Pulmonary Melioidosis Masquerading As Tuberculosis: A Case Report Presenting a Rare Medical Condition From Western India
Naineesh Gaikwad, Prachee A Makashir, Rohan Kelkar, Virendra Prasad Singh, Vrushali Thakar

TL;DR
A case of melioidosis in Western India was mistaken for tuberculosis, showing the need for accurate testing to distinguish these diseases.
Contribution
This case report highlights the diagnostic challenge of differentiating melioidosis from tuberculosis in endemic regions.
Findings
The patient's symptoms and imaging resembled pulmonary tuberculosis but were caused by melioidosis.
Microbiological confirmation was crucial for accurate diagnosis and treatment.
Melioidosis can present similarly to TB, leading to potential misdiagnosis without proper testing.
Abstract
A young adult from a rural region of Western India developed a two-week history of intermittent fever with evening temperature spikes, dry cough, and systemic symptoms, highlighting a clinical scenario frequently encountered in endemic areas. Examination revealed crackles on the left side of the chest. Investigations revealed thrombocytopenia, mild transaminitis, and bilateral pulmonary infiltrates on chest X-ray. High-resolution computed tomography of the chest showed cavitary consolidation resembling pulmonary tuberculosis (TB), but bronchoalveolar lavage was negative for TB. Despite empirical antibiotics, the patient remained febrile. On the sixth day since admission, blood culture identified Burkholderia pseudomallei, confirming melioidosis bacteremia. In an endemic TB setting, this case highlights the diagnostic challenge between TB and melioidosis and underlines the importance of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
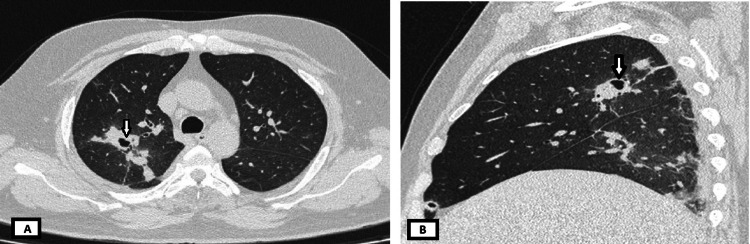 Figure 1
Figure 1 Figure 2
Figure 2| Test | Day 1 | Day 3 | Day 4 | Day 6 | Normal value |
| Hemoglobin (g/dL) | 12.6 | 13.6 | 12.6 | 11.9 | 13.2-17.5 |
| Platelet count (/mm3) | 44,000 | 90,000 | 151,000 | 351,000 | 150,000-350,000 |
| Total leucocyte count (/mm3) | 9,100 | 13,400 | 12,200 | 16,100 | 5,000-11,000 |
| Test | Day 1 | Day 9 | Normal value |
| Urea (mg/dL) | 25 | - | 17.9-54.9 |
| Creatinine (mg/dL) | 0.73 | - | 0.73-1.18 |
| Total bilirubin (mg/dL) | 1.0 | - | 0.3-1.2 |
| Aspartate aminotransferase (U/L) | 63 | 59 | <35 |
| Alanine aminotransferase (U/L) | 69 | 61 | <45 |
| Serum globulin (g/dL) | 2.8 | - | 6.4-8.3 |
| Serum albumin (g/dL) | 3.1 | - | 3.5-5.2 |
| Inflammatory markers | |||
| Erythrocyte sedimentation rate (mm/hour) | 73 | 98 | 0-20 |
| C-reactive protein (mg/dL) | 100.5 | 40.4 | <5 |
| Serum ferritin (ng/mL) | 4,349 | - | 20-500 |
| Antimicrobial | MIC | Interpretation |
| Ceftazidime | ≤4 | S |
| Piperacillin-tazobactam | ≤4 | R |
| Cefoperazone-sulbactam | ≤8 | S |
| Cefepime | 16 | R |
| Meropenem | 1 | S |
| Amikacin | ≥64 | R |
| Gentamicin | ≥16 | R |
| Ciprofloxacin | 2 | I |
| Cotrimoxazole (trimethoprim-sulfamethoxazole) | ≤20 | S |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBurkholderia infections and melioidosis · Chemical Looping and Thermochemical Processes · Subcritical and Supercritical Water Processes
Introduction
Melioidosis is a potentially fatal infectious disease caused by Burkholderia pseudomallei that primarily affects individuals in tropical and subtropical regions. The approximate worldwide occurrence of melioidosis is 165,000 cases and 89,000 deaths annually [1]. Recent environmental and clinical studies have highlighted a notable presence of melioidosis in India. In India, most cases have been reported from the southern states [2]. The growing epidemic of diabetes, a major risk factor, may contribute to an increase in melioidosis cases in the country. Melioidosis often resembles tuberculosis (TB) and is uncommonly suspected, making awareness crucial [3]. Humans are infected through direct contact with contaminated water or soil. The disease presents with a wide range of symptoms, including fever, pain, and organ-specific complications, often mimicking other common infections [4].
