Acute Pericarditis After Percutaneous Coronary Intervention
Ahmed Smman, Infanta Raffael

TL;DR
A patient developed pericarditis after a heart procedure and required multiple treatments over weeks to manage recurring symptoms.
Contribution
This case report highlights pericarditis as a rare but important complication following PCI.
Findings
Pericarditis occurred after PCI for STEMI and presented with chest pain and fever.
The patient required multiple hospitalizations and a combination of medications for management.
Colchicine and steroid therapy were used to manage recurrent pericarditis episodes.
Abstract
Pericarditis may be a complication of percutaneous coronary intervention (PCI), and should be considered as a differential for persistent chest pain following a PCI. In this report, we present a male in his 60s, who developed pericarditis after a primary PCI for an anterior ST elevation myocardial infarction (STEMI). He had an uncomplicated PCI to left anterior descending artery, and was discharged as per standard procedure 48 hours post-procedure. On that same evening, the patient re-presented to hospital with different chest pain and fever. Electrocardiogram (ECG) revealed anterior ST elevation. A provisional diagnosis of pericarditis was made in view of elevated inflammatory markers, a recent Mycoplasma infection with fevers, positron emission tomography-computed tomography (PET-CT) findings, as well as pericardial chest pain. A three-month course of colchicine was initiated. Two…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
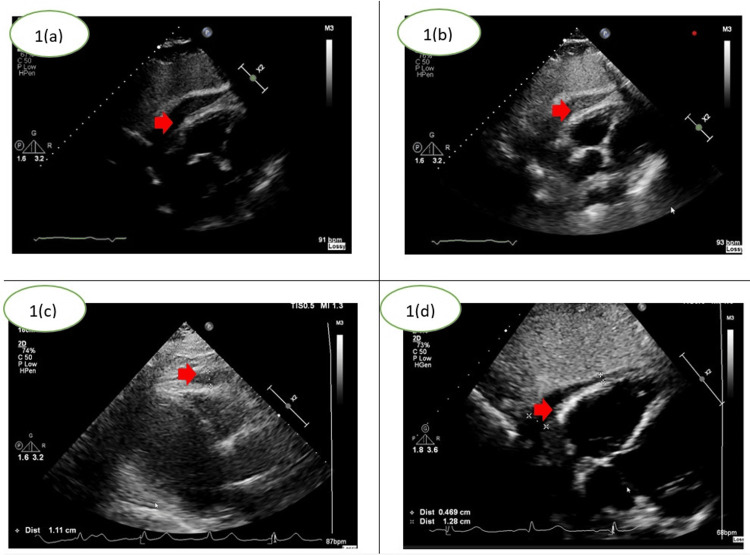 Figure 1
Figure 1| Markers | On admission | Peak | On discharge | Normal ranges |
| Troponin T | 71 | 71 | 28 | <14 ng/L |
| C-reactive protein | 90.5 | 257.5 | 12.5 | <3 mg/L |
| White cell count | 7.42 | 15.88 | 8.7 | 4.5-11 x 10^9/L |
| Blood cultures | No growth after 5 days | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPericarditis and Cardiac Tamponade · Cardiac Structural Anomalies and Repair · Takotsubo Cardiomyopathy and Associated Phenomena
Introduction
Pericarditis is inflammation of the membrane surrounding the heart, and usually manifests as sharp, stabbing central chest pain; other symptoms may include shortness of breath, fever, or fatigue [1]. Causes include viral infections (in developed countries), tuberculosis (in developing countries), autoimmune diseases, myocardial infarction, cardiac surgery, or idiopathic [2]. Diagnosis is based on two of the following: chest pain, new widespread ST-elevation or PR depression on electrocardiogram (ECG), pericardial friction rub and pericardial effusion [3].
Pericarditis may occur after percutaneous coronary intervention (PCI). Proposed mechanisms of post-PCI pericarditis include damage to the pericardial cells, which may lead to activation of immune responses and inflammation [1].
Mainstays of treatment include non-steroidal anti-inflammatory drugs (NSAIDs) or colchicine [3]. In the United Kingdom, there is an annual incidence of approximately 27.7 individuals per 100,000, and recurrence can occur in up to 30% of cases after the first episode [4].
