A 40-Year Regional Study of Cleft Lip and/or Palate Incidence in Tokai, Japan
Teruyuki Niimi, Chisato Sakuma, Nagana Natsume, Hideto Imura, Kumiko Fujiwara, Ken Kitagawa, Hiroo Furukawa, Nagato Natsume

TL;DR
A 43-year study in Japan's Tokai region found that the incidence of cleft lip and/or palate remained stable despite demographic changes.
Contribution
This paper provides a long-term regional epidemiological analysis of CL/P in Japan, highlighting consistent incidence rates over four decades.
Findings
CL/P incidence remained stable at 10-20 cases per 10,000 live births from 1981 to 2023.
Sex ratios for cleft types shifted after 2004, with males becoming more prevalent for isolated cleft palate.
No significant increase in CL/P or other major congenital anomalies was observed despite rising maternal age and social changes.
Abstract
Objective: Cleft lip and/or palate (CL/P) is among the most common congenital craniofacial anomalies worldwide, with reported incidences ranging from approximately 1 in 500 to 2,500 live births, depending on the geographic region and ethnic background. While genetic and environmental factors contribute to its etiology, long-term regional surveillance is essential to detect trends and identify risk factors. This study investigates the epidemiological characteristics of CL/P in the Tokai region of Japan over a 43-year period (1981-2023). Methods: Since 1981, the Cleft Lip and Palate Center at Aichi Gakuin University Dental Hospital has been conducting an annual population-based monitoring survey involving all obstetric facilities in Aichi, Gifu, and Mie prefectures. Mailed questionnaires captured data on total live births, presence and types of congenital anomalies, CL/P occurrence and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
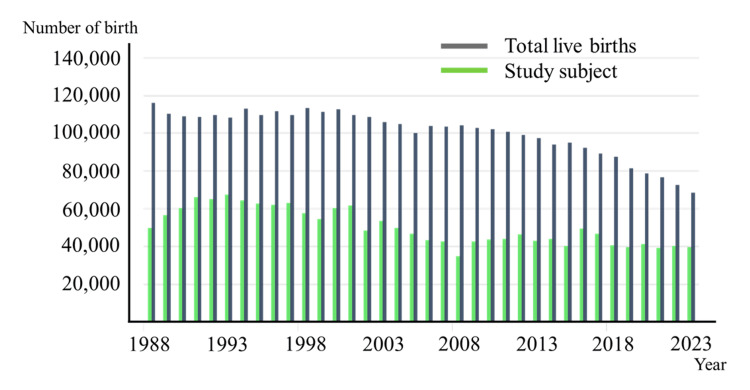 Figure 1
Figure 1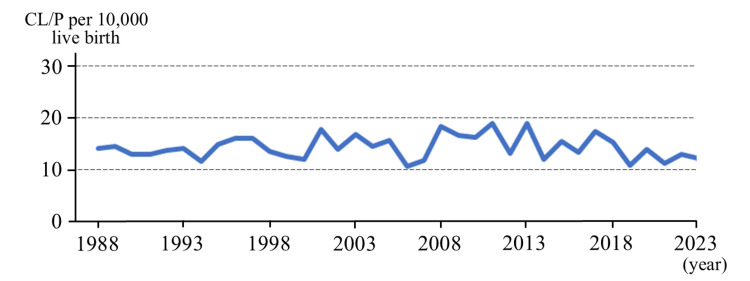 Figure 2
Figure 2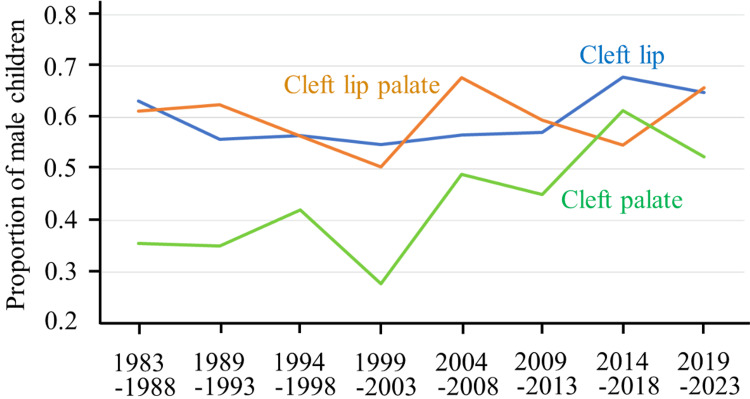 Figure 3
Figure 3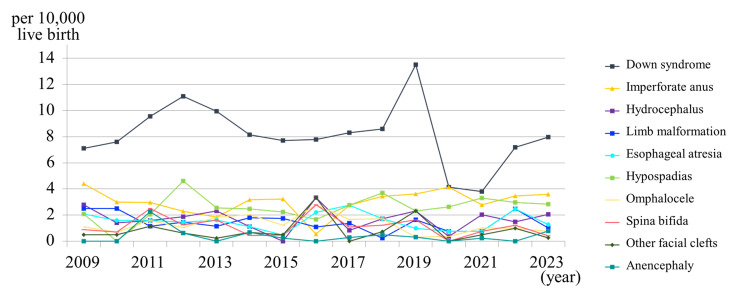 Figure 4
Figure 4| Year | Average age at first marriage for women | Average age at first birth | Average age at second birth | Average age at third birth |
| 1975 | 24.7 | 25.7 | 28.9 | 30.3 |
| 1980 | 25.2 | 26.4 | 28.7 | 30.6 |
| 1985 | 25.5 | 26.7 | 29.1 | 31.4 |
| 1990 | 25.9 | 27.0 | 29.5 | 31.8 |
| 1995 | 26.3 | 27.5 | 29.8 | 32.0 |
| 2000 | 27.0 | 28.0 | 30.4 | 32.3 |
| 2005 | 28.0 | 29.1 | 31.0 | 32.6 |
| 2010 | 28.8 | 30.5 | 31.8 | 33.2 |
| 2015 | 29.4 | 31.1 | 32.5 | 33.5 |
| 2019 | 29.6 | 31.2 | 32.7 | 33.8 |
| Year | Aichi Prefecture | Gifu Prefecture | Mie Prefecture | |||
| Study subject | Number of CL/P cases | Study subject | Number of CL/P cases | Study subject | Number of CL/P cases | |
| 1988 | 33,545 | 40 | 21,791 | 18 | 18,931 | 13 |
