Flush Occlusion of the Superficial Femoral Artery Managed Using a Retrograde Popliteal Approach: A Case Report
Nadeen Aladham, Herbert Oye

TL;DR
A rare case of a blocked artery in the leg was successfully treated using a less common backward surgical approach.
Contribution
Demonstrates the effectiveness of a retrograde popliteal approach for flush superficial femoral artery occlusions.
Findings
The retrograde popliteal approach provided direct access to the distal true lumen in a flush occlusion case.
This approach proved successful in treating arterial thrombosis when traditional methods failed.
It offers a viable option for managing complex peripheral arterial disease.
Abstract
Flush occlusion of the superficial femoral artery (SFA) poses significant challenges for endovascular revascularization because the absence of a distal stump complicates antegrade access. Traditional treatment options include balloon-directed catheter thrombectomy, mechanical thrombectomy, and tissue plasminogen activator thrombolysis. However, these approaches may be less effective in cases of flush or long-segment occlusions. The retrograde popliteal approach has emerged as a viable alternative, providing direct access to the distal true lumen and proving particularly useful when antegrade strategies fail. This case report describes the successful use of the retrograde popliteal approach to treat a flush SFA occlusion caused by arterial thrombosis, highlighting its role in managing complex peripheral arterial disease.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
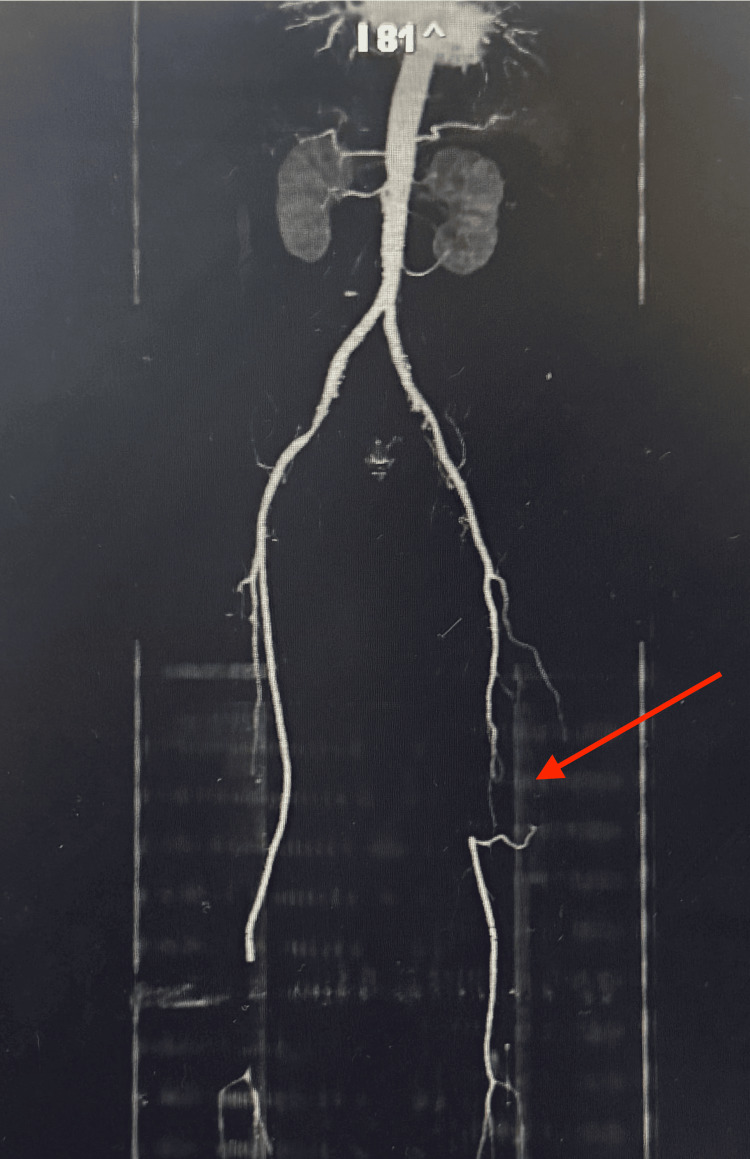 Figure 1
Figure 1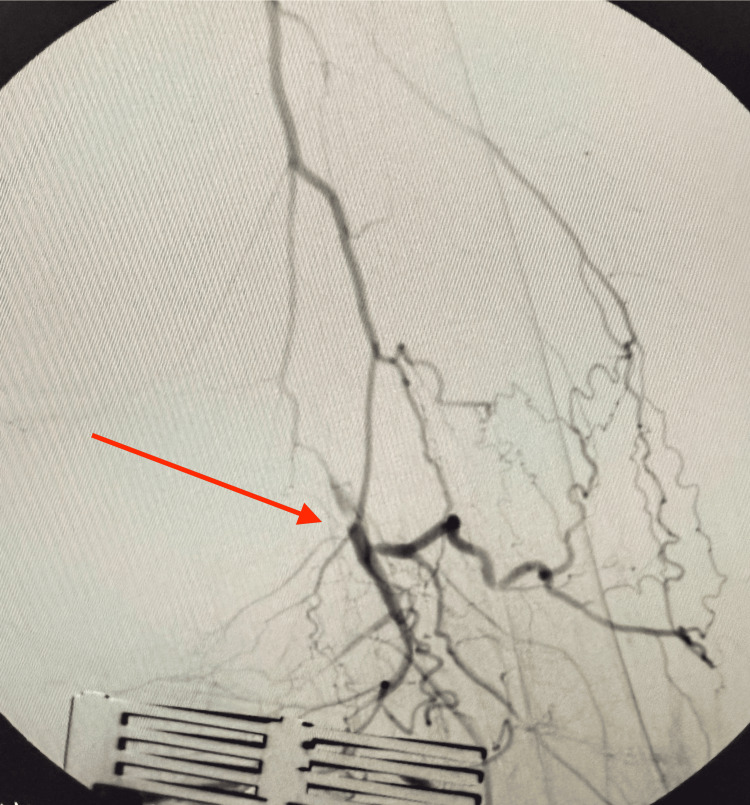 Figure 2
Figure 2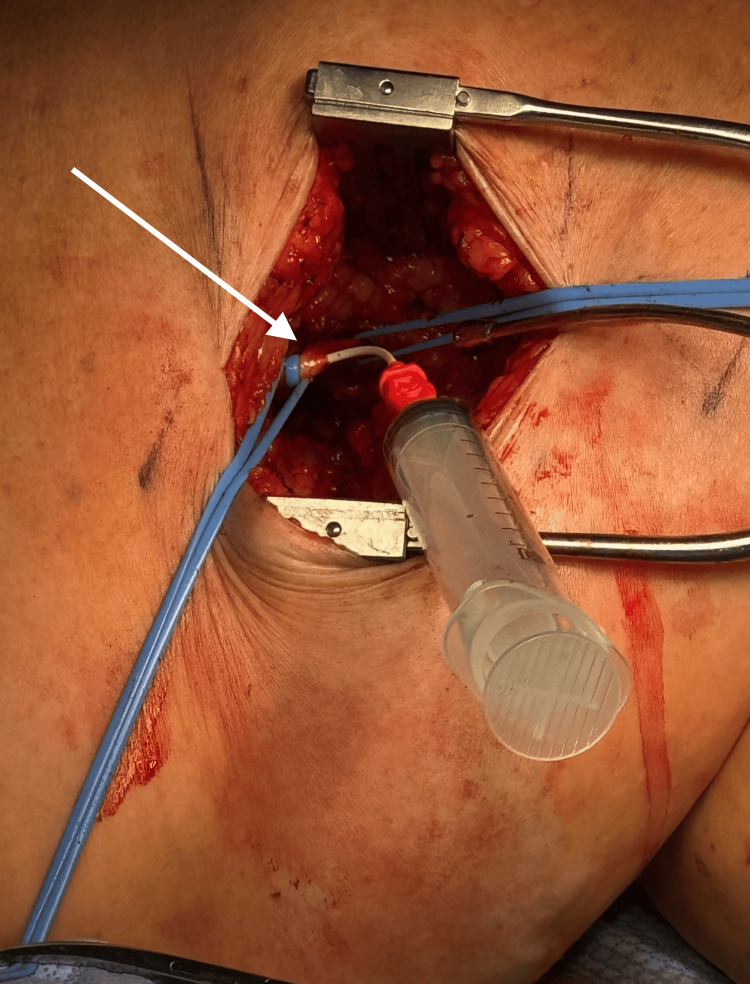 Figure 3
Figure 3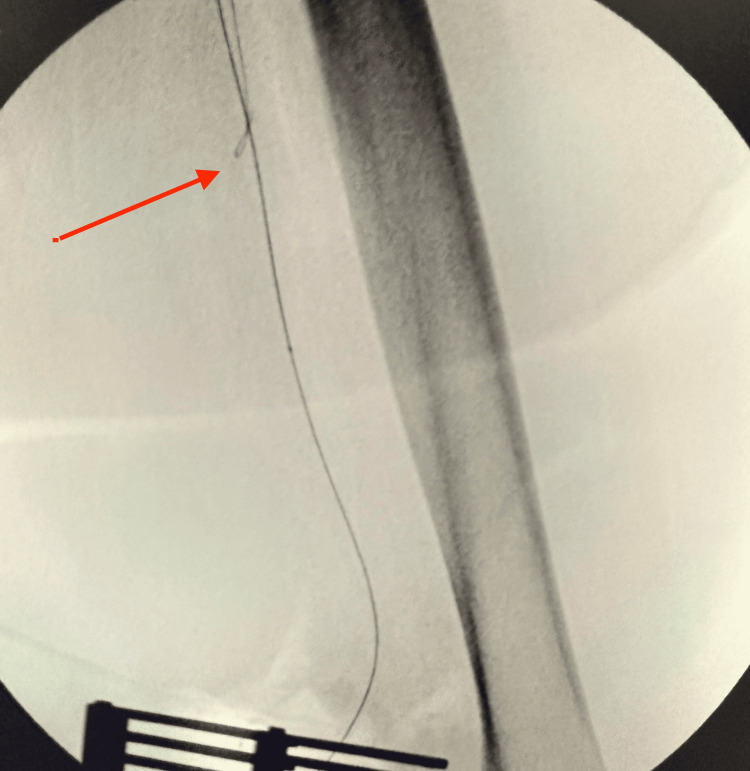 Figure 4
Figure 4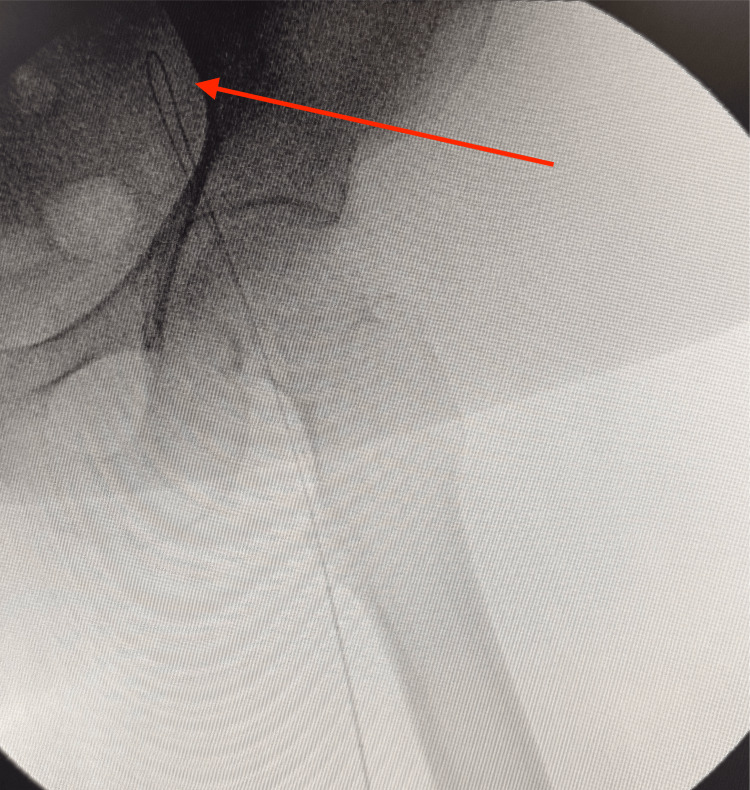 Figure 5