Case presentation
A male in his 60s, otherwise well, presented to hospital with central, non-radiating chest pain and nausea. Examination was unremarkable. ECG showed ST-elevation in V1-V4 and troponin measured at 71. He underwent urgent coronary angiography demonstrating thrombotic left anterior descending (LAD) occlusion with no by-stander disease and received a drug-eluting stent. Transthoracic echocardiography (TTE) showed left ventricular ejection fraction (LVEF) ~45% with apical regional wall-motion abnormality. He was discharged on aspirin, prasugrel, atorvastatin, bisoprolol, ramipril and lansoprazole with standard post-PCI advice. The evening of discharge, he re-presented with pleuritic chest and shoulder pain and low-grade fever, qualitatively different from his initial ischaemic pain. ECG changes were consistent with resolving anterior ST elevation myocardial infarction (STEMI) without new ischaemia and auscultation revealed a pericardial rub. Computed tomography pulmonary angiography (CTPA) excluded pulmonary embolism. TTE and computed tomography (CT) thorax showed a ~20 mm pericardial effusion without tamponade. Given a recent Mycoplasma infection and pericarditic pain, Dressler's syndrome was suspected; colchicine for three months was commenced alongside a 19-day doxycycline course. Twelve days later he re-attended with bilateral shoulder pain and fever. Inflammatory markers were significantly elevated; repeat focused TTE again showed a small-moderate effusion and LVEF 40-45% with apical hypokinesis. Broad septic screening was initiated and empiric intravenous (IV) piperacillin-tazobactam and teicoplanin were started after microbiology discussion in order to empirically manage possible infective pericarditis. CT and positron emission tomography (PET) revealed hypermetabolic pericardial effusion with surrounding fat stranding, supporting active pericarditis. Given absence of tamponade and an unfavourable subxiphoid window, pericardiocentesis was deferred. Cultures remained negative and inflammatory markers down-trended. Three weeks after completing oral co-trimoxazole, he re-presented with recurrent fevers and pericarditic chest pain. IV antibiotics were re-instituted while repeating cultures; anti-inflammatory therapy was optimised. Given recurrent symptoms despite NSAID/colchicine and repeatedly negative cultures, a cautious prednisolone wean was initiated with subsequent improvement.
A six-week follow-up appointment was arranged with the Cardiologist, along with a TTE prior to his appointment to visualise the progress of the effusion. He was advised not to partake in strenuous activities for two weeks, such as lifting, and given advice to return to hospital should he have further episodes of chest pain or shortness of breath.
The following TTE images demonstrate the progression of the pericardial effusion during his hospital stay (Figure 1A-1D). Laboratory results including troponin, C-reactive protein, and white cell count are summarised in Table 1. It was noted that the patient's symptoms improved as the effusion size reduced as shown in Figure 1C, 1D.
Subcostal transthoracic echocardiography (TTE) views of the pericardial effusion. 1(a)- Initial TTE showing small pericardial effusion after percutaneous coronary intervention. 1(b)- Increase in effusion size on day 12 with associated pericarditic pain. 1(c) and (d)- Reduction in effusion after anti-inflammatory and corticosteroid therapy. Red arrows demonstrate the location of the pericardial effusion. TTE images above were obtained from patient records.
The first differential diagnosis considered was another myocardial infarction. However, the declining troponin levels, absent dynamic changes in ECGs, alongside the different character of chest pain ruled this out. CTPA was negative for pulmonary embolism, and TTE ruled out cardiac tamponade. There were no clinical signs of any musculoskeletal injuries.
Discussion
Post-cardiac injury syndrome (PCIS) is a major cause of pericarditis. Damage to the pericardial cells can be caused by surgery, blunt trauma, myocardial necrosis, or iatrogenic [1]. Although the damage caused by PCI may be regarded as minimal, this can lead to activation of immune responses and inflammation. Early infarct-associated pericarditis occurs after five days post-myocardial infarction, whereas late post-myocardial infarction pericarditis (Dressler’s syndrome) occurs two to eight weeks after infarction [1]. In developed countries, the incidence of PCIS is less than 5%, deeming it to be rare [5].
