Pertussis-Associated Myocarditis in an Adolescent: A Case Report
Noora AlSuwaidi, Bosaina Otour, Amer Salman

TL;DR
A 16-year-old male developed myocarditis from a rare Bordetella pertussis infection, presenting with unusual symptoms like abdominal pain and rash.
Contribution
This paper reports a rare case of pertussis-associated myocarditis in an adolescent with atypical clinical presentation.
Findings
The patient had confirmed B. pertussis infection and acute myocarditis without typical respiratory symptoms.
Adolescent pertussis myocarditis is exceptionally rare with variable presentations but generally good outcomes.
No causal link has been established between pertussis vaccines and myocarditis.
Abstract
Myocarditis is an uncommon complication of infectious diseases in children, most often viral in origin. Bordetella (B.) pertussis infection rarely causes myocardial involvement, with very few cases reported in the literature and even fewer in adolescents. We describe a rare case of acute myocarditis in a previously healthy 16-year-old male with confirmed B. pertussis infection, who presented atypically with abdominal pain and rash in the absence of a characteristic pertussive cough. Review of prior reports suggests pertussis myocarditis in adolescents is exceptionally rare, with variable presentations but generally favorable outcomes. While myocarditis has also been reported extremely rarely following pertussis-containing vaccines, no causal relationship has been established. This case highlights the importance of considering pertussis in the differential diagnosis of myocarditis, even…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
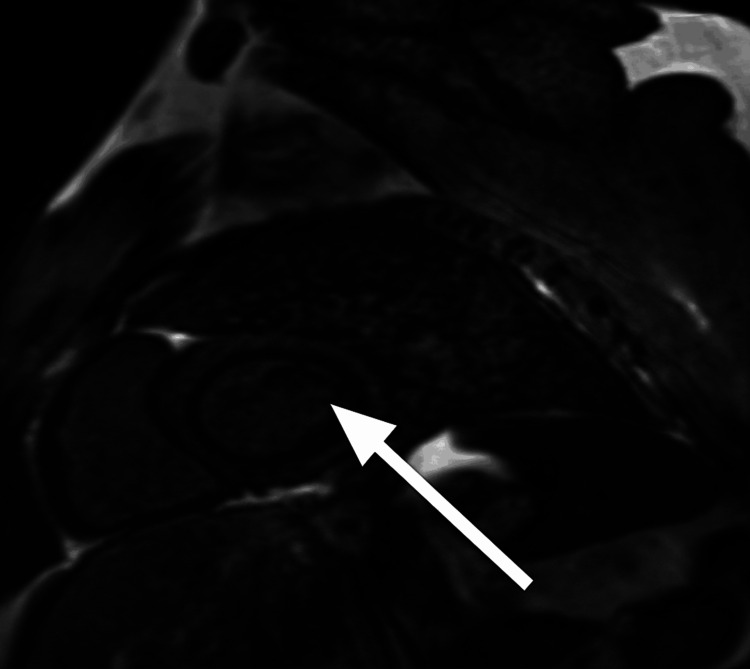 Figure 1
Figure 1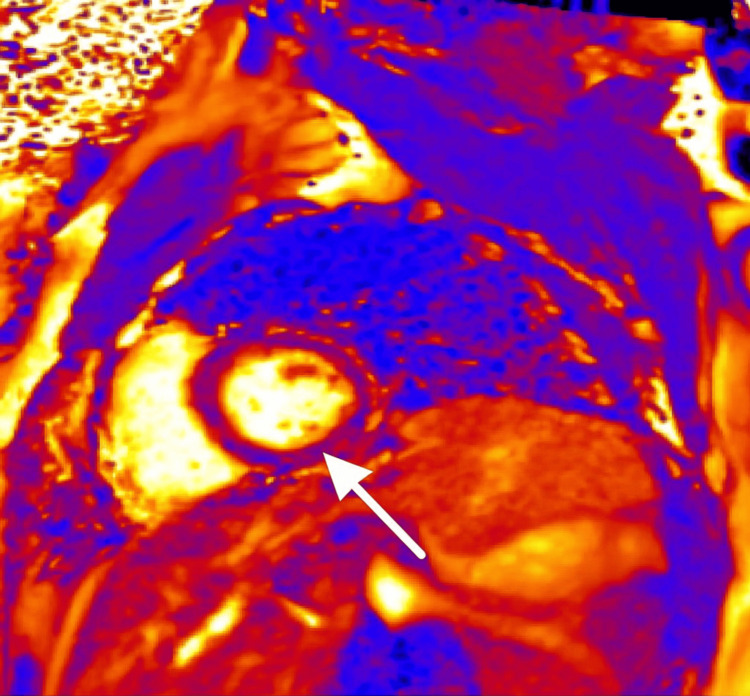 Figure 2
Figure 2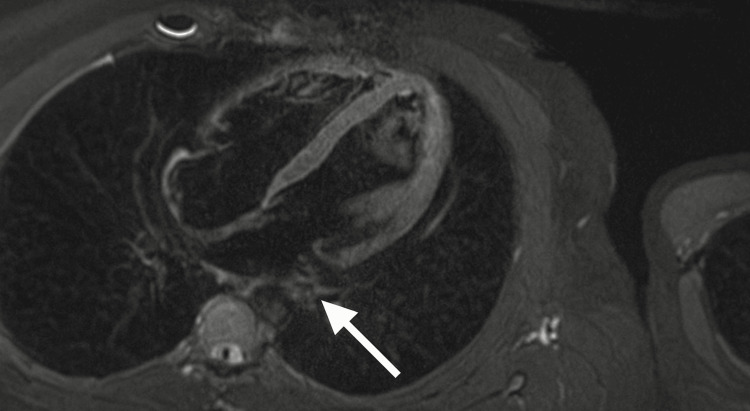 Figure 3
Figure 3| Parameter | Result | Reference Range |
| WBC | 8.2 × 10⁹/L | 4.0–11.0 × 10⁹/L |
| Lymphocytes | 3.26 × 10⁹/L | 1.0–4.0 × 10⁹/L |
| Hemoglobin | 15.9 g/dL | 12.0–17.5 g/dL |
| Platelets | 261 × 10⁹/L | 150–400 × 10⁹/L |
| CRP | 33.7 mg/L | 0–5 mg/L |
| Troponin I | 3.16 ng/mL | <0.04 ng/mL |
| Troponin T | 233 ng/L | <14 ng/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral Infections and Immunology Research · Infective Endocarditis Diagnosis and Management · Antimicrobial Resistance in Staphylococcus
