Efficacy and safety of sorafenib combined with transarterial chemoembolization in the treatment of hepatocellular carcinoma: a meta-analysis of randomized controlled trials
Lixiu Yu, Yi Xiong, Jing Liao, Yahui Deng, Xuejia Zhai

TL;DR
This study finds that combining sorafenib with transarterial chemoembolization improves outcomes for hepatocellular carcinoma patients, though with increased side effects.
Contribution
A meta-analysis showing sorafenib plus TACE improves response rates and survival in hepatocellular carcinoma compared to TACE alone.
Findings
Combination therapy improved partial response rate and objective response rate in HCC patients.
Combination therapy significantly increased 12-month overall survival compared to TACE alone.
Combination therapy increased hand-foot skin reaction and abdominal pain or diarrhea side effects.
Abstract
Transarterial chemoembolization (TACE) plus sorafenib has led to an increase in randomized controlled trials The efficacy and safety of sorafenib combined with TACE for the treatment of hepatocellular carcinoma (HCC) remain controversial. We conducted a comprehensive meta-analysis of randomized controlled trials on this issue. A literature search was conducted by using online database: PubMed, the Cochrane Library, Embase, Web of Science, Chinese National Knowledge Infrastructure (CNKI) and Wan-fang, with no language restrictions. A Meta-analysis was performed to calculate the pooled odds ratio (OR) and its corresponding 95% confidence interval (CI) for the efficacy and safety of sorafenib combined with TACE in the treatment of HCC. Review Manager 5.4 software was used for data analysis. A total of 19 randomized controlled trials involving 2,029 patients met the inclusion criteria for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
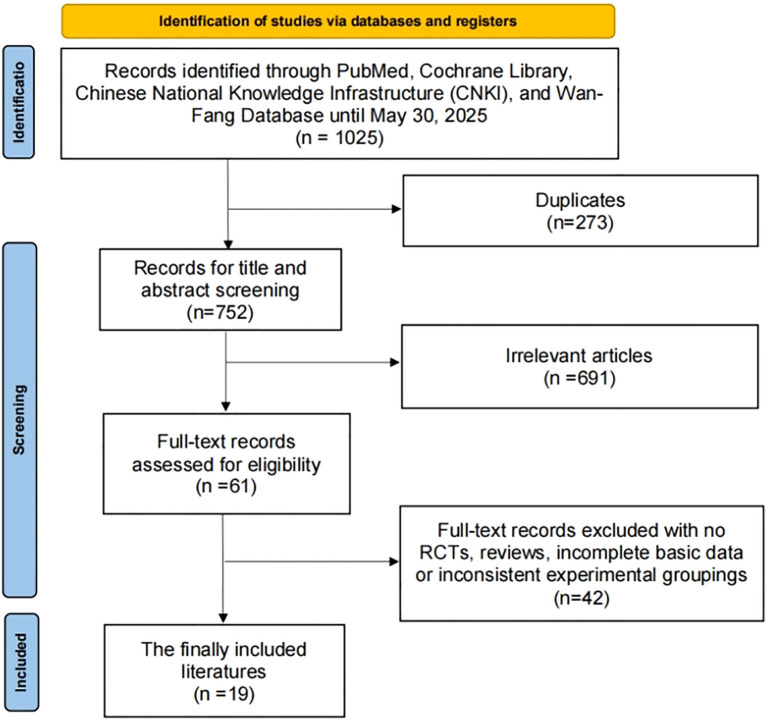 Figure 1
Figure 1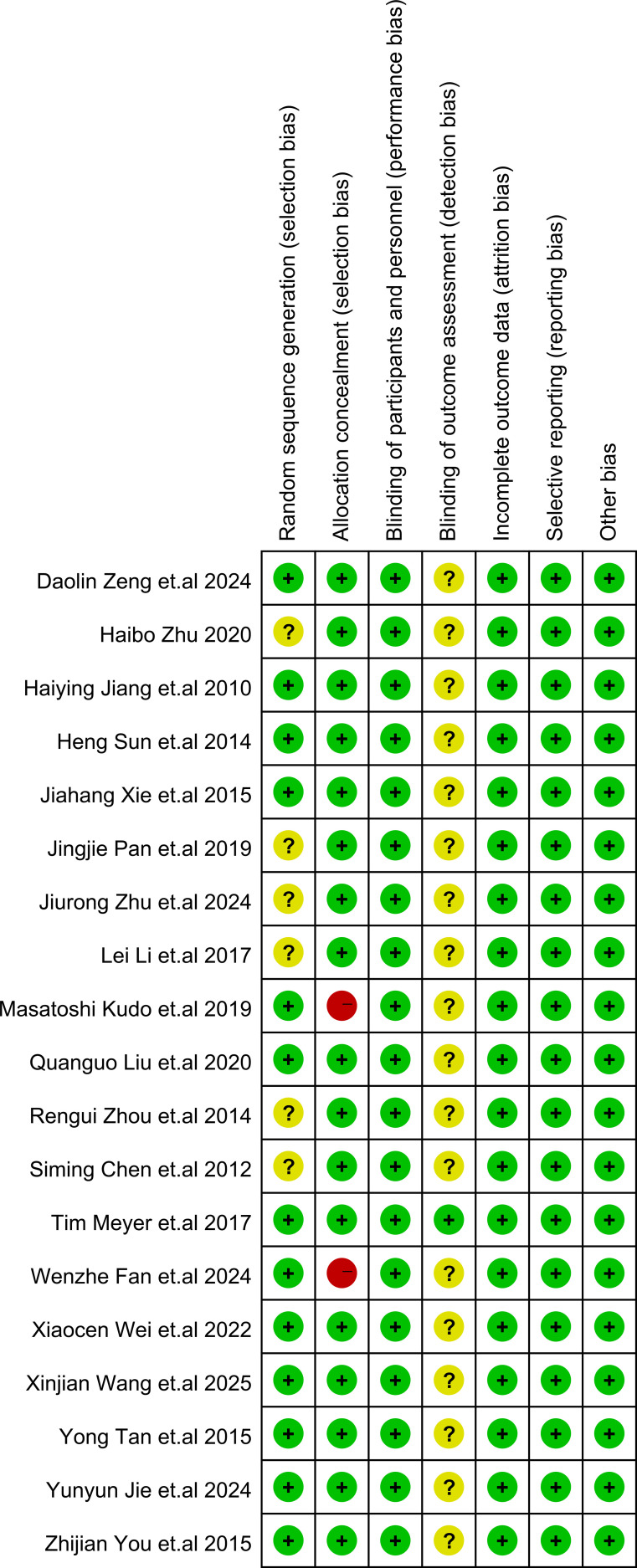 Figure 2
Figure 2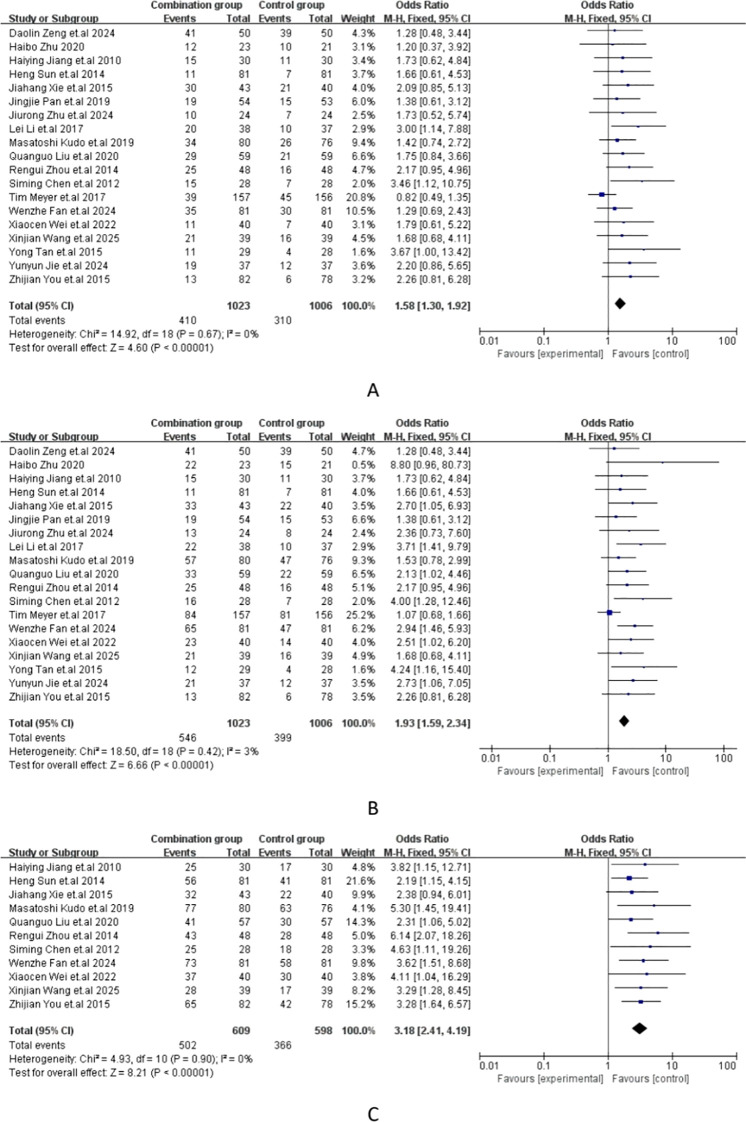 Figure 3
Figure 3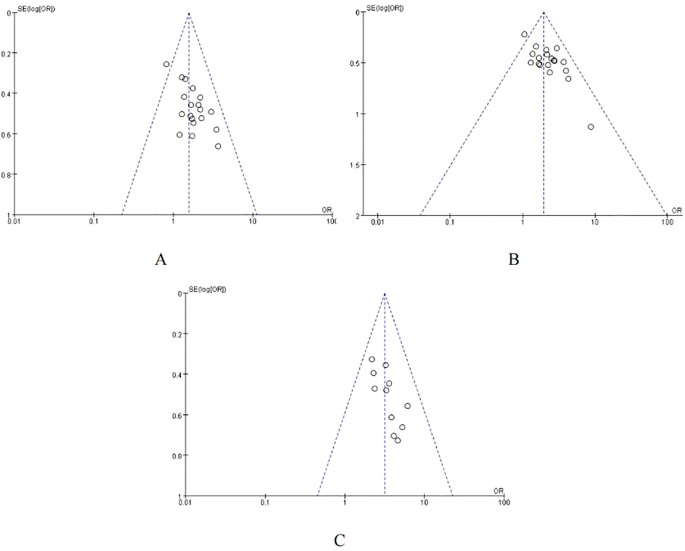 Figure 4
Figure 4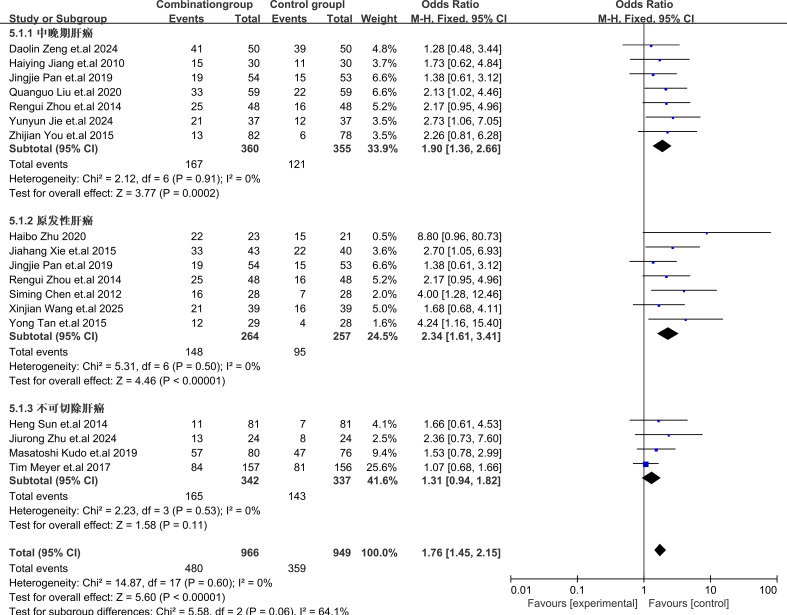 Figure 5