A similarly published case in 2021 involved a gentleman in his 50s, who was admitted for an elective PCI of a chronic total occlusion to the LAD artery. Six hours post-procedure, the patient developed sub-sternal chest pain, worsened by lying down. Repeat angiogram did not show any new findings, and ECG revealed ST-elevation in the anterior and lateral leads. TTE revealed a small pericardial effusion, and a 15-day course of ibuprofen was commenced. A three-fold reduction in C-reactive protein (CRP) was observed after three days of treatment [6].
Another interesting case in 2023 demonstrates a gentleman in his late 70s, who developed constrictive pericarditis after coronary artery perforation during PCI. He was initially admitted due to chest pain and underwent coronary angiogram, which revealed diffuse triple-vessel disease, with right coronary artery (RCA) chronic total occlusion (CTO). PCI at the RCA CTO lesion was complicated by perforation during right ventricular (RV) branch wiring proximal to the lesion. After prolonged balloon inflation, it seemed that the perforation had resolved. A follow-up TTE at one week showed no visible pericardial effusion, and the patient was discharged. Seven months later, the patient re-presented to hospital with dyspnoea and abdominal distention. Coronary angiogram revealed no new lesions, and TTE revealed a small pericardial effusion. He was therefore discharged on prednisolone and colchicine. Two weeks later, the patient went back to hospital with worsening abdominal distention and dyspnoea. TTE showed worsening pericardial effusion and constrictive physiology. The patient became haemodynamically unstable with increasing oxygen requirement, and had to undergo radical pericardiectomy. A thickened pericardium (5mm) was found intraoperatively, and a dark bloody pericardial effusion was drained. He had no complications post-operatively, and was discharged on diuretics with symptoms much improved [7].
Prompt recognition alongside appropriate imaging enables patients to receive treatment in a timely manner. This can prevent complications, such as cardiac tamponade and constrictive pericarditis, which in turn improves patient outcomes.
Conclusions
Mycoplasma infection, although rare, can be a cause of pericarditis. It was difficult to differentiate whether the pericarditis was caused by the Mycoplasma infection or post PCI in this case study, as both factors were involved. It may be worth considering delaying discharge after a PCI if the patient is still having signs of infection to rule out pericarditis. However, this decision should be individualised, based on infection severity, comorbidities, and risk of complications. It is vital to be vigilant and consider PCI complications for patients who present with atypical chest pain.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 12015 ESC Guidelines for the diagnosis and management of pericardial diseases: the Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC) Endorsed by: the European Association for Cardio-Thoracic Surgery (EACTS)Eur Heart J Adler Y Charron P Imazio M 292129643620152632011210.1093/eurheartj/ehv 318PMC 7539677 · doi ↗ · pubmed ↗
- 2Aetiology, treatment and outcomes of pericarditis: long-term data from a longitudinal retrospective single-centre cohort J Clin Med Giordani AS Bocaj I Vicenzetto C 13202410.3390/jcm 13226900 PMC 1159519839598049 · doi ↗ · pubmed ↗
- 3Pericardial effusion The ESC Textbook of Cardiovascular Medicine (3 edn) Brucato A Stefano Maggiolini 15731575 Oxford ESC Publications 2018 https://academic.oup.com/esc/book/35489/chapter-abstract/312419743
- 4Acute pericarditis: update Curr Cardiol Rep Lazarou E Tsioufis P Vlachopoulos C Tsioufis C Lazaros G 9059132420223559594910.1007/s 11886-022-01710-8PMC 9122084 · doi ↗ · pubmed ↗
- 5Post-cardiac Injury syndrome: aetiology, diagnosis, and treatment Cardiol Pract Sasse T Eriksson U 152017 https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volume-15/Post-cardiac-injury-syndrome-aetiology-diagnosis-and-treatment
- 6Acute pericarditis after percutaneous coronary intervention: a case report Medicina (Kaunas) RodevičG Budrys P Davidavičius G 57202110.3390/medicina 57050490 PMC 815203334067941 · doi ↗ · pubmed ↗
- 7Case report: constrictive pericarditis after coronary artery perforation during percutaneous coronary intervention Front Cardiovasc Med Kim KA Lee KY Hwang BH Kim DY Park CB 1208376102023 https://www.frontiersin.org/journals/cardiovascular-medicine/articles/10.3389/fcvm.2023.1208376/full 3734628610.3389/fcvm.2023.1208376 PMC 10280286 · doi ↗ · pubmed ↗