The clinical spectrum of melioidosis is highly variable, ranging from localized skin infections to pneumonia, sepsis, and multiorgan abscess formation [5]. Pulmonary involvement is particularly common and may mimic TB, presenting with fever, cough, weight loss, and cavitary lesions on imaging [6]. Such overlap in clinical presentation frequently leads to misdiagnosis in regions where TB is endemic, delaying appropriate therapy and increasing morbidity and mortality [7].
Several risk factors, such as diabetes mellitus, chronic kidney disease, chronic lung disease, immunosuppressive therapy, and excessive alcohol consumption, predispose individuals to severe disease [8]. However, melioidosis can also affect immunocompetent individuals, though less frequently, accounting for up to 20% of cases [5]. This underscores the significance of our case, as it highlights pulmonary melioidosis in an individual with no underlying risk factors, masquerading as TB, in a region of India where awareness remains low. Early recognition in such atypical hosts is crucial to prevent delays in initiating appropriate therapy.
Case presentation
A 32-year-old man, a farmer from Western Maharashtra, presented with a history of intermittent fever with evening temperature spikes for the past two weeks. He also reported a nonproductive cough, anorexia, generalized weakness, and body pain for eight days. There was no history of dysuria, arthralgia, rash, diarrhea, or weight loss. He had no prior comorbid medical conditions.
On examination, the patient had a temperature of 40.1°C, a heart rate of 110 beats per minute, a blood pressure of 124/76 mmHg, a respiratory rate of 26 breaths per minute, and an oxygen saturation of 97% on room air. On general examination, palpable lymphadenopathy was noted, and systemic examination of the chest revealed crackles in the left mammary and interscapular areas.
Initial investigations revealed thrombocytopenia (Table 1). The liver panel showed transaminitis, and inflammatory markers were raised (Table 2). These test results suggested an evolving systemic infection. Serological and antigen-based tests for common tropical infections, including typhoid fever (Typhoid IgM), dengue (NS1 antigen), malaria, rickettsial infections, and salmonellosis, were negative. Chest X-ray showed bilateral patchy infiltrates in the mid and lower zones, suggestive of infective pulmonary lesions. The patient was started on empirical intravenous ceftriaxone in view of persistent fever.
High-resolution computed tomography of the thorax revealed cavitary consolidation in the apical and anterior segments of the right upper lobe, highly suggestive of pulmonary TB (Figure 1). Bronchoscopy was subsequently performed for microbiological confirmation; however, bronchoalveolar lavage fluid culture and GeneXpert results were negative for Mycobacterium tuberculosis.
High-resolution computed tomography images of the thorax showing cavitary lesions with surrounding consolidation(A) Axial view. (B) Sagittal view
On the sixth day of hospitalization, given the diagnostic uncertainty and persistent fever despite empirical therapy, a clinical dilemma arose whether to escalate to broader spectrum antibiotics. At this time, blood culture results became available and grew B. pseudomallei, thereby confirming the diagnosis of melioidosis bacteremia (Figure 2).
Blood culture showing growth of Burkholderia pseudomallei
The antibiotic sensitivity report revealed sensitivity to ceftazidime, cefoperazone-sulbactam, meropenem, and trimethoprim-sulfamethoxazole (Table 3). Ceftazidime was selected for the intensive phase treatment based on proven efficacy and cost-effectiveness. The patient clinically improved after treatment with intravenous ceftazidime for two weeks. At the time of discharge, he was advised oral trimethoprim/sulfamethoxazole for three months as an eradication phase to reduce the chances of relapse.
Discussion
Melioidosis was first discovered by Whitmore and Krishnaswami in Myanmar and is also known as Whitmore's disease [9]. It is caused by a Gram-negative bacterium that is endemic across tropical countries, especially Southeast Asia and Northern Australia [5]. Infection is acquired by inoculation, ingestion, or inhalation of aerosols by coming in contact with contaminated soil and water [10].
Melioidosis is often underdiagnosed due to its diverse clinical manifestations and nonspecific symptoms, frequently mimicking TB, typhoid fever, or pneumonia [7,11]. Pulmonary melioidosis presents with fever, cough, and cavitary lesions, which may lead clinicians in endemic regions to empirically initiate anti-tubercular therapy, delaying appropriate management [6,7]. In our case, the patient’s persistent fever, elevated total leukocyte count, and organ-specific complications prompted a broad investigation. However, the diagnosis was not established until the blood culture yielded Burkholderia pseudomallei. This highlights the importance of considering melioidosis in the differential diagnosis of febrile illnesses in endemic regions, particularly when other common infections have been ruled out.