Figure 5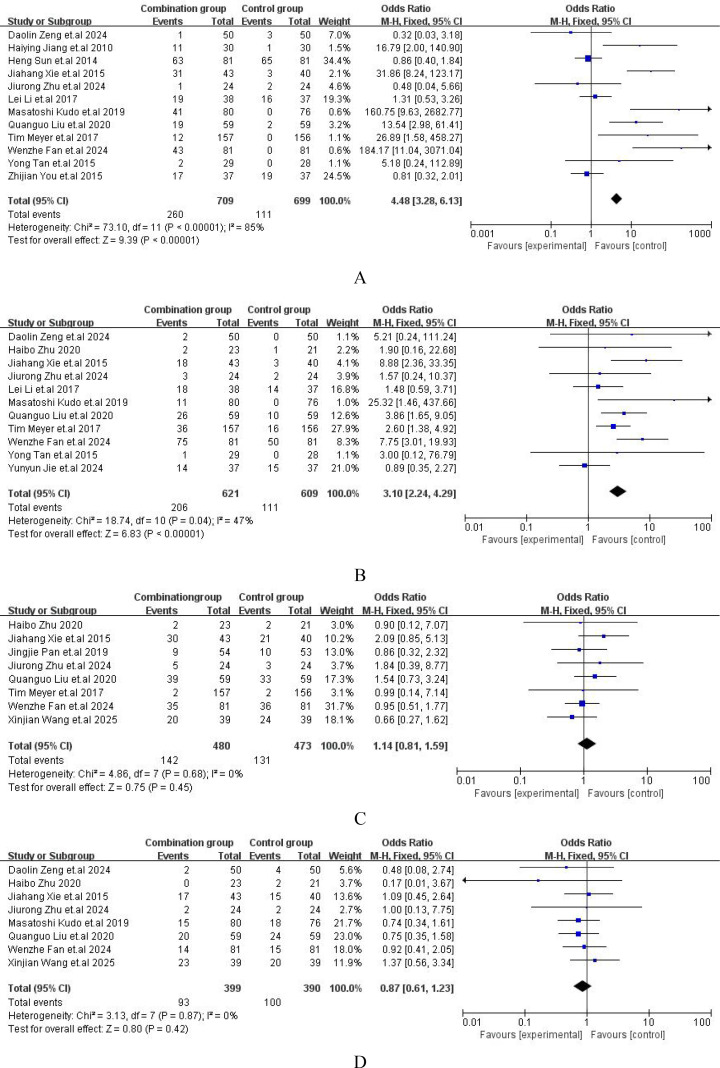 Figure 6
Figure 6| First author | Year | Study design | Group | Cases | Age (year) | Sex (male/female) | Child-Pugh class | ||
|---|---|---|---|---|---|---|---|---|---|
| A | B | C | |||||||
| Xinjian Wang ( | 2025 | RCT | combination group | 39 | 62.91 ± 3.75 | 25/14 | 29 | 10 | 0 |
| control group | 39 | 63.18 ± 4.22 | 27/12 | 28 | 11 | 0 | |||
| Yunyun Jie ( | 2024 | RCT | combination group | 37 | 60.77 ± 4.51 | 20/17 | 16 | 21 | 0 |
| control group | 37 | 61.34 ± 4.45 | 22/15 | 18 | 19 | 0 | |||
| Jiurong Zhu ( | 2024 | RCT | combination group | 24 | 54.26 ± 4.68 | 13/11 | 17 | 7 | 0 |
| control group | 24 | 54.93 ± 5.54 | 14/10 | 16 | 8 | 0 | |||
| Wenzhe Fan ( | 2024 | RCT | combination group | 81 | 54 | 72/9 | 81 | 0 | 0 |
| control group | 81 | 58 | 79/2 | 81 | 0 | 0 | |||
| Daolin Zeng ( | 2024 | RCT | combination group | 50 | 56.13 ± 4.72 | 27/23 | NA | NA | NA |
| control group | 50 | 54.58 ± 5.37 | 29/21 | NA | NA | NA | |||
| Xiaocen Wei ( | 2022 | RCT | combination group | 40 | 49.62± 2.14 | 23/17 | 24 | 16 | 0 |
| control group | 40 | 49.24± 2.11 | 22/18 | 25 | 15 | 0 | |||
| Quanguo Liu et al., 202022 ( | 2020 | RCT | combination group | 59 | 56.31 ± 9.87 | 37/22 | 43 | 16 | 0 |
| control group | 59 | 58.11 ± 10.44 | 32/27 | 48 | 11 | 0 | |||
| Haibo Zhu ( | 2020 | RCT | combination group | 23 | 58.50 ± 5.30 | 12/11 | 16 | 7 | 0 |
| control group | 21 | 57.50 ± 5.10 | 11/10 | 15 | 6 | 0 | |||
| Jingjie Pan ( | 2019 | RCT | combination group | 54 | 55.82 ± 13.04 | 36/18 | 35 | 19 | 0 |
| control group | 53 | 54.96 ± 14.15 | 30/23 | 33 | 20 | 0 | |||
| Masatoshi Kudo ( | 2019 | RCT | combination group | 80 | 72 | 63/17 | 79 | 1 | 0 |
| control group | 76 | 73 | 55/21 | 71 | 5 | 0 | |||
| Tim Meyer ( | 2017 | RCT | combination group | 157 | 65 | 139/18 | 145 | 5 | 0 |
| control group | 156 | 68 | 138/18 | 148 | 3 | 0 | |||
| Lei Li ( | 2017 | RCT | combination group | 38 | 53.70 ± 10.30 | 23/15 | 18 | 20 | 0 |
| control group | 37 | 53.40 ± 10.50 | 22/15 | 17 | 20 | 0 | |||
| Jiahang Xie ( | 2015 | RCT | combination group | 43 | 54.20 ± 7.10 | 34/9 | 30 | 13 | 0 |
