Sarcoidosis Masquerading as Adjustment Disorder: A Case Report of Hypercalcemia-Induced Altered Sensorium
Keerthana Sri, Sowmya Gopalan

TL;DR
A case of sarcoidosis was misdiagnosed as an adjustment disorder but was later correctly identified due to severe hypercalcemia and neurological symptoms.
Contribution
This case report highlights sarcoidosis as a rare but important cause of hypercalcemia-induced neurological symptoms.
Findings
The patient showed marked hypercalcemia and neurological symptoms due to sarcoidosis.
Early treatment with corticosteroids and electrolyte correction led to rapid clinical improvement.
Sarcoidosis should be considered in patients with unexplained hypercalcemia and altered mental status.
Abstract
Sarcoidosis is a multisystem granulomatous disease that can present with nonspecific symptoms and, rarely, with severe hypercalcemia and neurological manifestations. We report a case of a 55-year-old female with systemic hypertension, type 2 diabetes mellitus, and hypothyroidism, who presented with reduced appetite for five months, altered sensorium for three months, and difficulty rising from bed. Initial evaluation elsewhere diagnosed adjustment disorder. On further workup, she was found to have marked hypercalcemia (serum calcium = 16.7 mg/dL), renal dysfunction (creatinine = 3.7 mg/dL), and a chest X-ray showed hilar lymphadenopathy. Positron emission tomography-computed tomography revealed periportal and mediastinal lymphadenopathy. Endobronchial ultrasound-guided biopsy showed necrotizing granulomatous inflammation. Acid-fast bacillus testing was negative, and serum…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
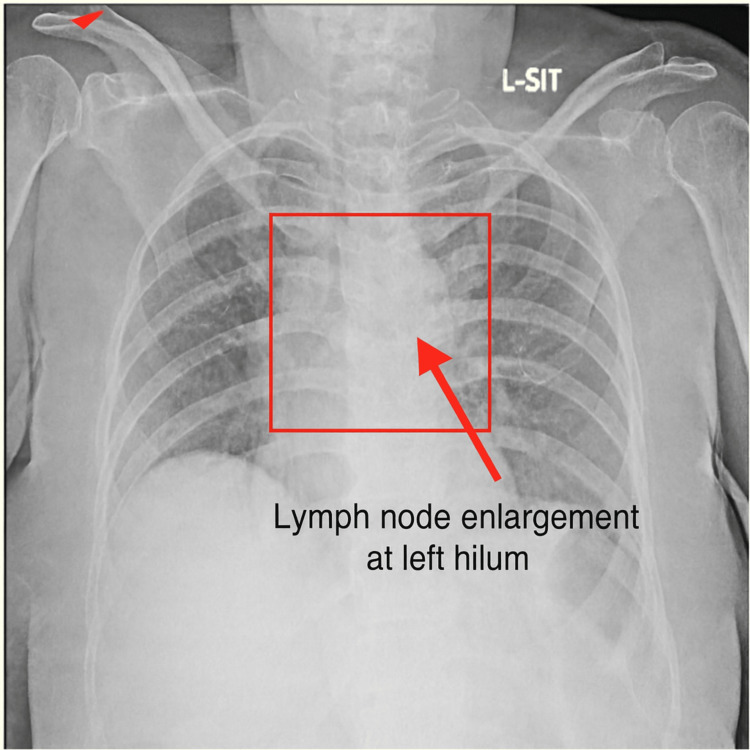 Figure 1
Figure 1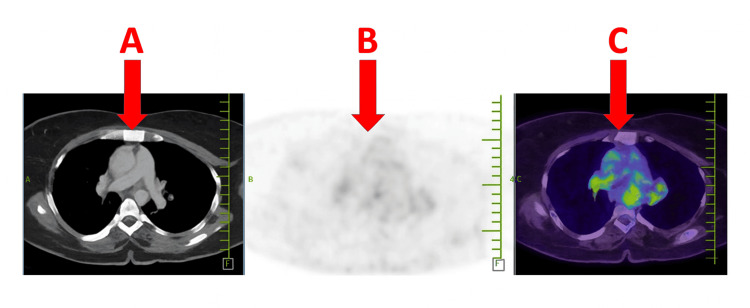 Figure 2
Figure 2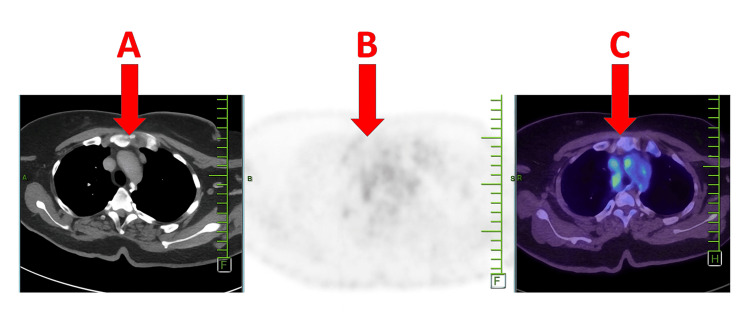 Figure 3
Figure 3| Test | Result | Reference range | Interpretation |
| Serum calcium | 16.7 mg/dL | 8.5 – 10.5 mg/dL | Severe hypercalcemia |
| Serum creatinine | 3.7 mg/dL | 0.6 – 1.2 mg/dL | Acute kidney injury |
| Chest X-ray | Bilateral hilar lymphadenopathy | Normal: Clear lung fields, no lymphadenopathy | Suggestive of granulomatous disease |
| Ultrasonography (USG) neck | Normal | Normal thyroid and parathyroid morphology | No parathyroid abnormality |
| Vitamin D (total) | Normal | 30 – 100 ng/mL | Excludes exogenous cause |
| X-ray lumbosacral (LS) spine & pelvis | Normal | No abnormal bony lesions | No bony lesions |
| PET-CT | Periportal and mediastinal lymphadenopathy | Normal: No FDG-avid lymphadenopathy | Systemic involvement |
| EBUS biopsy | Necrotizing granulomatous inflammation | Normal: No granulomas | Consistent with sarcoidosis |
| Acid-fast bacillus (AFB) GeneXpert | Negative | Negative | Excludes tuberculosis |
| Angiotensin-converting enzyme (ACE) levels | 92 U/L | 8 – 52 U/L (lab-dependent) | Supports sarcoidosis diagnosis |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoidosis and Beryllium Toxicity Research · Osteomyelitis and Bone Disorders Research · Trace Elements in Health
