An Unusual Culprit: Staphylococcus capitis Native Mitral Valve Endocarditis Following Scalp Surgery
Silvia Sacramento Azenha, Bhavna Murugesh, Bhiramah Rammanohar, Sani Aliyu

TL;DR
A previously healthy man developed severe heart and spine infections caused by Staphylococcus capitis after scalp surgery, highlighting the need for early diagnosis and treatment.
Contribution
This case report demonstrates that S. capitis can cause native valve endocarditis and discitis in immunocompetent adults.
Findings
S. capitis caused mitral valve endocarditis with leaflet perforation and severe regurgitation.
The infection was complicated by cervical discitis and multiple antibiotic-related adverse effects.
The isolate showed unusual flucloxacillin susceptibility, indicating variable resistance patterns in S. capitis.
Abstract
Staphylococcus capitis is a coagulase-negative Staphylococcus (CoNS) that colonizes the skin, particularly the scalp, and is often dismissed as a blood culture contaminant in the absence of prosthetic material. Reports of invasive adult infections, particularly native valve endocarditis (NVE), are rare. We describe the case of a man in his 50s, previously healthy and with no known cardiac pathology, who presented with a three-week history of night sweats, myalgia, chest discomfort, and severe neck pain. Clinical examination revealed a pansystolic murmur, and five sets of blood cultures were positive for S. capitis. Echocardiography demonstrated large mitral valve vegetations with leaflet perforation and severe regurgitation. MRI revealed cervical discitis. The clinical course was complicated by antibiotic-associated hepatic cholestasis, rash, and thrombocytopenia, necessitating multiple…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
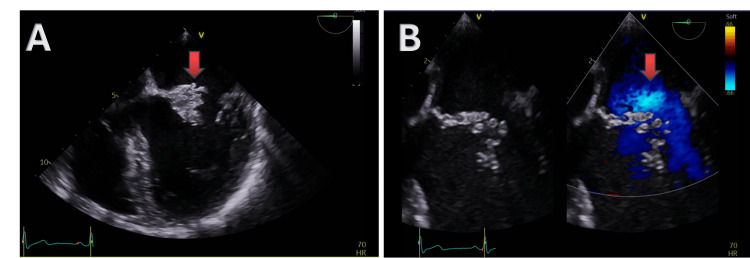 Figure 1
Figure 1 Figure 2
Figure 2| Timeline from admission | Blood culture results |
| Day 1 |
|
| Day 1 |
|
| Day 1 |
|
| Day 2 |
|
| Day 3 |
|
| Antibiotic | Method | Value | Interpretation as per EUCAST |
| Cefoxitin (flucloxacillin inferred from this) | disc | 32 mm | Susceptible |
| Erythromycin | disc | 26 mm | Susceptible |
| Tetracycline | disc | 32 mm | Susceptible |
| Rifampicin | disc | 38 mm | Susceptible |
| Gentamicin | disc | 26 mm | Susceptible |
| Linezolid | disc | 28 mm | Susceptible |
| Clindamycin | disc | 23 mm | Susceptible |
| Co-trimoxazole | disc | 33 mm | Susceptible |
| Ciprofloxacin | disc | 28 mm | Susceptible to increased exposure |
| Vancomycin | E-test MIC | 1.0 mg/L | Susceptible |
| Teicoplanin | E-test MIC | 0.125mg/l | Susceptible |
| Daptomycin | E-test MIC | 0.5 mg/L | Susceptible |
| Timeline from admission | Imaging | Findings |
| Day 5 | Transthoracic Echocardiogram (TTE) | 1.1cm x 1.0cm vegetation on the anterior MV leaflet with regurgitation |
| Day 10 | Transoesophageal Echocardiogram (TOE) | Mitral valve vegetation with anterior leaflet perforation and severe regurgitation |
| Day 13 | CT-TAP and CT-Head | No evidence of septic embolisation |
| Day 15 | MRI Spine | Cervical infective discitis (C5-C6) |
| Day 103 | Transthoracic Echocardiogram (TTE) | EF- 45% and a well-seated mechanical mitral valve replacement with no significant stenosis or regurgitation |
| Haematological parameters | On IV vancomycin | After switching to IV daptomycin |
| White blood cell (WBC) count (3.9 - 10.2 10*9/L ) | 0.6 (L) | 4.4 |
| Red blood cell (RBC) count (4.30 - 5.75 10*12/L ) | 4.61 | 4.34 |
| Hemoglobin (Hb) (135 - 172 g/L ) | 139 | 128 (L) |
| Platelet (PLT) count (150 - 370 10*9/L ) | 63 (L) | 152 |
| Hematocrit (Hct) (0.395 - 0.505 L/L ) | 0.404 | 0.394 (L) |
| Lymphocyte count (1.10 - 4.50 10*9/L ) | 0.42 (L) | 2.28 |
| Basophil count (0.00 - 0.20 10*9/L ) | 0.01 | 0.02 |
| Eosinophil count (0.00 - 0.50 10*9/L ) | 0.02 | 0.22 |