| control group | 40 | 53.9 ± 7.5 | 30/10 | 28 | 12 | 0 | |||
| Yong Tan ( | 2015 | RCT | combination group | 29 | 52.3 ± 5.1 | 19/10 | 20 | 9 | 0 |
| control group | 28 | 53.10 ± 5.30 | 17/11 | 19 | 9 | 0 | |||
| Zhijian You ( | 2015 | RCT | combination group | 82 | 24-76 | 60/22 | 65 | 12 | 5 |
| control group | 78 | 26-75 | 50/28 | 52 | 23 | 3 | |||
| Rengui Zhou ( | 2014 | RCT | combination group | 48 | 71.90 ± 12.70 | 34/14 | NA | NA | NA |
| control group | 52 | 67.90 ± 10.80 | 31/17 | NA | NA | NA | |||
| Heng Sun ( | 2014 | RCT | combination group | 81 | 54.50 ± 7.90 | 68/13 | 70 | 11 | 0 |
| control group | 81 | 53.90 ± 8.20 | 66/15 | 72 | 9 | 0 | |||
| Siming Chen ( | 2012 | RCT | combination group | 28 | 68.2 | 20/8 | 15 | 13 | 0 |
| control group | 28 | 68.2 | 17/11 | 16 | 12 | 0 | |||
| Haiying Jiang ( | 2010 | RCT | combination group | 30 | 56 | 24/6 | 25 | 5 | 0 |
| control group | 30 | 57 | 23/7 | 24 | 6 | 0 | |||
| Studies | Group | Cases | AFP (ng/ml) | VEGF (pg/ml) | ||
|---|---|---|---|---|---|---|
| Before treatment | After treatment | Before treatment | After treatment | |||
| Xinjian Wang et al., 2025 ( | treatment group | 39 | 369.51 ± 50.32 | 92.93 ± 24.42 | NA | NA |
| control group | 39 | 372.45 ± 51.45 | 121.72 ± 30.91 | NA | NA | |
| Yunyun Jie et al., 2024 ( | treatment group | 37 | 691.45 ± 130.57 | 133.67 ± 79.36 | 344.67 ± 64.56 | 271.46 ± 54.27 |
| control group | 37 | 684.52 ± 123.66 | 231.44 ± 88.78 | 345.37 ± 66.47 | 228.67 ± 47.56 | |
| Jiurong Zhu et al., 2024 ( | treatment group | 24 | 222.26 ± 13.16 | 71.71 ± 6.31 | NA | NA |
| control group | 24 | 219.43 ± 12.13 | 98.04 ± 9.01 | NA | NA | |
| Xiaocen Wei et al., 2022 ( | treatment group | 40 | 341.87 ± 34.21 | 158.39 ± 25.31 | 501.28 ± 35.42 | 278.53 ± 26.31 |
| control group | 40 | 341.59 ± 34.19 | 187.42 ± 26.53 | 502.13 ± 35.49 | 316.53 ± 25.41 | |
| Quanguo Liu et al., 2020 ( | treatment group | 59 | 516.65 ± 104.31 | 292.86 ± 78.49 | 478.13 ± 70.92 | 254.28 ± 50.81 |
| control group | 59 | 495.85 ± 110.93 | 361.18 ± 69.58 | 465.80 ± 84.69 | 337.47 ± 61.53 | |