| 1989 | 40,091 | 58 | 20,614 | 12 | 18,183 | 13 |
| 1990 | 34,034 | 44 | 20,295 | 18 | 17,918 | 17 |
| 1991 | 39,078 | 45 | 20,033 | 25 | 17,519 | 16 |
| 1992 | 44,094 | 54 | 20,347 | 23 | 17,686 | 13 |
| 1993 | 41,569 | 71 | 20,017 | 15 | 17,368 | 10 |
| 1994 | 41,462 | 50 | 20,623 | 10 | 18,144 | 15 |
| 1995 | 38,577 | 58 | 20,187 | 20 | 17,500 | 16 |
| 1996 | 37,100 | 57 | 20,546 | 26 | 17,780 | 17 |
| 1997 | 39,912 | 62 | 19,930 | 25 | 17,660 | 14 |
| 1998 | 33,351 | 46 | 20,447 | 18 | 17,829 | 14 |
| 1999 | 33,271 | 56 | 20,151 | 9 | 17,375 | 4 |
| 2000 | 38,707 | 53 | 20,276 | 6 | 17,726 | 14 |
| 2001 | 37,632 | 62 | 19,603 | 25 | 17,094 | 23 |
| 2002 | 29,449 | 48 | 19,617 | 11 | 17,190 | 9 |
| 2003 | 33,112 | 58 | 19,156 | 19 | 16,497 | 13 |
| 2004 | 29,537 | 48 | 18,363 | 12 | 16,287 | 13 |
| 2005 | 27,243 | 41 | 17,706 | 16 | 15,345 | 16 |
| 2006 | 26,121 | 27 | 18,092 | 13 | 15,816 | 6 |
| 2007 | 24,441 | 34 | 17,696 | 11 | 15,716 | 6 |
| 2008 | 22,435 | 38 | 17,506 | 16 | 15,633 | 10 |
| 2009 | 28,399 | 46 | 17,327 | 9 | 15,614 | 16 |
| 2010 | 27,846 | 44 | 16,887 | 13 | 15,262 | 14 |
| 2011 | 31,069 | 52 | 16,851 | 21 | 15,080 | 10 |
| 2012 | 34,281 | 41 | 16,496 | 11 | 14,729 | 9 |
| 2013 | 33,041 | 67 | 16,000 | 7 | 14,514 | 8 |
| 2014 | 31,598 | 37 | 15,138 | 7 | 13,727 | 9 |
| 2015 | 29,483 | 47 | 15,464 | 11 | 13,950 | 4 |
| 2016 | 34,013 | 43 | 14,831 | 13 | 13,202 | 10 |
| 2017 | 31,361 | 63 | 14,039 | 12 | 12,663 | 7 |
| 2018 | 29,039 | 52 | 13,719 | 7 | 12,582 | 3 |
| 2019 | 26,366 | 28 | 12,776 | 9 | 11,690 | 6 |
| 2020 | 29,118 | 45 | 12,092 | 6 | 11,141 | 5 |
| 2021 | 26,540 | 30 | 11,730 | 9 | 10,980 | 5 |
| 2022 | 28,524 | 43 | 11,124 | 4 | 10,489 | 5 |
| 2023 | 27,524 | 39 | 10,469 | 1 | 9524 | 8 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCleft Lip and Palate Research · Craniofacial Disorders and Treatments
Introduction
Cleft lip and/or palate (CL/P) ranks among the most frequently encountered congenital craniofacial malformations worldwide, with an estimated incidence of 1 per 500 to 2,500 live births [1-3]. Beyond its morphological implications, CL/P can cause significant functional challenges, including feeding difficulty, speech impairment, otitis media-associated hearing loss, dental and occlusal abnormalities, and psychological or social development issues, warranting early and sustained multidisciplinary care [4].
The incidence of CL/P is influenced not only by genetic predisposition but also by environmental exposures, ethnicity, geographic region, temporal trends, and the diagnostic/reporting capabilities of healthcare systems [5-8]. In addition, advances in prenatal diagnostic technology and the option of pregnancy termination can alter the apparent incidence reported at birth, although the extent of this influence varies across countries and cultural contexts. Consequently, detailed regional epidemiological surveillance is critical for evaluating incidence trends, identifying potential risk factors, and informing preventive strategies and health policy.