| Monocyte count (0.10 - 0.90 10*9/L ) | 0.01 (L) | 0.31 |
| Neutrophil count (1.50 - 7.70 10*9/L ) | 0.12 (L) | 1.47 (L) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Antimicrobial Resistance in Staphylococcus · Infectious Aortic and Vascular Conditions
Introduction
Staphylococcus capitis is a coagulase-negative Gram-positive cocci that is part of the normal flora of human skin, mainly the scalp and chin, and is usually regarded as a contaminant in the context of a positive blood culture in the absence of prosthetic material [1]. Recently, however, both adult and neonatal S. capitis infections have gained attention. Outbreaks of S. capitis in neonatal intensive care units have highlighted its subacute presentation in late-onset sepsis and significant antimicrobial resistance to most drug classes [2]. Limited literature describes adult infections with S. capitis, especially cases of native valve endocarditis (NVE). One case report has described prosthetic valve S. capitis endocarditis after a scalp laceration [3]. Of the 12 cases of S. capitis NVE cases reported, only one occurred in a patient with native valves in the absence of predisposing comorbidities or cardiac pathology [4]. In this case report, we present a rare case of S. capitis-associated NVE without established risk factors, following a scalp procedure.
Case presentation
History and examination
A man in his 50s, previously well, presented with a three-week history of night sweats, myalgia, chest discomfort, and progressive neck pain. He denied recent dental procedures or intravenous drug use. Ten months earlier, he had undergone excision of a benign scalp lesion. On examination, he was afebrile with stable vital signs. Cardiovascular examination revealed a grade III/VI pansystolic murmur radiating to the axilla, with no clinical signs of heart failure. Neurological examination was unremarkable.
Investigations
On admission, the C-reactive protein was 122 mg/L, the white cell count was 10.4 × 10⁹/L, and neutrophils were 7.9 × 10⁹/L. Three sets of blood cultures grew Gram-positive cocci in clusters, subsequently identified as *S. capitis *by matrix-assisted laser desorption/ionization-time-of-flight mass spectrometry (MALDI-TOF), a standard diagnostic technique freely used in clinical microbiology laboratories. Blood culture timeline and results are outlined in Table 1, and the antibiotic susceptibility testing of the first blood culture is detailed in Table 2. The isolate demonstrated cefoxitin susceptibility, indicating methicillin sensitivity and, by inference, susceptibility to flucloxacillin as per European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidance [5]. Disc susceptibility interpretation was similar across all five blood culture sets.
Transoesophageal echocardiography performed on day 10 demonstrated mitral valve vegetations involving both the anterior and posterior leaflets. The anterior leaflet had a 2.1 × 2.2 cm vegetation with a 1.2 cm mobile filament, while the posterior leaflet was thickened with a 0.7 × 1.2 cm mobile vegetation. There was also evidence of anterior leaflet perforation with severe mitral valve regurgitation (Figure 1). In view of persistent neck pain, an MRI of the whole spine was performed on day 15 to evaluate for possible spinal involvement, which revealed findings consistent with cervical infective discitis at the C5-C6 level (Figure 2). Imaging findings are summarized in Table 3. According to the 2023 Duke-International Society for Cardiovascular Infectious Diseases (ISCVID) criteria, this case meets the definition of definite infective endocarditis, based on repeated isolation of a nontypical organism (Staphylococcus capitis) from multiple blood culture sets and echocardiographic evidence of mitral valve vegetations with leaflet perforation and severe regurgitation [6].