Figure 5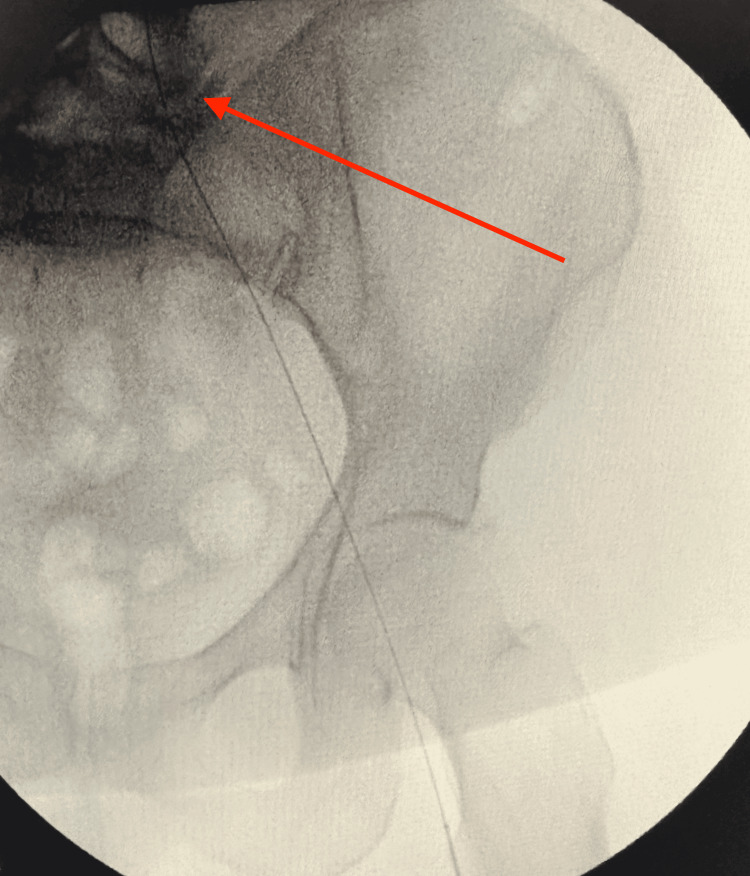 Figure 6
Figure 6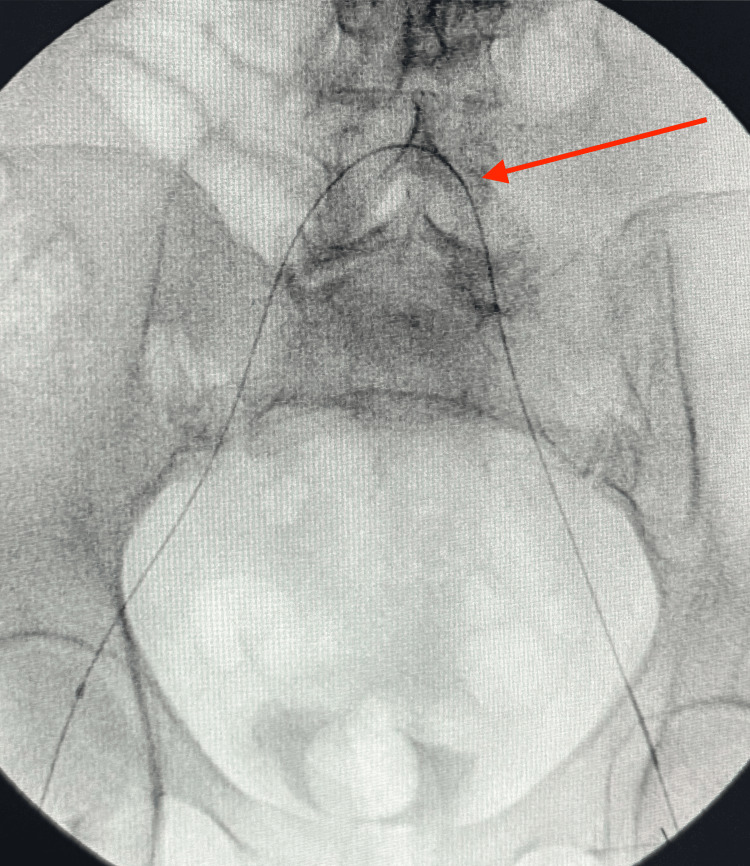 Figure 7
Figure 7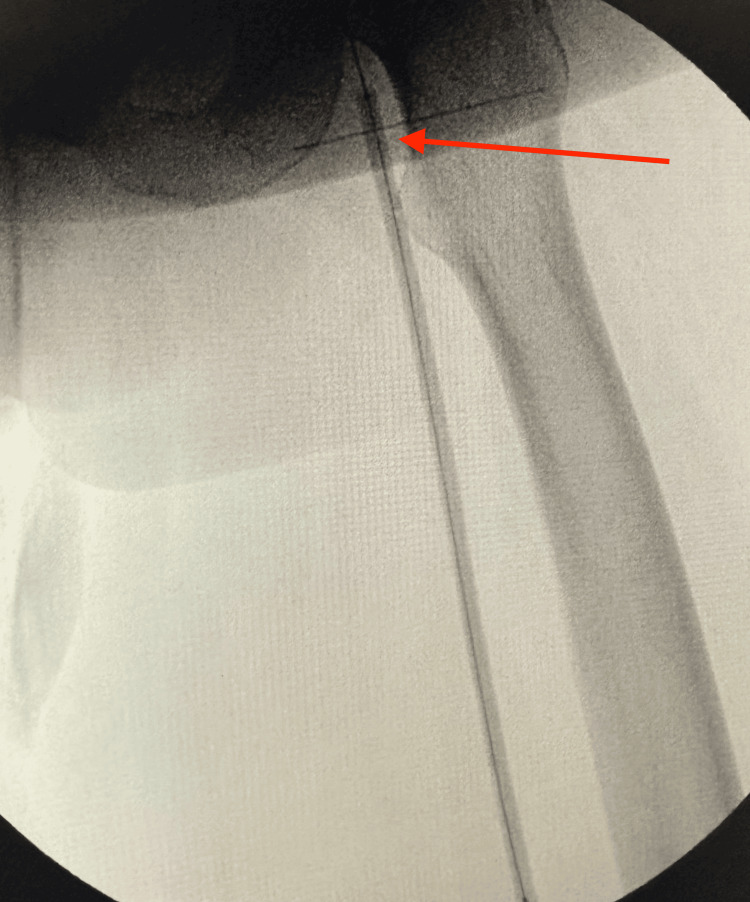 Figure 8
Figure 8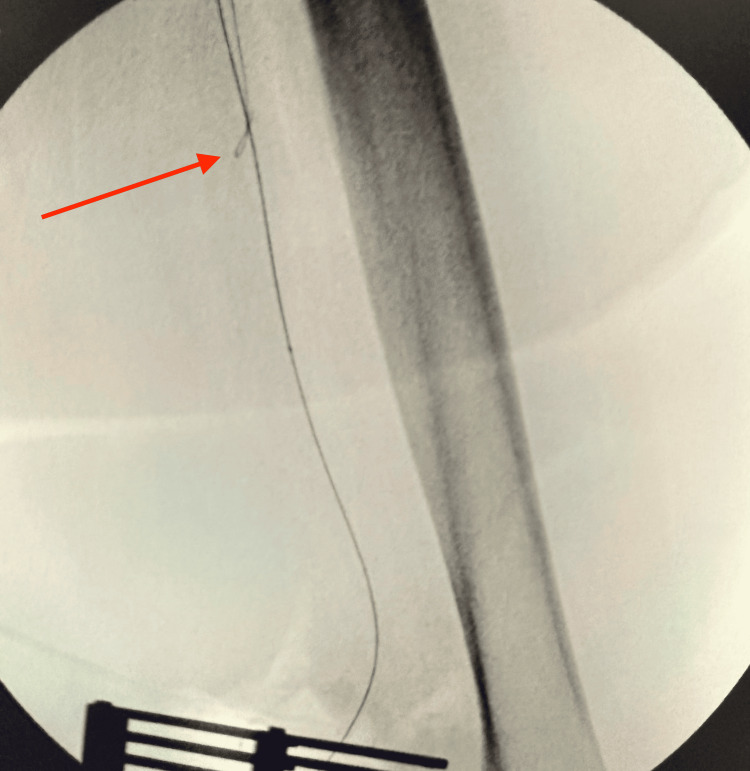 Figure 9
Figure 9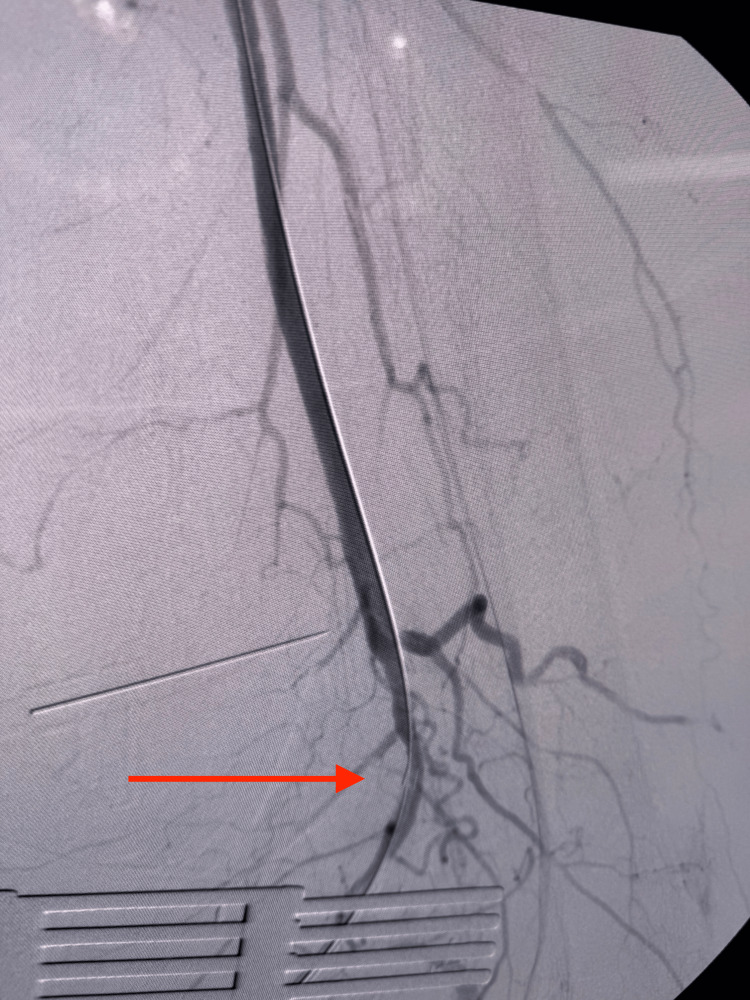 Figure 10
Figure 10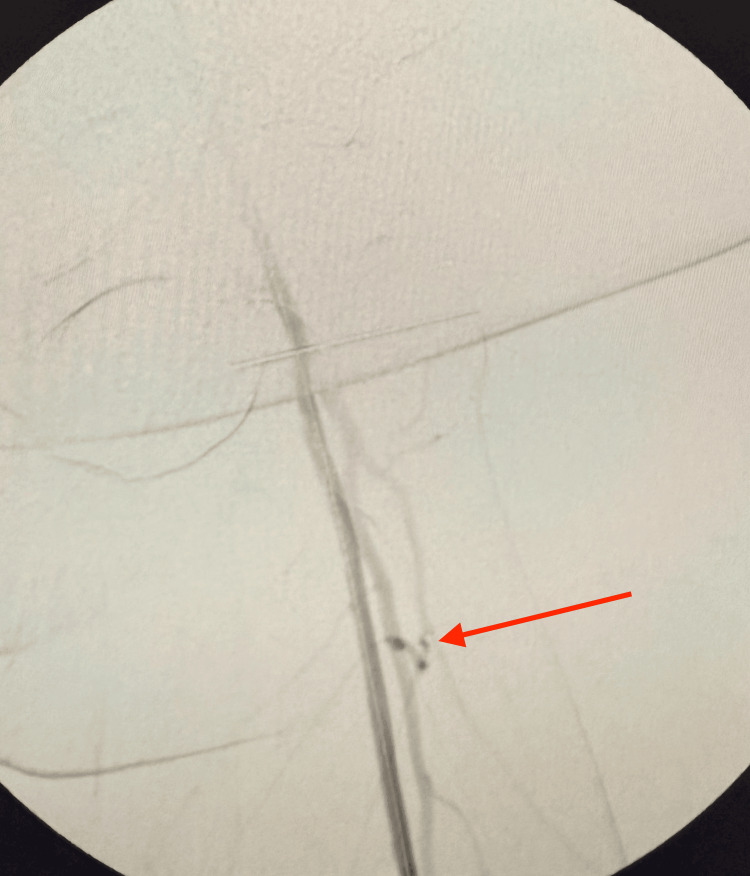 Figure 11
Figure 11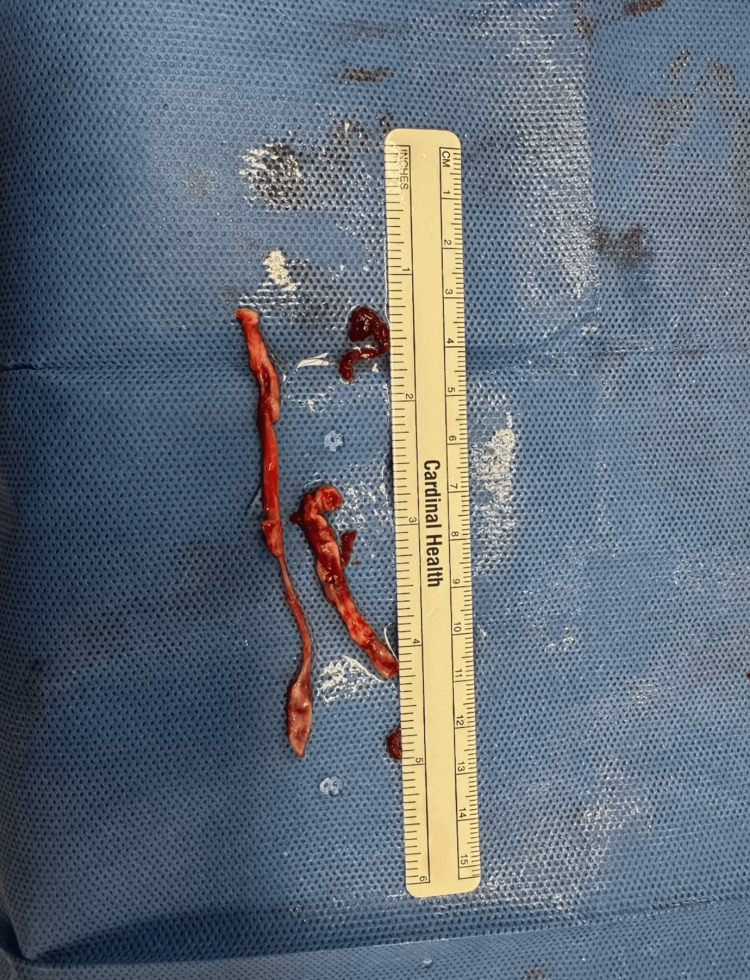 Figure 12
Figure 12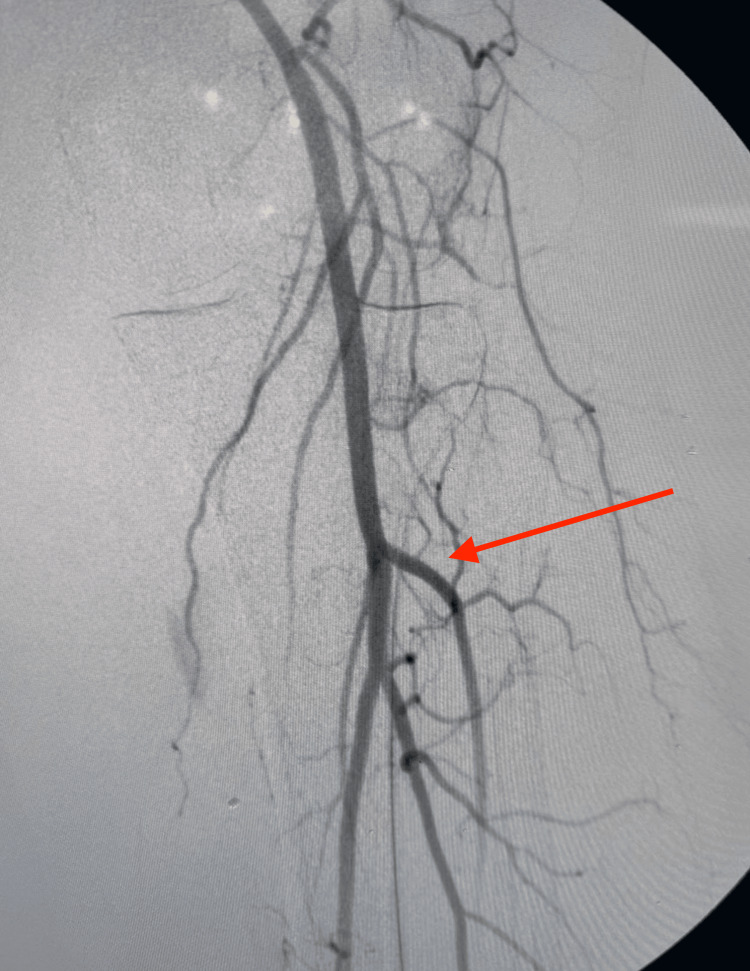 Figure 13
Figure 13 Figure 14
Figure 14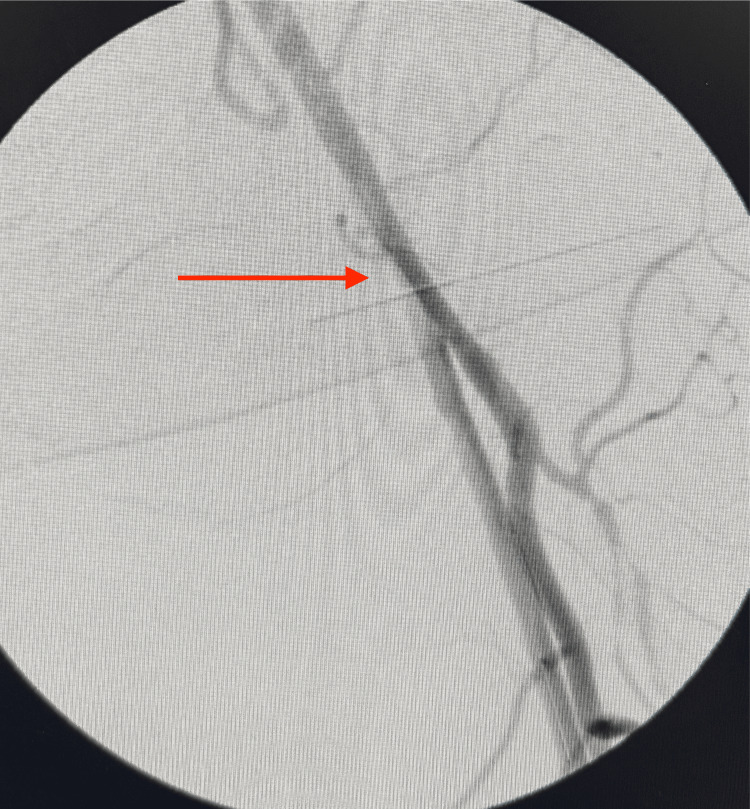 Figure 15
Figure 15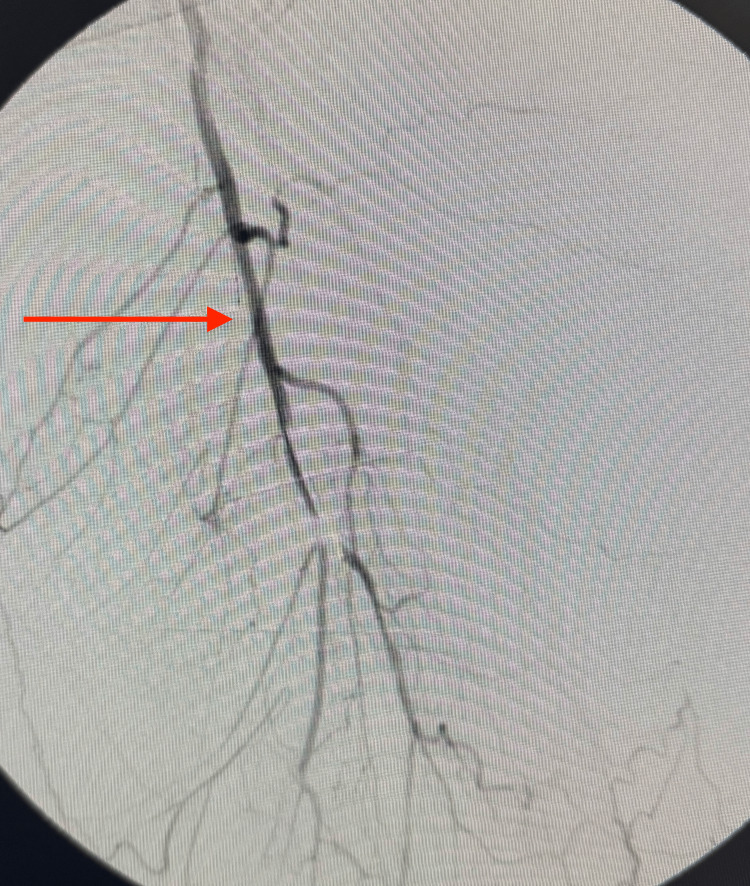 Figure 16