Introduction
Sarcoidosis is a systemic granulomatous inflammatory disorder of unknown etiology that most commonly affects the lungs and intrathoracic lymph nodes, but may involve virtually any organ. The clinical presentation is heterogeneous and ranges from asymptomatic radiographic findings to multisystem disease with constitutional symptoms, organ dysfunction, and metabolic complications [1-4]. Hypercalcemia in sarcoidosis most commonly results from extrarenal production of 1,25-dihydroxyvitamin D (calcitriol) by activated macrophages within granulomatous tissue. Unlike renal synthesis, this extrarenal pathway is not tightly regulated by parathyroid hormone or serum calcium levels, leading to sustained overproduction of calcitriol. The consequent increase in intestinal calcium absorption predisposes patients to hypercalcemia and hypercalciuria, both of which can contribute to renal complications such as nephrolithiasis, nephrocalcinosis, and progressive renal dysfunction. In addition, elevated calcium levels may produce systemic manifestations, including fatigue, muscle weakness, and neuropsychiatric symptoms, thereby compounding the overall disease burden [4-6].
Neurological involvement in sarcoidosis, known as neurosarcoidosis, can occur through two principal mechanisms. First, direct granulomatous infiltration of the central or peripheral nervous system can involve the meninges, cranial nerves, spinal cord, or cerebral parenchyma, resulting in a wide clinical spectrum that ranges from chronic meningitis and cranial neuropathies to seizures and myelopathy. Second, neurological symptoms may arise indirectly from metabolic or toxic consequences, most notably those associated with severe hypercalcemia. Hypercalcemia-induced encephalopathy can manifest as cognitive impairment, mood disturbances, lethargy, psychosis, or, in extreme cases, coma. Thus, neurosarcoidosis reflects a complex interplay between localized granulomatous inflammation and systemic metabolic dysregulation, both of which may coexist and amplify neurological morbidity [6-9].
This case report emphasizes the importance of a high index of suspicion for sarcoidosis in patients with systemic symptoms and severe electrolyte disturbances.
Case presentation
A 55-year-old female, residing in Andaman, presented with reduced appetite for five months and altered sensorium for three months. She also experienced progressive difficulty getting out of bed. Her medical history included systemic hypertension, type 2 diabetes mellitus, and hypothyroidism, all medically controlled. She was initially evaluated in a local hospital in May 2024, where she was diagnosed with adjustment disorder and treated with supportive measures. Her condition deteriorated over time, prompting further evaluation.