Introduction
Pertussis, a respiratory infection caused by Bordetella pertussis, persists as a global health concern even with widespread immunization programs [1]. While classic symptoms include paroxysmal cough, inspiratory whoop, and post-tussive vomiting, these features may not always be present in adolescents and adults, leading to diagnostic challenges [2]. Severe complications predominantly occur in infants, with cardiac involvement being particularly uncommon across all age groups [3]. Previous literature mainly documents cases of pertussis-associated myocarditis in neonates and young infants, often resulting in poor clinical outcomes such as cardiogenic shock and dilated cardiomyopathy. Adolescents with myocarditis related to pertussis infection are scarcely reported, often only as rare consequences of vaccination, with insufficient evidence linking causality. Proposed mechanisms underlying pertussis-associated myocarditis include direct myocardial injury from toxins produced by Bordetella pertussis, immune-mediated myocardial inflammation, and microvascular coronary dysfunction leading to perfusion abnormalities [4-6]. This case report highlights an atypical presentation of acute myocarditis in an adolescent with confirmed pertussis infection, manifesting as abdominal pain and rash, thereby broadening the known clinical spectrum.
Case presentation
A previously healthy, 16-year-old male presented to the emergency department with a 1-day history of lower abdominal pain, chest pain, and shortness of breath. On the same day, he developed a generalized pruritic rash and a tactile fever. Two days earlier, he had experienced a sore throat and two episodes of non-bilious vomiting. Notably, there was no history of cough prior to or during hospitalization [2]. Upon examination, the patient was afebrile with a temperature of 36.5 °C, a respiratory rate of 18/min, oxygen saturation of 100% on room air, and a blood pressure of 118/75 mmHg. Both cardiovascular and respiratory examinations were unremarkable. Abdominal examination revealed right iliac fossa tenderness without signs of peritonism. A faint erythematous maculopapular rash was observed scattered across his trunk and upper limbs. Laboratory investigations revealed (Table 1).