Figure 16| Test | Patient value | Reference range | Unit |
| White blood cell count | 7.9 | 4.0-11.0 | × 10⁹/L |
| Hemoglobin | 13.8 | 11.6-15.0 | g/dL |
| Hematocrit | 42.5 | 35-45 | % |
| Platelet count | 237 | 150-450 | × 10⁹/L |
| Sodium | 140 | 135-145 | mmol/L |
| Potassium | 3.8 | 3.5-5.0 | mmol/L |
| Chloride | 108 | 98-107 | mmol/L |
| Bicarbonate | 23 | 22-29 | mmol/L |
| Blood urea nitrogen | 15 | 7-20 | mg/dL |
| Creatinine | 0.8 | 0.59-1.04 | mg/dL |
| Glucose | 97 | 70-100 | mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Artery Disease Management · Vascular Procedures and Complications · Aortic aneurysm repair treatments
Introduction
Lower extremity ischemia caused by superficial femoral artery (SFA) occlusion can result in significant morbidity if not promptly managed. Arterial thrombosis, often superimposed on atherosclerotic plaque, is a common underlying mechanism. Thrombus at the origin of the profunda femoris artery frequently arises from a combination of proximal plaque rupture or ulceration, distal embolization, and local flow stagnation. In flush SFA occlusion, altered hemodynamics at the femoral bifurcation can predispose to thrombus formation within the profunda origin.