On clinical examination, the patient was drowsy, dehydrated, and responding to simple oral commands, with stable vitals. On systemic examination, no respiratory distress or other signs of infection were noted.
Neurological examination revealed the following findings: consciousness and orientation testing showed the patient was alert and oriented to time, place, and person. Higher mental functions testing showed a Mini-Mental State Examination (MMSE) score of 28/30, with intact attention, memory, comprehension, and abstract thinking, and depressed mood with psychomotor retardation.
Cranial nerves (II-XII) were intact, pupils were equal and reactive, extraocular movements were full, and no facial asymmetry or dysarthria was noted. Motor system testing revealed normal tone, power of 5/5 in all limbs, and no involuntary movements, with mild proximal fatigability noted on sustained activity. Reflexes testing showed deep tendon reflexes were present and symmetrical, with plantar reflex flexor bilaterally, and no clonus. Sensory system testing revealed pain, temperature, vibration, and proprioception intact, with no dermatomal sensory loss. Coordination testing revealed normal finger-nose and heel-knee tests, with no dysmetria or past pointing. The gait was normal. Autonomic function testing revealed no orthostatic hypotension.
Baseline investigations are presented in Table 1. Chest radiography revealed bilateral hilar lymphadenopathy (Figure 1). PET-CT demonstrated periportal and mediastinal lymphadenopathy (Figures 2, 3). Endobronchial ultrasound (EBUS) biopsy showed necrotizing granulomatous inflammation.
Chest X-ray (posteroanterior view) showing lymph node enlargement at the left hilum (red arrow).
Axial PET-CT images of the thorax.(A) CT showing periportal lymph nodes. (B) PET grayscale image. (C) Fused PET-CT highlighting fluorodeoxyglucose-avid periportal lymphadenopathy (red arrows), consistent with sarcoidosis-related lymphadenopathy.
Axial PET-CT images of the thorax.(A) CT showing mediastinal lymph nodes. (B) PET grayscale image. (C) Fused PET-CT highlighting fluorodeoxyglucose-avid mediastinal and hilar lymph nodes (red arrows), consistent with sarcoidosis-related lymphadenopathy.
Differential diagnoses considered were tuberculosis, which was excluded based on negative acid-fast bacillus (AFB) testing and absence of constitutional symptoms, malignancy, which was not supported by imaging or pathology, and primary hyperparathyroidism, which was excluded by normal neck ultrasound and vitamin D.
The patient was managed with aggressive hydration consisting of an initial bolus of 0.9% saline at 15 mL/kg IV over two hours, followed by maintenance fluids at 2.5 mL/kg/hour.
Correction of hypercalcemia was done, and intravenous fluids were administered to restore renal perfusion. The patient was started on oral prednisone 40 mg once daily to reduce granulomatous inflammation. Regular monitoring of electrolytes, renal function, and neurological status was done.
Outcome and follow-up
The patient showed marked clinical improvement after initiation of aggressive intravenous hydration and corticosteroid therapy. Calcium decreased to 11.0 mg/dL and creatinine to 1.5 mg/dL. By day three, serum calcium normalized to 9.6 mg/dL and creatinine improved to 1.2 mg/dL, correlating with marked symptomatic improvement.
At two-week outpatient follow-up (day 14), the patient reported sustained improvement in mood, energy levels, and bowel habits. Repeat laboratory investigations showed a serum calcium of 9.4 mg/dL, creatinine of 1.0 mg/dL, and a fall in angiotensin-converting enzyme (ACE) level to 70 U/L. There were no new systemic or neurological symptoms. Prednisone was continued at the same dose for another week, followed by a gradual taper of 5 mg every two weeks under close monitoring.
At one-month follow-up, the patient remained asymptomatic, with normal appetite and no recurrence of constipation or fatigue. Serum calcium and renal parameters remained within the normal range. She had no features of corticosteroid toxicity, and chest imaging showed persistent but non-progressive mediastinal lymphadenopathy.