Transoesophageal echocardiogram (TOE) demonstrating mitral valve involvement.A: large vegetation on the anterior mitral valve leaflet (red arrow); B: color Doppler showing severe mitral regurgitation (red arrow).
Magnetic resonance imaging (MRI) of the cervical spine showing infective discitis at C5–C6 (red arrow).
Treatment course
Initial empirical antibiotics (amoxicillin and ceftriaxone) were changed to vancomycin after MALDI-TOF identification, and subsequently to flucloxacillin after susceptibility testing. On day five, clearance of the organism in blood cultures was achieved. Flucloxacillin was discontinued due to obstructive cholestasis, with liver function tests showing alanine aminotransferase (ALT) 267 IU/L (reference range 40-50 IU/L) and alkaline phosphatase (ALP) 202 IU/L (reference range 30-130 IU/L). The patient was then switched back to vancomycin (minimum inhibitory concentration (MIC) 1.0 mg/L). However, this was complicated by a blanching rash, neutropenia, and thrombocytopenia, which were thought to be induced by vancomycin. Therapy was subsequently changed to intravenous daptomycin. Following this, an improvement in cell counts was observed (Table 4).
Outcome
The patient was transferred to the regional cardiothoracic center on day 32 of admission and underwent mechanical mitral valve replacement the following day. He completed 47 days of intravenous daptomycin and was discharged on oral linezolid for seven days. Enriched heart valve cultures were sent and did not demonstrate any growth. At the two-month follow-up, echocardiography showed improved ejection fraction (from 30-35% to 45%) and a well-seated mechanical mitral valve replacement with no significant stenosis or regurgitation. A gradual improvement in neck pain was also noted.
Discussion
Repeated isolation of coagulase-negative Staphylococcus (CoNS) from blood cultures can represent a range of possibilities, including true infective endocarditis, catheter- or device-related infection, transient bacteremia, or simple contamination [1]. Differentiating these is essential, as CoNS are frequent skin commensals. In this patient, the absence of intravascular or prosthetic material, together with consistent clinical findings and echocardiographic evidence, supported the diagnosis of true NVE. In a large multicenter cohort study, coagulase-negative staphylococci accounted for approximately 12% of native valve infective endocarditis cases [7].
The European Society of Cardiology (ESC), American Heart Association (AHA), and National Institute for Health and Care Excellence (NICE) guidelines place emphasis on common pathogens associated with infective endocarditis, such as Staphylococcus aureus [8-10]. Coagulase-negative staphylococci, known for their biofilm formation and indolent course, are primarily discussed in the context of prosthetic valve endocarditis, with less focus on native valve infections. They can also infect other indwelling devices such as pacemaker leads, vascular grafts, central lines, and orthopedic implants, where biofilm formation facilitates persistent infection. Because these organisms are often associated with prosthetic material, *S. capitis *isolated from blood cultures may be mistakenly regarded as a contaminant in patients without such devices, leading to potential diagnostic delays [1,2].
This case highlights the significance of considering S. capitis as a cause of infective endocarditis affecting native heart valves, with potential complications including valve perforation and secondary infections, such as discitis. Systemic complications described in the literature also include vertebral osteomyelitis, meningitis, prosthetic joint infections, prosthetic valve endocarditis, and late-onset neonatal sepsis. Hematogenous spread has been implicated in device-related infections, intravascular catheter sepsis, and endovascular involvement such as pacemaker lead and prosthetic graft infections [1,2,4]. These reports demonstrate the organism’s potential for persistence and dissemination through biofilm formation on foreign materials, although this was not the underlying mechanism in our patient, who had no prosthetic devices.
A key learning point was the initial delay in echocardiography, as the organism was initially disregarded as a contaminant. This reflects the evolving concept of infective endocarditis as a time-sensitive diagnosis, where early echocardiography may help avoid diagnostic delay and prevent advanced complications [11].
Interestingly, the S. capitis isolate in this case was susceptible to flucloxacillin, which is uncommon given the high prevalence of methicillin resistance among coagulase-negative staphylococci due to mecA gene carriage [5].