| Lei Li et al., 2017 ( | treatment group | 38 | 738.2 ± 185.8 | 118.4± 46.7 | 331.0 ± 76.2 | 279.7 ± 57.6 |
| control group | 37 | 720.6 ± 177.4 | 224.5 ± 102.1 | 342.8 ± 81.6 | 220.5 ± 40.8 | |
| Rengui Zhou et al., 2014 ( | treatment group | 48 | 176.9 ± 14.9 | 83.9 ± 10.2 | NA | NA |
| control group | 52 | 172.7 ± 14.3 | 134.8 ± 13.5 | NA | NA | |
| Siming Chen et al., 2012 ( | treatment group | 28 | 182.36 ± 4.27 | 85.59 ± 7.2 | NA | NA |
| control group | 28 | 169.83 ± 6.2 | 131.32 ± 12.8 | NA | NA | |
| Haiying Jiang et al., 2010 ( | treatment group | 30 | NA | NA | 261.78 ± 139.36 | 146.45 ± 120.23 |
| control group | 30 | NA | NA | 262.67 ± 140.45 | 295.56 ± 127.27 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatocellular Carcinoma Treatment and Prognosis · Liver physiology and pathology · Silymarin and Mushroom Poisoning
Introduction
1
Hepatocellular carcinoma (HCC) is the most common types of primary malignant tumor of the liver, posing a significant threat to human health (1). The treatment of HCC presents challenges due to the disease’s complexity, which is typically diagnosed at an advanced stage and often develops in the context of cirrhosis (2). The treatment methods for liver cancer include surgical resection, liver transplantation, local ablation, transarterial embolization, and transarterial chemoembolization (TACE). Surgical resection and liver transplantation are considered as radical treatment methods for liver cancer. However, due to patients often with severe liver function impairment, the surgical resection rate remains relatively low. Local ablation techniques, such as radiofrequency ablation and microwave ablation, are appropriate for patients with small hepatocellular carcinomas but show limited effectiveness for larger tumors. Consequently, for patients with intermediate to advanced liver cancer, TACE is often employed as a local interventional therapy.