Discussion
Sarcoidosis is a multisystem granulomatous disease with variable clinical presentation and outcomes. Pulmonary and lymphatic involvement are most common, but extrapulmonary manifestations can be the initial clue to diagnosis [1,2]. Hypercalcemia occurs in approximately 10-20% of sarcoidosis patients and is mediated by extrarenal conversion of 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D by activated macrophages in granulomatous tissue [3,4]. This results in increased intestinal calcium absorption and reduced renal excretion, which can precipitate acute kidney injury if left untreated [5]. Several case reports and series have described neurocognitive or psychiatric symptoms associated with hypercalcemia secondary to sarcoidosis. In one study, Sharma reported that hypercalcemia may present with depression, confusion, or encephalopathy, often preceding systemic diagnosis [4]. Our patient similarly presented with altered sensorium, initially attributed to a psychiatric disorder, which delayed recognition of the underlying metabolic disturbance. The diagnosis of sarcoidosis requires a combination of compatible clinical and radiological findings, histological confirmation of non-caseating granulomas, and exclusion of alternative causes such as tuberculosis and fungal infections [6]. In endemic areas, distinguishing sarcoidosis from tuberculosis remains particularly challenging; however, negative microbiological studies (including AFB GeneXpert) and necrotizing granulomatous histopathology supported sarcoidosis in our case. The role of serum ACE levels remains controversial. While elevated ACE supports the diagnosis, it lacks sensitivity and specificity [7]. Nevertheless, in conjunction with histology and imaging, it contributed to the diagnostic certainty in this case. PET-CT has emerged as a valuable tool for detecting occult systemic involvement, assessing disease activity, and guiding biopsy sites [8], as demonstrated in our patient. Management of sarcoidosis-related hypercalcemia requires prompt recognition and correction of electrolyte imbalance, aggressive hydration, and corticosteroid therapy [9]. Corticosteroids reduce granulomatous activity and suppress extrarenal vitamin D activation, leading to normalization of calcium levels. Our patient responded well to steroids, with resolution of hypercalcemia and improvement in sensorium.
This case reinforces the need for clinicians to consider sarcoidosis in the differential diagnosis of unexplained hypercalcemia with neurological manifestations. Early diagnosis is crucial to prevent complications such as irreversible renal dysfunction and chronic neurocognitive impairment.
Conclusions
This case demonstrates that sarcoidosis can rarely present with severe hypercalcemia, causing neuropsychiatric symptoms and acute kidney injury. Hypercalcemia in sarcoidosis results from unregulated calcitriol production by activated macrophages within granulomas and, if unrecognized, can lead to complications such as renal dysfunction and neuropsychiatric manifestations. Careful evaluation with laboratory studies, imaging, and histopathological confirmation is essential to distinguish sarcoidosis from other granulomatous diseases, particularly tuberculosis in endemic areas. In patients with unexplained hypercalcemia and lymphadenopathy, sarcoidosis should be considered after excluding more common causes such as malignancy and tuberculosis. Early recognition and prompt corticosteroid therapy can lead to rapid clinical and biochemical recovery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sarcoidosis Lancet Baughman RP Lower EE du Bois RM 1111111836120031267232610.1016/S 0140-6736(03)12888-7 · doi ↗ · pubmed ↗
- 2Statement on sarcoidosis. Joint Statement of the American Thoracic Society (ATS), the European Respiratory Society (ERS) and the World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG) adopted by the ATS Board of Directors and by the ERS Executive Committee, February 1999 Am J Respir Crit Care Med 73675516019991043075510.1164/ajrccm.160.2.ats 4-99 · doi ↗ · pubmed ↗
- 3Sarcoidosis N Engl J Med Iannuzzi MC Rybicki BA Teirstein AS 2153216535720071803276510.1056/NEJ Mra 071714 · doi ↗ · pubmed ↗
- 4Hypercalcemia in granulomatous disorders: a clinical review Curr Opin Pulm Med Sharma OP 442447620001095823710.1097/00063198-200009000-00010 · doi ↗ · pubmed ↗
- 5Calcium and vitamin D in sarcoidosis: how to assess and manage Semin Respir Crit Care Med Burke RR Rybicki BA Rao DS 4744843120102066539710.1055/s-0030-1262215 PMC 4876288 · doi ↗ · pubmed ↗
- 6Neurosarcoidosis: a clinical dilemma Lancet Neurol Hoitsma E Faber CG Drent M Sharma OP 397407320041520779610.1016/S 1474-4422(04)00805-1 · doi ↗ · pubmed ↗
- 7Neurosarcoidosis: pathophysiology, diagnosis, and treatment Neurol Neuroimmunol Neuroinflamm Bradshaw MJ Pawate S Koth LL Cho TA Gelfand JM 08202110.1212/NXI.0000000000001084 PMC 849550334607912 · doi ↗ · pubmed ↗
- 8Sarcoidosis Lancet Valeyre D Prasse A Nunes H Uzunhan Y Brillet PY Müller-Quernheim J 1155116738320142409079910.1016/S 0140-6736(13)60680-7 · doi ↗ · pubmed ↗