Incidental Discovery of a Duplicated Ovary During Surgery for Acute Appendicitis in an Adolescent
Kyriakos Apostolidis, Chrysovalantis Mariorakis, Christos Voskidis, Vasiliki Magaliou, Ioannis Gogoulis, Maria Petridou, Maria Piagkou, George Triantafyllou, Christos Lyrtzis, Ioannis Georgakis

TL;DR
A 13-year-old girl had a duplicated ovary discovered during surgery for suspected appendicitis, highlighting the need for thorough intraoperative exploration in adolescents with abdominal pain.
Contribution
This case adds to the rare documentation of ovarian duplication and emphasizes the importance of interdisciplinary collaboration during pediatric abdominal surgeries.
Findings
A duplicated right ovary was incidentally identified during an appendectomy in a 13-year-old girl.
The patient had an uneventful recovery after the appendectomy and intraoperative evaluation of the genitalia.
The case underscores the limitations of preoperative imaging in identifying rare anatomical anomalies.
Abstract
Acute right lower quadrant abdominal pain in adolescent women commonly raises suspicion for appendicitis; however, the differential diagnosis must also include gynecologic causes. Rare congenital anomalies can complicate the clinical picture and lead to unexpected intraoperative findings. We report the case of a 13-year-old girl presenting with right iliac fossa pain and minimal clinical signs. Laboratory and imaging studies supported a diagnosis of acute appendicitis. During an appendectomy, a duplicated right ovary was incidentally identified - an extremely rare anatomical anomaly with fewer than 30 cases documented in the literature. The appendectomy was completed, the internal genitalia were evaluated and repositioned anatomically, and the patient had an uneventful postoperative course, being discharged within 48 hours. Ovarian duplication is a rare embryologic anomaly that is…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
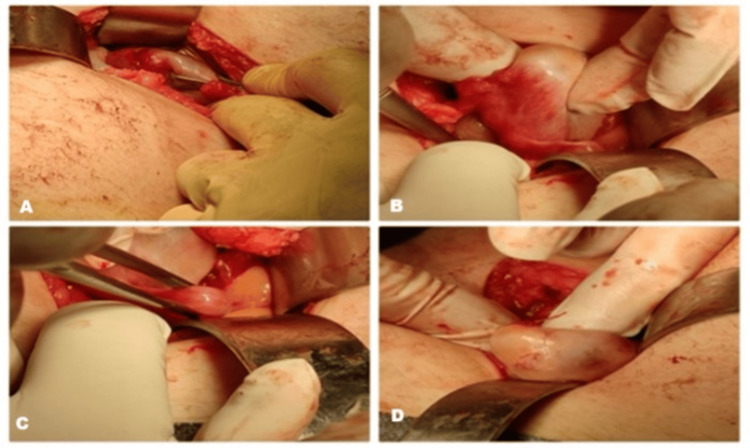 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAppendicitis Diagnosis and Management · Intraperitoneal and Appendiceal Malignancies · Intestinal and Peritoneal Adhesions
Introduction
Acute pain in the right lower quadrant of the abdomen among adolescent women is a common yet diagnostically challenging presentation in both pediatric and emergency medical settings. While acute appendicitis remains one of the most prevalent causes of surgical abdomen in this demographic group, gynecologic etiologies - such as ovarian torsion, ruptured ovarian cyst, pelvic inflammatory disease, or congenital anomalies - must also be considered owing to their overlapping symptoms and proximity of affected structures [1]. Among these rare conditions, ovarian duplication - which encompasses both supernumerary ovaries and accessory ovaries - represents an extraordinarily uncommon congenital anomaly. Its estimated incidence varies from one in 29,000 to 700,000, with fewer than 40 cases of supernumerary ovaries documented in the literature to date [2-4]. Ectopic ovaries are entirely distinct from normal adnexa and possess their own vascular supply, whereas accessory (or supernumerary) ovaries are situated anatomically adjacent and may share structural or vascular connections [2-4]. These anomalies are sometimes associated with other congenital malformations involving the Müllerian ducts or urinary tract [5]. Clinically, they are often asymptomatic and discovered incidentally during imaging or surgical procedures, but may also present with pain, torsion, mass effect, or neoplastic transformation [4,6]. The preoperative diagnosis of ovarian duplication remains notably challenging. Although ultrasonography serves as the initial imaging modality in pediatric and adolescent populations due to its availability and safety, it may lack sufficient resolution to detect such rare anomalies [7]. Even advanced imaging modalities such as magnetic resonance imaging (MRI), which offer higher sensitivity for soft tissue characterization, may misinterpret supernumerary ovarian tissue as atypical cysts or adrenal lesions [4,7]. This underscores the importance of systematic intraoperative assessment, particularly during laparoscopic procedures in female adolescents.