TACE is a classic interventional treatment method for intermediate and advanced stage hepatocellular carcinoma. It precisely delivered chemotherapeutic drugs and embolic agents directly to the tumor through the hepatic artery, cutting off the tumor’s blood supply and increasing the local concentration of medication (3). This method has been shown to prolong survival rates in patients with intermediate-stage HCC. However, it also has its limitations. Due to incomplete embolization and the establishment of collateral blood vessels in the tumor, TACE often fails to achieve pathological necrosis. Additionally, postoperative ischemia and hypoxia in tumor tissues can increase the level of hypoxia-inducible factors in residual tumors and elevate the expression of vascular endothelial growth factor(VEGF), aggravating the disease and recurrence (4, 5).
In recent years, targeted therapy has made significant progress in the treatment of advanced liver cancer. Sorafenib, a multi-kinase inhibitor, suppresses tumor angiogenesis by targeting the VEGF signaling pathway, inhibiting tumor growth and metastasis. As the standard first-line treatment drug, it can significantly extend the overall survival of patients with advanced liver cancer (6, 7). However, the efficacy of sorafenib monotherapy remains limited, potentially leading drug resistance in some patients. Exploring combination therapy regimens has become a research hotspot. Studies have shown that sorafenib plus TACE may enhance the control of local tumor after TACE and mitigate hypoxia-driven metastasis (8). Thus, the combination of sorafenib with TACE has gained attention as a potential therapeutic strategy (9, 10).
With the incidence of HCC rising, optimizing treatment strategies for patients with intermediate to advanced liver cancer has become increasingly urgent. Studies have indicated that the combination of sorafenib and TACE may offer potential benefits in the treatment of HCC. However, there is a lack of systematic summary and evaluation, and inconsistencies in their results (11). To address this issue and provide valuable insights for clinical practice, we conducted a systematic review and meta-analysis focusing on the efficacy and safety of TACE plus sorafenib for the treatment of HCC (12, 13).
