the treatment of S. pneumoniae and H. influenzae originating from CA-RTIs in Pakistan despite some concerns about high levels of inappropriate antibiotic use in this country. Continued surveillance of antibiotic susceptibility in Pakistan is required to regularly assess any future changes.
Supplementary Material
dkaf288_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aliberti S, Dela Cruz CS, Amati F et al Community-acquired pneumonia. Lancet 2021; 398: 906–19. 10.1016/S 0140-6736(21)00630-934481570 · doi ↗ · pubmed ↗
- 2Cillóniz C, Dominedò C, Garcia-Vidal C et al Community-acquired pneumonia as an emergency condition. Curr Opin Crit Care 2018; 24: 531–9. 10.1097/MCC.000000000000055030239410 · doi ↗ · pubmed ↗
- 3Saleem Z, Hassali MA, Godman B et al Sale of WHO A Wa Re groups antibiotics without a prescription in Pakistan: a simulated client study. J Pharm Policy Pract 2020; 13: 26. 10.1186/s 40545-020-00233-332774870 PMC 7397594 · doi ↗ · pubmed ↗
- 4Saleem Z, Faller EM, Godman B et al Antibiotic consumption at community pharmacies: a multicenter repeated prevalence surveillance using WHO methodology. Med Access Point Care 2021; 5: 1–9. 10.1177/23992026211064714 PMC 941363736204499 · doi ↗ · pubmed ↗
- 5Dhedhi NA, Ashraf H, Ansari NB et al Self-medication among people visiting outpatient clinics of a tertiary care hospital, Karachi. J Family Med Prim Care 2021; 10: 773–9. 10.4103/jfmpc.jfmpc_1887_2034041075 PMC 8138398 · doi ↗ · pubmed ↗
- 6King LM, Fleming-Dutra KE, Hicks LA. Advances in optimizing the prescription of antibiotics in outpatient settings. BMJ 2018; 363; k 3047. 10.1136/bmj.k 304730420401 PMC 6511972 · doi ↗ · pubmed ↗
- 7Jain S, Self WH, Wunderink RG et al Community-acquired pneumonia requiring hospitalization among U.S. adults. N Engl J Med 2015; 373: 415–27. 10.1056/NEJ Moa 150024526172429 PMC 4728150 · doi ↗ · pubmed ↗
- 8Gadsby NJ, Russell CD, Mc Hugh MP et al Comprehensive molecular testing for respiratory pathogens in community-acquired pneumonia. Clin Infect Dis 2016; 62: 817–23. 10.1093/cid/civ 121426747825 PMC 4787606 · doi ↗ · pubmed ↗