Case presentation
A 13-year-old girl of Ukrainian descent was transferred from a provincial hospital to the Emergency Department of a tertiary care facility due to progressive right iliac fossa pain that commenced in the morning and intensified throughout the day. The pain was associated with nausea but was not accompanied by fever, vomiting, or bowel disturbances. Her medical history was notable for a COVID-19 infection one month prior, following which she experienced intermittent palpitations and retrosternal tightness.
On examination, the abdomen was soft but tender over the right iliac fossa and lower abdomen. Laboratory investigations revealed mildly elevated inflammatory markers (C-reactive protein (CRP), 1.66 mg/dL) and increased neutrophils (11,200/μL; 81.8%). An abdominal X-ray demonstrated significant aeroplegia, which improved after the administration of glycerin suppositories. However, due to persistent localized tenderness, an abdominal and pelvic ultrasound was performed, which demonstrated findings consistent with acute appendicitis. Given these results, the patient was scheduled for surgery. An open laparoscopy was performed due to the unavailability of the laparoscopic tower during multiple simultaneous emergency cases. Following a routine appendectomy, a systematic intraoperative inspection of the pelvic organs revealed a mass adjacent to the right ovary. Initially suspected to be an ovarian cyst, its location and morphology were atypical. Intraoperative gynecological consultation confirmed the presence of a duplicated right ovary (Figure 1) - a rare anomaly with very limited descriptions in the literature.
Intraoperative findings of a duplicated right ovary.Intraoperative images demonstrating the discovery of a duplicated right ovary in a 13-year-old girl undergoing appendectomy. (A) Exposure of the pelvic cavity after appendectomy, showing the adnexal region. (B) Identification of an additional adnexal structure adjacent to the right ovary. (C) Careful mobilization of the duplicated ovary using atraumatic forceps. (D) Final inspection confirming the presence of two anatomically distinct right ovaries without evidence of torsion or cystic change.
The internal genitalia were repositioned into normal anatomical alignment without further intervention, and the procedure was completed. The patient’s postoperative recovery was uneventful, and she was discharged on the second postoperative day. A follow-up examination on the 10th postoperative day showed no abnormalities or complications.
The patient provided informed consent to anonymously publish the data. The research was conducted ethically following the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Discussion
The differential diagnosis of acute abdominal pain in adolescent women is extensive, encompassing both gastrointestinal and gynecologic conditions. Appendicitis remains the predominant cause of surgical abdomen in this demographic group. Still, gynecologic etiologies such as ovarian torsion, cyst rupture, and pelvic inflammatory disease must also be considered due to their anatomical proximity and overlapping symptomatology [8].
In this case, the clinical findings were most consistent with acute appendicitis, as evidenced by localized tenderness in the right iliac fossa, mildly elevated inflammatory markers, and ultrasonographic signs of appendiceal inflammation. However, the intraoperative discovery of a duplicated right ovary introduced a scarce diagnostic consideration. Ovarian duplication, also known as a supernumerary ovary, is a congenital anomaly with fewer than 40 documented cases worldwide [9]. It is essential to distinguish between ectopic and supernumerary ovaries. An ectopic ovary is entirely separate from the normal adnexa and has its own vascular supply, whereas supernumerary ovary remains structurally or vascularly connected to the native ovary. In our case, the duplicated structure was adjacent but anatomically distinct from the right ovary, suggesting a supernumerary ovary; however, definitive classification would require histological and vascular studies [10-13].
The embryological basis of ovarian duplication remains uncertain; however, the most widely accepted explanation is an abnormal division of the gonadal ridge during embryogenesis, resulting in the formation of additional ovarian tissue. While many cases are asymptomatic and discovered incidentally, complications including torsion, cyst formation, and neoplastic transformation have been described. For instance, Lim et al. [14] reported two concurrent dermoid cysts in an accessory and an ectopic ovary, demonstrating that ectopic ovarian tissue retains malignant potential. Similarly, Zon et al. [15] described a dermoid cyst in an accessory ovary in Thailand, reinforcing this risk.
From a diagnostic standpoint, this case illustrates the limitations of preoperative imaging in identifying rare anomalies. Ultrasound remains the first-line imaging modality in adolescents because of its safety and accessibility, but its resolution is often inadequate for detecting ectopic ovarian tissue. Magnetic resonance imaging (MRI) offers superior soft tissue characterization and, in some reports, has revealed cord-like structures and follicle-like features suggestive of ectopic ovarian tissue. For example, Wang et al. [11] described a fourth supernumerary ovary in the hepatorenal space, which mimicked an adrenal pheochromocytoma on MRI, demonstrating how such anomalies can masquerade as extra-pelvic masses [11,12].