Methods
2
Literature search
2.1
During this systematic review, we adhered to the PRISMA guidelines (14). A comprehensive system retrieved online databases: PubMed, the Cochrane Library, Embase, Web of Science, the Chinese National Knowledge Infrastructure (CNKI), and the Wan-Fang Database in China without language restrictions on May 30, 2025. MeSH terms and free words related to “Hepatocellular Carcinoma”, “sorafenib” and “Therapeutic Chemoembolization” were used in this research. Details of search strategy were displayed in Supplementary File S1. Additionally, we manually screened the references of all identified articles for additional studies that might be relevant to this meta-analysis.
Inclusion and exclusion criteria
2.2
Inclusion criteria
Randomized controlled trials (RCTs).Study patients were pathologically or clinically diagnosed with hepatocellular carcinoma, regardless of the kind of treatment that they have experienced before.Two intervention arms (TACE plus sorafenib vs TACE alone) were compared in the study.One of the following must be reported in study: partial response rate (PR), objective response rate (ORR), 12-month OS rates and adverse reactions.There is no language restriction.
Exclusion criteria
Duplicate studies.Non-RCTs.Inconsistent experimental groupings.The basic data was incomplete and the original data was unavailable.Reviews, meta-analyses, non-clinical reports, case reports, conference summaries, opinions, editorials and letters.
Data extraction
2.3
Data was extracted independently by two investigators (Lixiu Yu and Yi Xiong) according to the inclusion and exclusion criteria. General information of the eligible studies including first author’s name, published year, study design, case of participants in the eligible studies, age, gender, Child-Pugh class. Efficacy outcome measures included PR, ORR, 12-month OS rates. Safety outcomes included typical adverse events (AEs) reported by patients. Disagreements between the investigators were resolved through discussion.
Quality assessment
2.4
The quality of the RCTs included in this meta-analysis was evaluated by Cochrane Collaboration’s risk of bias tool (15) from seven critical aspects: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, other bias. Each aspect was judged as low, unclear, or high risk of bias. The quality assessment was conducted independently by two researchers (Yi Xiong and Lixiu Yu). Disagreements were resolved by discussion.
Data synthesis and analysis
2.5
Meta-analyses were conducted by using Review Manager 5.4. The pooled odds ratio (OR) and 95% confidence interval (CI) were employed to evaluate efficacy and safety. The I2 statistic was used to measure heterogeneity of the studies. If significant heterogeneity was detected with I² > 50%, the estimated outcomes of eligible studies were calculated using a random-effects model. Otherwise, a fixed-effects model was applied. And statistical test with p < 0.05 was considered significant.
Results
3
Study search and selection
3.1
As depicted in Figure 1, the study selection process involved a comprehensive search of online databases and manual searches, yielding a total of 1025 articles. After eliminating 273 duplicate articles, further 691 articles were excluded based on their titles and abstracts. Upon full-text review and applying the inclusion criteria, 42 articles were excluded. Ultimately, 19 RCTs, comprising a total of 2,029 patients diagnosed with liver cancer, were included in this study (10, 16–33).
The process of selection of the eligible studies.
Study characteristics
3.2
A total of 19 RCTs were included in this meta-analysis, of these 17 studies (10, 16–19, 21–29, 31–33) reported Child-Pugh classification system. Majority of patients were classified as Child-Pugh class A. The baseline characteristics of patients were summarized in Table 1. Of the 2029 enrolled patients with HCC, 1,023 received sorafenib plus TACE, and1,006 were treated with TACE alone. The patients’ ages were between 45 and 75 years old. Sorafenib was administered orally at a dosage of 400 mg twice daily. The details of intervention characteristics and outcome measures of all the included trials were summarized in Supplementary File S2. All the trials (10, 16–33) used PR and ORR as outcome metrics, and eleven trials (10, 16, 19, 21, 22, 27, 29–33) reported 12-month OS rates.
Quality assessment
3.3
The details of study quality assessment were summarized in Figure 2 and Supplementary File S3. The Cochrane Collaboration’s risk of bias tool was used to evaluate the quality of included studies. Overall, the included studies revealed a superior standard of methodological quality. Most studies presented a low risk of bias.
Risk of bias summary. In the illustration, green represents low risk, yellow represents unclear risk, and red represents high risk.
Meta-analysis results
3.4
Efficacy of sorafenib combined with TACE
3.4.1
The meta-analysis of all the included studies indicated that compared with TACE alone, Sorafenib combined with TACE had a favorable partial response rate (PR) with integrated OR = 1.58 (95% CI: 1.30–1.92), P = 0.67, I² = 0%. In addition, the result of objective response rate (ORR) with pooled OR = 1.93, 95%CI (1.59,2.34)] and 12-months OS rate with pooled OR = 3.18, 95%CI (2.41,4.19) demonstrated that TACE plus sorafenib had better clinical outcomes than TACE alone. The details of the efficacy and funnel plot were summarized in Figures 3 and 4 respectively. One the other hand, the available data in Table 2 suggested that both APF and VEGF levels decreased after treatment especially for TACE plus sorafenib, which further proved that the combination of TACE and sorafenib was an effective strategy.