In Japan, regional variability in CL/P incidence has been observed. Social phenomena such as delayed marriage and advanced maternal age have been suggested as potential risk modifiers; however, to our knowledge, no studies have directly examined the association between maternal age and CL/P incidence in the Japanese population. In response, robust regional monitoring infrastructure and accurate dissemination of localized data have become academic and public health priorities.
Beginning in 1981, the Cleft Lip and Palate Center at Aichi Gakuin University Dental Hospital has led a regional epidemiological monitoring initiative encompassing all obstetric facilities in the three prefectures of Tokai (Aichi, Gifu, and Mie). This program, arguably one of Japan’s most enduring and comprehensive CL/P surveillance systems, has accrued over four decades of high-quality data, receiving significant recognition both nationally and internationally.
This manuscript presents an analysis of CL/P incidence in Tokai from 1981 to 2023. We assess annual trends in incidence, cleft type distribution, sex ratio, and associated anomaly rates. We also consider the influence of sociocultural changes, particularly delayed childbearing, on CL/P occurrence.
This study aims to (1) describe long-term trends in the annual incidence of CL/P across the Tokai region (Aichi, Gifu, and Mie prefectures) over a 43-year period (1981-2023), (2) examine whether there were significant temporal changes in the overall CL/P incidence during this period, and (3) compare the regional incidence patterns with recent national and global epidemiological findings.
Materials and methods
This retrospective epidemiological study utilized data from a CL/P surveillance system conducted by the Cleft Lip and Palate Center at Aichi Gakuin University Dental Hospital since 1981. The survey targeted all delivery-capable healthcare facilities (hospitals, clinics, and maternity centers) located in Aichi, Gifu, and Mie prefectures. These three prefectures constitute the Tokai region, situated in Central Honshu, Japan’s main island, between the Kanto region to the east (Tokyo area) and the Kansai region to the west (Osaka, Kyoto). According to the 2020 National Census, the Tokai region has a total population of approximately 10.1 million (Aichi, 7.5 million; Gifu, 2.0 million; and Mie, 1.5 million), accounting for about 8% of Japan’s total population. Each annual survey period ran from January 1 to December 31, excluding stillbirths and terminations, with data collected per calendar year.