Another consideration is the association between ovarian duplication and congenital anomalies. Zhigang and Wenlu [13] reported an intrarenal supernumerary ovary with concurrent renal pelvis and ureteral duplication, suggesting a shared embryologic pathway for urogenital development. Other studies have described coexisting Müllerian anomalies, endometriosis, and ectopic ovarian tissue in unusual sites such as the rectosigmoid colon [16].
Our patient’s postoperative recovery was uneventful, and the duplicated ovary was left in situ, given the absence of symptoms or complications. However, long-term follow-up is warranted, as the reproductive and gynecological implications remain uncertain [13].
The main strength of this case lies in its documentation of a rare instance of ovarian duplication in an adolescent, thereby contributing to the limited existing literature. It emphasizes the importance of systematic intraoperative exploration in female patients undergoing appendectomy, highlighting the role of interdisciplinary collaboration between pediatric surgeons and gynecologists. An additional strength is the inclusion of a comprehensive literature review, which situates this case within a broader clinical context.
However, several limitations should be acknowledged. As with most case reports, the findings are based on a single patient and therefore lack generalizability. Moreover, histological analysis was not performed, preventing a definitive distinction between a supernumerary and an accessory ovary. The absence of advanced preoperative imaging, such as MRI, limited diagnostic precision, though this reflects the constraints of an emergency surgical setting. Finally, the lack of long-term follow-up data precludes conclusions regarding the patient’s future reproductive and gynecological outcomes.
Conclusions
This case stresses the importance of maintaining an expansive differential diagnosis when evaluating adolescent patients presenting with acute abdominal pain, as both gastrointestinal and gynecologic causes must be considered. Although imaging is integral to diagnosis, its limitations in identifying rare congenital anomalies such as ovarian duplication highlight the necessity of thorough intraoperative examination. The incidental identification of a duplicated right ovary during an appendectomy underscores the significance of systematic pelvic evaluation in adolescent women and illustrates the critical need for interdisciplinary cooperation between pediatric surgeons and gynecologists. Current literature also suggests that duplicated ovaries may be found in extrapelvic regions, be associated with other congenital anomalies, and possess potential for neoplastic transformation. These observations underscore the importance of diligent intraoperative vigilance and, when appropriate, long-term clinical follow-up. By documenting this case and reviewing existing literature, we contribute to the relatively limited yet expanding body of knowledge concerning ovarian duplication, thereby providing clinicians with additional insights for managing similar rare intraoperative findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Does this child have appendicitis?JAMA Bundy DG Byerley JS Liles EA Perrin EM Katznelson J Rice HE 43845129820071765229810.1001/jama.298.4.438PMC 2703737 · doi ↗ · pubmed ↗
- 2Two cases of supernumerary ovary and one of accessory ovary, with an analysis of previously reported cases Am J Obstet Gynecol Wharton LR 110111197819591384425610.1016/s 0002-9378(16)36660-1 · doi ↗ · pubmed ↗
- 3Supernumerary ovaries: update and review Obstet Gynecol Cruikshank S Van Drie D 126128601982 https://journals.lww.com/greenjournal/citation/1982/07000/supernumerary_ovaries__update_and_review.27.aspx 7088444 · pubmed ↗
- 4The ectopic ovary. A case report and review of the literature Arch Pathol Lab Med Lachman MF Berman MM 2332351151991 https://pubmed.ncbi.nlm.nih.gov/2001159/2001159 · pubmed ↗
- 5Supernumerary ovary. A case report J Reprod Med Harlass F Magelssen D Soisson AP 459461321987 https://pubmed.ncbi.nlm.nih.gov/3612636/3612636 · pubmed ↗
- 6Supernumerary ovary: a case report and literature review J Obstet Gynaecol Litos MG Furara S Chin K 3253272320031291850710.1080/01443610310000106055 · doi ↗ · pubmed ↗
- 7A case of supernumerary ovary Obstet Gynecol Lee B Gore B 738740641984 https://journals.lww.com/greenjournal/abstract/1984/11000/a_case_of_supernumerary_ovary.30.aspx?casa_token=pm EM 3i 4l 8IIAAAAA:F 8BNNQAN 2C Lm KD Qa-_f F Kr FYE Dvlws U 3Z Vziqt JW Zd Y Hza R 04Zg Y 8Cn Jsk 8Gjo U Vsg 3q Kr 09nu 9Ybb 6Vc O 68GR Eujf Oz OA Svbgw 46238253 · pubmed ↗
- 8Evaluation of the adolescent female with acute lower abdominal pain Clin Pediatr Emerg Med Bean JF Rowell E 243247152014 https://www.sciencedirect.com/science/article/abs/pii/S 1522840114000573?via%3Dihub