(A) Forest plot of partial response rate (PR); (B) Forest plot of objective response rate(ORR); (C) Forest plot of the 12-month OS rates.
Funnel plot of ORR. (A) Funnel plot of PR; (B) Funnel plot of ORR; (C) Funnel plot of the 12-month OS rates.
Subgroup analysis
3.4.2
Subgroup analysis of different types of HCC showed that TACE plus sorafenib for patients with primary HCC provided the best benefits with OR = 2.34, 95% CI (1.61,3.41), I2 = 0%, P = 0.50, for intermediate-advanced HCC OR = 1.90, 95% CI (1.36,2.66), I2 = 0%, P = 0.91], and for unresectable HCC OR = 1.31, 95% CI (0.94,1.81), I2 = 0%, P = 0.53. These results indicated that sorafenib combined with TACE showed a statistically significant difference in efficacy compared with TACE alone for the treatment of intermediate-advanced and primary HCC. However, for the treatment of unresectable HCC, there was no statistically significant difference in efficacy. The subgroup analysis details were presented in Figure 5.
Forest plot of the subgroup analysis.
Safety evaluation
3.4.3
The major adverse events (AEs) from all included studies were presented in Supplementary File S4. Compared with TACE alone, the incidence of hand-foot skin reaction [OR = 4.48, 95%CI (3.28,6.13), P < 0.00001] (Figure 6A) and abdominal pain or diarrhea [OR = 3.10, 95%CI (2.24,4.29), P = 0.04] (Figure 6B) were both higher than those with TACE plus sorafenib. However, the incidence of nausea or vomiting [OR = 1.14, 95%CI (0.81,1.59), P = 0.68] (Figure 6C) or fever [OR = 0.87, 95%CI (0.61,1.23), P = 0.87] (Figure 6D) between the two groups was no significant difference. The comprehensive details of the safety were outlined in Figure 6.
Forest plot of safety analysis. (A) Hand and foot skin reaction; (B) Diarrhea or abdominal pain; (C) Nausea or vomit; (D) Fever.
Discussion
4
In the present study, we systematically evaluated the efficacy and safety of sorafenib in combination with TACE versus TACE alone on the treatment of HCC, providing a definitive systematic review with updated data. A total of 19 randomized controlled trials (10, 16–33), encompassing 2029 patients, were identified and included in this meta-analysis. The results indicated that compared with TACE alone, the combination of sorafenib and TACE significantly improved patient prognosis. Our findings further confirmed the combination of TACE and sorafenib significantly improved the clinical outcomes for the treatment of HCC.
In terms of efficacy, the combined therapy demonstrated a significant advantage over TACE alone in PR, ORR and the 12-month OS rates. Notably, the combination regimen yielded a substantial clinical benefit with an OR = 1.93 for ORR, which was consistent with the report by Chen et al. (34) (OR = 2.19). Sorafenib is a multi-kinase inhibitor that inhibits the activity of vascular endothelial growth factor receptor (VEGFR) and the platelet-derived growth factor receptor (PDGFR) and reduce the formation of new blood vessels in HCC tumors. It can also reduce the number and activity of immune-suppressive cells (such as regulatory T cells and myeloid-derived suppressor cells), and strengthen anti-tumor immunity (35). TACE works by embolizing the feeding arteries to the tumor, and reducing its blood supply, leading to tumor shrinkage and has an improved prognosis for HCC patients. Studies proved that TACE plus sorafenib had significantly enhanced the efficacy for HCC patients (36–39).
Subgroup analysis revealed that the efficacy of combination therapy was superior to TACE alone in patients with intermediate-advanced HCC and primary HCC. However, the benefit for unresectable HCC patients was not significant with OR = 1.31(0.94,1.82). There were some discrepancies between these findings and the TACTICS trial (10) which conducted by several domestic centers and reported significant clinical benefits of sorafenib plus TACE in unresectable HCC. The variation for this may be related to sample size and differences in sorafenib regimens. Increasing sample size tends to reduce the error. TACTICS trial only included 156 patients with unresectable HCC, while our work included 679 patients with this subtype. Additionally, the regimens for sorafenib may have some impacts on the outcomes. Among TACTICS trial sorafenib was initiated 14–21 days before TACE at a dose of 400 mg once daily, while this systematical study included both sorafenib initiated before TACE and after TACE regimens. Subgroup analysis indicated that for sorafenib initiated before TACE OR = 1.68(1.25, 2.27), while for sorafenib initiated after TACE OR = 2.32(1.74, 3.11). It still needs further confirmation by more high-quality RCTs with large samples and reliable design.