Treatment options include Fogarty catheter thrombectomy, mechanical thrombectomy, tissue plasminogen activator thrombolysis, and conventional antegrade endovascular revascularization [1-3]. However, certain lesions, particularly flush or long-segment occlusions, pose technical challenges that may limit the success of antegrade approaches.
The retrograde popliteal approach provides direct access to the distal true lumen and has emerged as a reliable alternative in these difficult cases. Thrombus and atheromatous debris were removed using manual aspiration through selective catheters and mechanical extraction with a Fogarty thrombectomy catheter when required. When endovascular aspiration alone was insufficient, an open popliteal arteriotomy allowed direct Fogarty thrombectomy and facilitated retrograde wiring. Balloon angioplasty was then used for vessel preparation, followed by a drug-coated balloon to treat the underlying atherosclerotic disease.
Modern techniques employing ultrasound guidance and low-profile devices have improved both safety and technical success. Studies report high technical success rates and favorable short- to mid-term patency outcomes [4-6]. This approach is particularly valuable when traditional antegrade, thrombectomy, or thrombolysis strategies are unsuccessful, offering a viable solution for complex SFA occlusions. In this patient, a less invasive strategy was favored due to comorbidities and the technical feasibility of retrograde popliteal access.
Case presentation
A 56-year-old female with a history of hypertension, hyperlipidemia, hypothyroidism, and peripheral vascular disease presented with acute left leg pain. She denied chest pain, dizziness, or syncope. On physical examination, distal pulses in the left lower extremity were diminished compared with the contralateral side.
Laboratory findings on presentation are summarized in Table 1, with reference ranges derived from Mayo Clinic Laboratories and institutional norms [7].
Abdominal CT angiography (CTA) with runoff demonstrated complete occlusion of the left SFA (Figure 1). No other significant vascular abnormalities were identified.
CT angiogram with runoff demonstrating complete occlusion of the left SFA (red arrow)SFA, superficial femoral artery
Given the CTA findings, informed consent was obtained, and the patient was prepared for surgery. An angiogram with fluoroscopy confirmed complete occlusion of the left SFA (Figure 2).
Fluoroscopic angiogram of the left SFA showing complete occlusion (red arrow)SFA, superficial femoral artery
An initial attempt to cross the lesion via a right femoral approach with a crossover sheath was unsuccessful. Given the failure of antegrade access, the decision was made to expose the left popliteal artery to allow retrograde cannulation of the popliteal, SFA, and iliac arteries (Figure 3).
Exposure of the left popliteal artery for retrograde access (white arrow)
Through a popliteal arteriotomy, the lesion was successfully crossed retrogradely. A stepwise retrograde popliteal approach was performed for revascularization of the completely occluded left SFA. The site of complete arterial occlusion is shown with the guidewire attempting to cross the blockage (Figure 4). Continued advancement of the wire is illustrated as it traverses the occluded segment (Figure 5), eventually reaching the iliac artery (Figure 6). Subsequent fluoroscopic imaging confirmed a patent left iliac artery (Figure 7).
Site of complete arterial occlusion, with the guidewire attempting to cross the blockage (red arrow)
Continued advancement of the wire, attempting to traverse the occluded segment (red arrow)
Wire successfully advanced to the iliac artery (red arrow)
Recanalization of the iliac artery (red arrow)
The first balloon was positioned at the level where the flush occlusion begins (Figure 8). The guidewire continued to advance toward the occlusion and approached the level of the blockage (Figure 9). The balloon was then advanced from the groin toward the lesion, with contrast outlining its position (Figure 10). Following balloon angioplasty, the flush occlusion was successfully opened; however, a thrombus was noted at the origin of the profunda femoris artery (Figure 11).
First balloon positioned at the level where the flush occlusion begins (red arrow)
Guidewire advancing toward the occlusion, approaching the level of the blockage (red arrow)
Balloon advanced from the groin toward the occlusion site, with contrast outlining its position (red arrow)
Flush occlusion successfully opened, with thrombus noted at the origin of the profunda femoris artery (red arrow)
Sequential balloon angioplasty was performed using a 6 mm × 200 mm plain balloon, followed by a 6 mm × 300 mm drug-coated balloon (Figure 8, Figure 9). Thrombus and atherosclerotic plaque were also extracted (Figure 12).