Although diabetes and immunocompromised states (chronic kidney disease, alcoholism, liver cirrhosis, chronic lung disease, hematological disorders, a history of splenectomy, or neutropenia) are commonly associated with melioidosis, individuals without underlying risk factors can also develop severe disease, as was illustrated in our patient [5]. Melioidosis exhibits a wide clinical spectrum, ranging from rapidly progressive, fulminant sepsis that can be fatal within days to slower, subacute illness with multiple abscesses in the lungs, liver, spleen, bones, and soft tissues. Chronic forms may persist for months to years, often presenting with indolent abscesses that mimic TB, fungal infections, or malignancy. The infection can also remain latent and asymptomatic for years, with reactivation occurring under conditions of immune compromise such as trauma, burns, diabetes, malignancy, or immunosuppressive therapy [12].
Diagnosis primarily relies on the culture of blood, pus, or other clinical specimens [13]. Molecular methods such as PCR and serology can support rapid detection but are not widely available [14]. Early recognition and prompt initiation of appropriate antimicrobial therapy are critical, as mortality rates for septicemic melioidosis can reach 50% [7]. In the intensive phase, intravenous antibiotic therapy with ceftazidime, meropenem, or imipenem is administered for 10-14 days. This is followed by a prolonged oral eradication phase with trimethoprim-sulfamethoxazole for three to six months to prevent relapse [13]. Inadequate treatment increases the risk of recurrence, emphasizing adherence to the full therapeutic regimen [15].
This case demonstrates that melioidosis should be considered in febrile patients with pulmonary lesions, even in individuals with no comorbidities, especially when TB is suspected but microbiology is negative.
Conclusions
Melioidosis is an emerging infectious disease in India that often presents with nonspecific systemic symptoms and pulmonary findings closely resembling TB, leading to frequent misdiagnosis and inappropriate therapy. This case highlights the need for clinicians practicing in endemic regions such as Western India to maintain a high index of suspicion for melioidosis, particularly in patients with chronic febrile illness, poor response to anti-tubercular therapy, or risk factors such as diabetes and occupational exposure to soil or surface water. Early microbiological confirmation through culture and appropriate antimicrobial therapy is essential for effective management and improved outcomes. Greater clinical awareness, timely diagnosis, and inclusion of melioidosis in the differential diagnosis of TB-like presentations are critical steps toward reducing morbidity and mortality associated with this underrecognized infection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Melioidosis: emerging beyond endemic areas Nursing Borton D 293452202210.1097/01.NURSE.0000872460.50198.3936129502 · doi ↗ · pubmed ↗
- 2Melioidosis in India and Bangladesh: a review of case reports Asian Pac J Trop Med Tipre M Kingsley PV Smith T Leader M Sathiakumar N 320329112018
- 3The epidemiology and clinical spectrum of melioidosis: 540 cases from the 20 year Darwin prospective study P Lo S Negl Trop Dis Currie BJ Ward L Cheng AC 04201010.1371/journal.pntd.0000900 PMC 299491821152057 · doi ↗ · pubmed ↗
- 4Human melioidosis caused by novel transmission of Burkholderia pseudomallei from freshwater home aquarium, United States Emerg Infect Dis Dawson P Duwell MM Elrod MG 303030352720213457069310.3201/eid 2712.211756 PMC 8632198 · doi ↗ · pubmed ↗
- 5Melioidosis Nat Rev Dis Primers Wiersinga WJ Virk HS Torres AG Currie BJ Peacock SJ Dance DA Limmathurotsakul D 17107420182938857210.1038/nrdp.2017.107PMC 6456913 · doi ↗ · pubmed ↗
- 6Clinical features and epidemiology of melioidosis pneumonia: results from a 21-year study and review of the literature Clin Infect Dis Meumann EM Cheng AC Ward L Currie BJ 3623695420122205770210.1093/cid/cir 808PMC 3258273 · doi ↗ · pubmed ↗
- 7Burden of melioidosis in India and South Asia: challenges and ways forward Lancet Reg Health Southeast Asia Mohapatra PR Mishra B 100004220223738329510.1016/j.lansea.2022.03.004PMC 10306050 · doi ↗ · pubmed ↗
- 8Melioidosis in critical care: a review Indian J Crit Care Med Sridharan S Princess IB Ramakrishnan N 0525202110.5005/jp-journals-10071-23837 PMC 832779534345132 · doi ↗ · pubmed ↗