A mailed questionnaire was distributed annually to all eligible obstetric providers. The list of institutions was updated each year based on the Ministry of Health, Labour and Welfare’s designated maternal protection facility registry and local government facility listings. Respondents were asked to report the following items based on their routine clinical diagnostic practice, as no additional training or standardized diagnostic definitions were provided: (1) total live births in the year, (2) presence and type of any congenital anomalies (based on routine clinical diagnosis at each facility; no specific international coding system, such as ICD-11, was mandated), (3) occurrence of CL/P, (4) cleft subtype (isolated lip, isolated palate, or combined lip and palate), (5) sex of the affected infant, and (6) presence of associated anomalies (e.g., cardiac malformations, limb defects, chromosomal abnormalities).
The questionnaires were paper-based and, once completed, were transcribed into a dedicated electronic database. To ensure data quality, all entries were checked by a second member of the research team, and any discrepancies were resolved by re-checking the original questionnaire forms. Annual incidence rates of CL/P (per 10,000 live births), type-specific distributions, sex ratios, geographic breakdowns, and rates of associated anomalies were calculated. Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 26.0 (Released 2018; IBM Corp., Armonk, NY, US). Differences in categorical variables such as sex ratios and trends were assessed with chi-square tests or Fisher’s exact tests when appropriate. A p-value of less than 0.05 was considered statistically significant.
To evaluate the potential impact of non-response bias, we performed a sensitivity analysis assuming different incidence rates in non-responding institutions.
Institutional review and ethical approval were obtained from the Japan Oral Care Association Ethics Committee.
Results
Survey response rate
The survey response rate was defined as the proportion of newborns born at facilities that returned the annual survey form, out of all newborns born at facilities capable of providing delivery care identified in the public registry in Aichi, Gifu, and Mie Prefectures. The rate was approximately 30% in 1981, exceeded 40% after 1988, and stabilized between 50% and 60% from the 2000s onward (Figure 1). When non-responding institutions were assumed to have the same incidence as responding ones, the overall incidence remained 0.15%. If non-responding institutions were assumed to have 20% lower or 20% higher incidence rates, the overall incidence changed only marginally, ranging from 0.14% to 0.16%. These results indicate that the potential impact of non-response bias on our overall incidence estimates is minimal.
Trends in the number of births and study registrants in the three Tokai prefecturesBirth numbers have been declining annually, whereas the questionnaire response rate has shown an upward trend, reaching around 60% in recent years. "Total birth" refers to the number of live births in the three Tokai prefectures as reported by the Ministry of Health, Labour and Welfare. "Study subject" refers to the number of live births at the institutions that responded to the survey.
Trends in CL/P incidence
From 1981 to 2023, annual live birth counts in Aichi initially exceeded 70,000 but declined to under 50,000 by 2023. This reduction reflects the nationwide demographic trend of declining fertility in Japan, largely due to delayed marriage [9], reduced family size, and a shrinking population of women of childbearing age, rather than region-specific factors or selective termination (Table 1). CL/P incidence remained between 10 and 20 per 10,000 births (1 in 500-1,000 births). Gifu and Mie experienced similar birth declines, to around 10,000 by 2023, with CL/P incidence across prefectures ranging between 8 and 14 per 10,000 births in Gifu and 4 and 23 per 10,000 births in Mie (Table 2). The overall incidence across the three prefectures was 14.45 per 10,000 births (95% CI: 13.89-15.00). No statistically significant upward or downward trends were observed within each prefecture or region-wide (chi-square test: Aichi, p = 0.40; Gifu, p = 0.10; Mie, p = 0.89; overall region: p = 0.89) (Figure 2).