The present work indicated that there was no significant difference between TACE plus sorafenib group and TACE alone group in aspects of nausea, vomiting and fever. However, the safety results also suggested that compared with TACE alone, the combination of TACE and sorafenib significantly increased the risk of hand-foot skin reaction (HFSR) [OR = 4.48,95%CI (3.28,6.13)], abdominal pain and diarrhea [OR = 3.10,95%CI (2.24,4.29)]. The increased risk of these may relate to the pharmacological properties of sorafenib. It inhibited multiple intracellular signaling pathways in liver carcinoma cells. It can inhibit angiogenesis in tumor tissues and block cancer cell proliferation by inhibiting kinase activities, such as those of c-Raf, VEGFR2, VEGFR3, which can affect the function of the skin and blood vessels leading to HFSR (42). Sorafenib can also lead to a decrease in intestinal mucosal blood supply and repair ability, thereby causing abdominal pain and diarrhea (40). Prioritizing the management of treatment-related toxicities is essential to maintain patient quality of life and ensure treatment adherence (25). It is crucial to find potential ways to reduce adverse reactions, such as providing skin care guidance, adjusting drug doses, and administering antidiarrheal and rehydration therapies.
This study boasts several notable strengths: firstly, our work systematically analyzed 19 RCTs, which had been significantly enhanced in terms of credibility. Secondly, by applying rigorous literature screening criteria and utilizing the Cochrane risk-of-bias tool for quality assessment, the reliability of our research findings is significantly enhanced. Thirdly, in this study, we conducted subgroup analyses to explore differential treatment responses among various patient and comprehensively evaluated the efficacy and safety of TACE plus sorafenib, which indicated that further research needed to fully elucidate the mechanisms behind these observations.
There were some limitations to this study that warranted attention. Firstly, although a quality assessment was conducted, the majority of the trials included exhibited uncertain risks of bias. These uncertainties could potentially impact the accuracy of our study results (41). Secondly, there were some variations in the studies whose data have been complied together not only with different patient characteristics but geographic regions, and most of the articles did not stratify the severity of adverse events. We were also unable to adjust for confounders such as age, sex and medical duration of HCC. In addition, HCC is a highly heterogeneous disease in treatment responses among patients. Other factors related to tumor biology (such as genetic mutation profiles and tumor microenvironment), host factors (such as liver function status and overall health condition), and environmental and lifestyle factors also influence disease progression and prognosis. Due to limited data, information on other relevant factors were not extracted, which may cause some bias in our results. In light of these limitations, future research should conduct more large-scale, multicenter RCTs to minimize individual variability and sampling bias.
Conclusion
5
The combination of TACE plus sorafenib offers therapeutic benefits in the treatment of HCC and may be a choice of treatment in patients with unresectable HCC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rumgay H Arnold M Ferlay J Lesi O Cabasag CJ Vignat J . Global burden of primary liver cancer in 2020 and predictions to 2040. J Hepatol. (2022) 77:1598–606. doi: 10.1016/j.jhep.2022.08.021, PMID: 36208844 PMC 9670241 · doi ↗ · pubmed ↗
- 2Alawyia B Constantinou C . Hepatocellular carcinoma: a narrative review on current knowledge and future prospects. Curr Treat Options Oncol. (2023) 24:711–24. doi: 10.1007/s 11864-023-01098-9, PMID: 37103744 · doi ↗ · pubmed ↗
- 3Chang Y Jeong SW Young Jang J Jae Kim Y . Recent updates of transarterial chemoembolilzation in hepatocellular carcinoma. Int J Mol Sci. (2020) 21:8165. doi: 10.3390/ijms 21218165, PMID: 33142892 PMC 7662786 · doi ↗ · pubmed ↗
- 4Zhou B Wang J Yan Z . Ginsenoside Rg 3 attenuates hepatoma VEGF overexpression after hepatic artery embolization in an orthotopic transplantation hepatocellular carcinoma rat model. Onco Targets Ther. (2014) 7:1945–54. doi: 10.2147/OTT.S 69830, PMID: 25364265 PMC 4211851 · doi ↗ · pubmed ↗
- 5Tao Z Chen B Tan X Zhao Y Wang L Zhu T . Coexpression of VEGF and angiopoietin-1 promotes angiogenesis and cardiomyocyte proliferation reduces apoptosis in porcine myocardial infarction (MI) heart. Proc Natl Acad Sci U S A. (2011) 108:2064–9. doi: 10.1073/pnas.1018925108, PMID: 21245320 PMC 3033313 · doi ↗ · pubmed ↗
- 6European Association for the Study of the Liver . EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J Hepatol. (2018) 69:182–236. doi: 10.1016/j.jhep.2018.03.019, PMID: 29628281 · doi ↗ · pubmed ↗
- 7Kelley RK Rimassa L Cheng AL Kaseb A Qin S Zhu AX . Cabozantinib plus atezolizumab versus sorafenib for advanced hepatocellular carcinoma (COSMIC-312): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. (2022) 23:995–1008. doi: 10.1016/S 1470-2045(22)00326-6, PMID: 35798016 · doi ↗ · pubmed ↗
- 8Kimura Y Kaneko R Yano Y Kamada K Ikehara T Nagai H . The prognosis of hepatocellular carcinoma treated with sorafenib in combination with TACE. Asian Pac J Cancer Prev. (2020) 21:1797–805. doi: 10.31557/APJCP.2020.21.6.1797, PMID: 32592380 PMC 7568902 · doi ↗ · pubmed ↗