Despite flucloxacillin being appropriate in this case, treatment was complicated by drug-induced obstructive cholestasis followed by a rash and thrombocytopenia, probably due to vancomycin. This underscores the need for vigilance and monitoring for drug toxicity when treating infective endocarditis.
As far as we know, previously reported cases of S. capitis NVE were associated with comorbidities or underlying valvular abnormalities such as mitral valve prolapse or bicuspid aortic valve [4]. In contrast, our patient had no known past medical history or structural heart disease, with the recent scalp procedure being the only identifiable risk factor and likely portal of entry for S. capitis bacteremia [12]. Colley et al. similarly reported S. capitis endocarditis following a scalp procedure; however, that case occurred in a patient with a prosthetic valve [3].
There was no growth in the enriched culture from the valve tissue, likely due to the patient having already received more than four weeks of antibiotics by that time. Although a broad-range 16S rDNA polymerase chain reaction (PCR) on the native valve would have been valuable in confirming S. capitis as the causative organism [13], the repeated isolation of the same organism in five initial blood cultures provided strong evidence in our case.
Conclusions
*Staphylococcus capitis *can cause severe native mitral valve endocarditis with complications such as discitis, even in immunocompetent adults without comorbidities. Prior skin procedures may represent a risk factor. Clinicians should be cautious not to dismiss S. capitis as a contaminant when it is repeatedly isolated in blood cultures in patients with clinical features of infective endocarditis.
Prompt echocardiography is recommended to avoid diagnostic delays. This case underscores the need for vigilance in interpreting the significance of coagulase-negative staphylococci when repeatedly isolated in blood cultures, the variability of antimicrobial susceptibility, and the importance of supporting investigations to enable early and tailored therapy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Determining the clinical significance of coagulase-negative staphylococci isolated from blood cultures Infect Control Hosp Epidemiol Beekmann SE Diekema DJ Doern GV 5595662620051601843210.1086/502584 · doi ↗ · pubmed ↗
- 2Methicillin-resistant Staphylococcus capitis with reduced vancomycin susceptibility causes late-onset sepsis in intensive care neonates P Lo S One Rasigade JP Raulin O Picaud JC 07201210.1371/journal.pone.0031548 PMC 327940222348102 · doi ↗ · pubmed ↗
- 3Prosthetic valve endocarditis developing after an infected scalp laceration J Emerg Med Colley JL Nolan SP Edlich RF 26927431985409357910.1016/0736-4679(85)90430-5 · doi ↗ · pubmed ↗
- 4Native and prosthetic valve Staphylococcus capitis endocarditis: a review of the literature Cardiol Res Thakker RA Chatila K Reynoso D Karnath B 1401451220213404610610.14740/cr 1231 PMC 8139748 · doi ↗ · pubmed ↗
- 5Evaluation of surrogate tests for the presence of mec A-mediated methicillin resistance in Staphylococcus capitis, Staphylococcus haemolyticus, Staphylococcus hominis, and Staphylococcus warneri J Clin Microbiol Humphries RM Magnano P Burnham CA Dien Bard J Dingle TC Callan K Westblade LF 02059202010.1128/JCM.02290-20PMC 777143433115842 · doi ↗ · pubmed ↗
- 6The 2023 Duke-International Society for Cardiovascular Infectious Diseases Criteria for Infective Endocarditis: updating the Modified Duke Criteria Clin Infect Dis Fowler VG Durack DT Selton-Suty C 5185267720233713844510.1093/cid/ciad 271PMC 10681650 · doi ↗ · pubmed ↗
- 7Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohort Study Arch Intern Med Murdoch DR Corey GR Hoen B 46347316920091927377610.1001/archinternmed.2008.603PMC 3625651 · doi ↗ · pubmed ↗
- 82023 ESC Guidelines for the management of endocarditis: developed by the task force on the management of endocarditis of the European Society of Cardiology (ESC) Endorsed by the European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Nuclear Medicine (EANM)Eur Heart J Delgado V Ajmone Marsan N de Waha S 39484042442023 https://doi.org/10.1093/eurheartj/ehad 1933773832210.1093/eurheartj/ehad 625 · doi ↗ · pubmed ↗