Annual incidence rates of CL/P per 10,000 live births in Aichi, Gifu, and Mie Prefectures, Tokai region, Japan (1988-2023)Data from 1981-1987 are not plotted because some facilities had incomplete reporting in those early years; reporting completeness improved after 1988 (survey response rate exceeded ~40%); therefore, the figure presents annual rates from 1988 onward for clearer trend interpretation. The incidence rate of CL/P is 10-20 per birth, and no significant change has been observed over the past 40 years.
Cleft type and sex ratio
Subtype distributions were consistent over time. Males predominated in cases of CL and CLP, while historical data showed a female predominance in CP (Figure 3).
Sex differences among children with CL, CLP, and CPCL and CLP occur more frequently in males, while CP is more common in females. However, in recent years, the gender difference in CP has become less distinct.CL: cleft lip, CLP: cleft lip with cleft palate, CP: cleft palate.
Associated congenital anomalies
From 2009 onward, additional data were collected on cardiac, limb, neural tube, and chromosomal anomalies. Between 2009 and 2023, their prevalence remained stable, with no significant year-to-year changes or upward trends in any category (chi-square test for trend, p > 0.05) (Figure 4).
Annual trends in the incidence rates of other major congenital anomalies in the Tokai region, Japan (2009-2023)Although the incidence of Down syndrome shows considerable annual variation, the overall incidence rates of congenital anomalies have not changed during the last 15 years.
Discussion
As reported in the Results section, the annual survey response rate gradually increased from approximately 30% in 1981 to stabilize between 50% and 60% from the 2000s onward. The gradual improvement in response rates may have been facilitated by enhanced engagement efforts, including distribution of annual summary booklets, collaboration with the Japanese Cleft Palate Foundation (JCPF), provision of feeding support materials, and performance-based feedback and recognition incentives. This likely contributed to the completeness and reliability of the collected data over time.
From 1981 to 2023, annual live birth counts in Aichi declined gradually. The decline in annual live births observed in the Tokai region mirrors Japan’s nationwide demographic shift, driven mainly by lower fertility rates and changes in reproductive behavior, such as delayed marriage and childbearing. In this longitudinal regional surveillance study spanning over four decades, the incidence of CL/P in the Tokai region remained remarkably stable (0.10%-0.20%), despite demographic changes such as declining birth rates, delayed marriage, and rising maternal age [9] (Table 1). This stability suggests that CL/P is primarily influenced by genetic predisposition and less by short-term environmental or social shifts. Moreover, despite improvements in prenatal diagnostic capabilities, termination based solely on CL/P is not common in Japan, potentially accounting for the unchanging birth incidence. Although demographic and social factors such as delayed marriage and rising maternal age have changed markedly over the study period, the present data do not allow direct causal inferences regarding their relationship with CL/P incidence. These observations should be interpreted as concurrent trends rather than causal associations.
The sex distribution patterns observed in the Tokai region, male predominance in CL/CLP and female predominance in CP, are consistent with those reported across other regions of Japan and in international studies. Although the reversal of the CP sex ratio after 2004 was observed, the sample size for CP cases was relatively small. This represents a notable observation that warrants further investigation, as ongoing detailed analyses may provide additional insights.
Although minor fluctuations in the CP sex ratio were observed, the number of cases was small, and detailed subtype analyses are being conducted in a separate study. In this report, we focus on overall CL/P incidence trends. The stable incidence over 43 years provides important information for healthcare planning, perinatal counseling, and policy-making, as it allows for predictable allocation of resources and sustained monitoring efforts.
Furthermore, our expanded surveillance from 2009 onward indicates that the rates of other major congenital anomalies (e.g., cardiac, limb, chromosomal) have remained constant, which may reflect sustained standards of perinatal and prenatal care in the region. The stable prevalence of other major congenital anomalies from 2009 to 2023 may reflect the consistent quality of perinatal care and prenatal diagnostic practices in the Tokai region. Despite demographic shifts, such as increased maternal age, advances in maternal health management and stable reporting systems likely contributed to the absence of significant temporal changes.