Extraction of thrombus from the left popliteal artery
Retrograde popliteal angioplasty was completed, and fluoroscopic angiography demonstrated restoration of flow through the left SFA (Figure 13). The guidewire was successfully advanced distally to the level of the ankle (Figure 14). Post-procedure selective catheter angiography confirmed persistent patency of the left SFA and proximal profunda femoris artery (Figure 15).
Fluoroscopic angiogram after retrograde popliteal angioplasty demonstrating restoration of flow through the left SFA (red arrow)SFA, superficial femoral artery
Guidewire successfully advanced distally to the level of the ankle (red arrow)
Selective catheter angiogram after retrograde popliteal angioplasty demonstrating restoration of flow (red arrow) through the left SFA and proximal profunda femoris arterySFA, superficial femoral artery
On follow-up, selective angiography demonstrated persistent patency of the left SFA at the site of retrograde popliteal revascularization (Figure 16). Clinically, the patient had improved distal pulses in the affected extremity and complete resolution of ischemic pain.
Follow-up selective angiogram demonstrating persistent patency of the lower portion of the profunda femoris artery (red arrow) after retrograde popliteal revascularization
All assessment tools, measurements, and procedural descriptions in this case report were developed by the authors.
Discussion
Femoral-popliteal (fem-pop) bypass is an established revascularization strategy for SFA occlusions. While effective, it carries increased risks, including groin infection and lymphatic complications, particularly in patients with comorbidities [8]. In this patient, although fem-pop bypass could have been performed, the elevated risk of lymphatic complications made a less invasive approach preferable.
The retrograde popliteal approach was chosen for its direct access to the distal true lumen, enabling crossing of a chronic total occlusion of the SFA. This technique requires only a single incision, reducing surgical trauma and minimizing the risk of wound or lymphatic complications compared with fem-pop bypass [4,5]. Sequential balloon angioplasty using a Mustang and a Lutonix drug-coated balloon, combined with thrombus and plaque extraction, successfully restored flow, demonstrating the efficacy of this method in complex lesions that are difficult to cross antegradely [4,5].
Additionally, a hybrid endovascular strategy via the right common femoral artery was employed to remove thrombus from the profunda femoris artery. This allowed simultaneous treatment of both proximal and distal lesions while minimizing operative trauma, highlighting the versatility of combining retrograde popliteal access with complementary endovascular interventions [5,6].
In this patient, the combination of retrograde popliteal angioplasty and hybrid endovascular intervention resulted in complete revascularization, improved distal pulses, and resolution of ischemic symptoms. This case demonstrates that retrograde popliteal revascularization is a feasible and effective alternative to fem-pop bypass, particularly in patients with complex occlusions and comorbidities where minimally invasive strategies are preferable [4-6].
Conclusions
Retrograde popliteal revascularization is a feasible and effective option for managing flush SFA occlusions, particularly when antegrade access fails. This approach can reduce the need for fem-pop bypass, thereby minimizing surgical risks such as groin infection and lymphatic complications. Furthermore, it allows for simultaneous or complementary endovascular interventions, such as thrombus removal from the profunda femoris artery, providing a hybrid strategy that maximizes revascularization success while minimizing operative trauma. This case demonstrates that retrograde popliteal access is a safe, less invasive alternative for complex peripheral arterial occlusions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Catheter-directed intra-arterial thrombolysis for lower extremity arterial occlusions Anatol J Cardiol GüneşY Sincer I Erdal E 54592220193137564810.14744/Anatol J Cardiol.2019.63296 PMC 6735447 · doi ↗ · pubmed ↗
- 2Percutaneous-aspiration thrombectomy for acute and subacute lower-limb ischemia: feasibility and mid-term results Egypt J Surg Zied SA Desoky HF Eldmarany HA 13101320402021 https://journals.lww.com/ejos/fulltext/2021/40040/percutaneous_aspiration_thrombectomy_for_acute_and.38.aspx
- 3Retrograde popliteal approach for challenging occlusions of the femoral-popliteal arteries J Vasc Surg Ye M Zhang H Huang X Shi Y Yao Q Zhang L Zhang J 84895820132380625310.1016/j.jvs.2013.03.038 · doi ↗ · pubmed ↗
- 4Recanalization of superficial femoral artery chronic total occlusion through retrograde popliteal approach recanalization of superficial femoral artery chronic total occlusion Heliyon Jiang C Zhao Y Zhang WW Chen Z Zeng Q Li F 010202410.1016/j.heliyon.2024.e 30872 PMC 1114059538828305 · doi ↗ · pubmed ↗
- 5Retrograde popliteal approach for endovascular revascularization of flush superficial femoral artery chronic total occlusion: a two-center experience Indian J Vasc Endovasc Surg Singh A Prakash N Kumar N 424782021 https://journals.lww.com/ijvs/fulltext/2021/08010/retrograde_popliteal_approach_for_endovascular.9.aspx
- 6Hybrid procedures for patients with critical limb ischemia and severe common femoral artery atherosclerosis Ann Vasc Surg Matsagkas M Kouvelos G Arnaoutoglou E Papa N Labropoulos N Tassiopoulos A 106310692520112202394110.1016/j.avsg.2011.07.010 · doi ↗ · pubmed ↗
- 7Mayo Clinic Laboratories Test Cataloghttps://www.mayocliniclabs.com/test-catalog
- 8Risk factors for wound infections after vascular surgery: Kuwait experience Med Princ Pract Al Fawaz AA Safar AH Al-Mukhaizeem A Kamal E Alloush M Hanbal E 3923983120223558870810.1159/000525158 PMC 9485949 · doi ↗ · pubmed ↗