This study has several limitations. First, although the questionnaire response rate has improved, the data still only cover approximately 60% of all births. The study does not include all births in the Tokai region, as only deliveries at responding institutions were captured. Although sensitivity analyses indicate minimal impact on overall incidence estimates, the potential for non-response bias cannot be completely excluded. Additionally, because the cleft types were not diagnosed through direct clinical examination of the patients and were reported based on routine clinical diagnostic practice without standardized definitions (e.g., ICD-11), there may be some uncertainty regarding diagnostic accuracy. In particular, it is possible that minor forms such as submucous CP or soft palate clefts were overlooked, which could have led to a slight underestimation of the true incidence rates. Thus, some degree of misclassification bias cannot be excluded, which represents an inherent limitation of relying on provider-reported questionnaire data. Furthermore, our study is limited by the absence of detailed maternal, socioeconomic, and environmental data, which precludes assessment of potential genetic-environmental interactions influencing CL/P risk.
Nevertheless, the strengths of this study lie in its extensive geographic coverage, including all delivery facilities across the three prefectures of the Tokai region, and its consistent methodology maintained over more than 40 years. As such, it provides one of the most comprehensive and reliable regional CL/P datasets in Japan. We intend to continue this surveillance in the future.
Conclusions
Using data from a sustained 43-year regional surveillance program in Tokai, Japan, this study demonstrates that CL/P incidence has remained stable at approximately 10-20 per 10,000 live births, even amid societal shifts such as rising maternal age and lower birth rates. The observed reversal in CP sex ratio post‑2004 requires additional investigation. This long-term surveillance demonstrates stable CL/P incidence despite demographic shifts, such as declining birth rates and rising maternal age. While these changes occurred concurrently, causal relationships cannot be inferred from the present data. This research underscores the importance of long-term, regionally oriented congenital anomaly monitoring to inform public health planning, genetic counseling strategies, and perinatal care improvements. Ongoing data collection and analysis, ideally including comparisons across other regions and internationally, are strongly encouraged.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cleft lip and palate Lancet Mossey PA Little J Munger RG Dixon MJ Shaw WC 177317853742009 https://www.thelancet.com/journals/lancet/article/PIIS 0140-6736(09)60695-4/abstract 1974772210.1016/S 0140-6736(09)60695-4 · doi ↗ · pubmed ↗
- 2The prevalence, risk of premature births, mortality and causes of death of cleft lip with or without palate in South Korea: a nationwide population-based cohort study Int J Epidemiol Ryu JY Park TH Cho BC Choi KY 9749835120223519080710.1093/ije/dyac 019 · doi ↗ · pubmed ↗
- 3Global prevalence of cleft palate, cleft lip and cleft palate and lip: a comprehensive systematic review and meta-analysis J Stomatol Oral Maxillofac Surg Salari N Darvishi N Heydari M Bokaee S Darvishi F Mohammadi M 11012012320223403394410.1016/j.jormas.2021.05.008 · doi ↗ · pubmed ↗
- 4Cleft lip - a comprehensive review Front Pediatr Shkoukani MA Chen M Vong A 53120132440029710.3389/fped.2013.00053 PMC 3873527 · doi ↗ · pubmed ↗
- 5Cleft lip and palate: understanding genetic and environmental influences Nat Rev Genet Dixon MJ Marazita ML Beaty TH Murray JC 1671781220112133108910.1038/nrg 2933 PMC 3086810 · doi ↗ · pubmed ↗
- 6Incidence of cleft lip and cleft palate in 39,696 Japanese babies born during 1983 Int J Oral Maxillofac Surg Natsune N Kawai T 565568151986 https://www.sciencedirect.com/science/article/abs/pii/S 030097858680059 X 309718110.1016/s 0300-9785(86)80059-x · doi ↗ · pubmed ↗
- 7The prevalence of cleft lip and palate in the Japanese: their birth prevalence in 40,304 infants born during 1982 Oral Surg Oral Med Oral Pathol Natsume N Suzuki T Kawai T 421423631987 https://www.sciencedirect.com/science/article/abs/pii/0030422087902520?via%3Dihub 347214010.1016/0030-4220(87)90252-0 · doi ↗ · pubmed ↗
- 8The prevalence of cleft lip and palate in Japanese Br J Oral Maxillofac Surg Natsume N Suzuki T Kawai T 232236261988 https://www.bjoms.com/article/0266-4356(88)90168-4/abstract 316501910.1016/0266-4356(88)90168-4 · doi ↗ · pubmed ↗