Imaging studies showed widespread ST elevation on the initial ECG. Abdominal ultrasound was inconclusive due to poor visualization of the appendix and showed no evidence of lymphadenitis or free fluid. Echocardiography revealed moderate left ventricular dysfunction with an ejection fraction (EF) between 41% and 46%. CT coronary angiography demonstrated limited right coronary artery perfusion with suboptimal opacification but did not reveal structural anomalies. Respiratory PCR detected Bordetella pertussis (cycle threshold: 28); other respiratory pathogens were negative. Blood cultures remained sterile. Initial management focused on suspected appendicitis, but the patient was transferred to cardiology after laboratory and imaging findings revealed myocarditis. Azithromycin 500 mg orally daily for five days was given as per the pertussis protocol. No inotropes, angiotensin-converting enzyme (ACE) inhibitors, or beta-blockers were required during hospitalization. Serial echocardiograms showed progressive improvement in left ventricular function, with EF rising to 55% at two weeks and normalizing to 62% at six weeks. At the two-month outpatient follow-up, he remained asymptomatic with no complications [3,7].
Cardiac magnetic resonance imaging (MRI)Short-axis view showing the left ventricle with myocardial involvement (arrow).
Representative cardiac MRI slices are shown in Figures 1-3.
Cardiac magnetic resonance imaging (MRI), delayed TRUFI PSIR, short-axis viewDemonstrating late gadolinium enhancement with epicardial involvement in the inferolateral midventricle, consistent with myocarditis (arrow).TRUFI = true fast imaging with steady-state free precession; PSIR = phase-sensitive inversion recovery
Cardiac magnetic resonance imaging (MRI), T2-weighted four-chamber viewUseful for assessing myocardial edema. No active myocardial edema is seen, supporting the absence of acute inflammation (arrow).
Discussion
Myocarditis in childhood is most often triggered by viral agents, with bacterial etiologies representing a minority [1]. Bordetella pertussis-related myocarditis has been documented mainly in neonates and infants; adolescent cases are exceedingly rare and, when described, tend to be temporally associated with vaccination rather than confirmed infection [7]. This report is unique, as it documents acute myocarditis of clear pertussis etiology in an adolescent, with an atypical clinical presentation. Absence of cough in this patient is notable since it deviates from classic pertussis presentations. Hypotheses for this atypical manifestation include partial vaccine-derived immunity masking upper respiratory symptoms, systemic immune activation predominating over airway inflammation, or a greater tendency toward cardiac involvement in older children. The abdominal pain could plausibly stem from diaphragmatic irritation, mesenteric lymphadenitis secondary to pertussis, or hypoperfusion related to LV dysfunction. Pruritic rash, seldom described in previous reports, likely reflects immune-mediated systemic inflammation [2,6]. Diagnosis was supported by elevated cardiac biomarkers, confirmatory echocardiographic and CT findings, and PCR identification of the pathogen. Cardiac MRI, the gold standard for diagnosing myocarditis, was unfortunately unavailable, representing a limitation [6]. Nevertheless, clinical, laboratory, and molecular data provided a robust basis for pertussis-related myocarditis. Therapeutically, most adolescent patients recover with antimicrobial therapy and supportive management. Although myocarditis cases following pertussis vaccination are reported, their rarity and lack of mechanistic evidence argue against a causal link, emphasizing infection as the higher risk [8,9]. Vaccination remains pivotal for protection against severe sequelae such as myocarditis [1]. Recent literature continues to support recovery and atypical presentation in adolescent cases [7].
Conclusions
Pertussis-associated myocarditis in adolescents is exceedingly rare. This case is notable for its atypical presentation--abdominal pain and rash without cough--which delayed recognition. Clinicians should maintain a broad differential when assessing adolescents with chest pain, elevated cardiac markers, and unusual features. Early cardiac evaluation and pathogen identification guide management. While myocarditis is sporadically reported post-vaccination, overwhelming evidence supports vaccination for the prevention of severe pertussis-related morbidity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diagnosis and management of myocarditis in children: a scientific statement from the American Heart Association Circulation Law YM Lal AK Chen S 035144202110.1161/CIR.000000000000100134229446 · doi ↗ · pubmed ↗
- 2Pertussis in young infants throughout the world Clin Infect Dis Cherry JD 02263201610.1093/cid/ciw 550PMC 510662227838663 · doi ↗ · pubmed ↗
- 3Clinical practice. Pertussis--not just for kids N Engl J Med Hewlett EL Edwards KM 1215122235220051578849810.1056/NEJ Mcp 041025 · doi ↗ · pubmed ↗
- 4Pertussis toxin and adenylate cyclase toxin: key virulence factors of Bordetella pertussis and cell biology tools Future Microbiol Carbonetti NH 455469520102021055410.2217/fmb.09.133PMC 2851156 · doi ↗ · pubmed ↗
- 5Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases Eur Heart J Caforio AL Pankuweit S Arbustini E 263626482636-48, 2648 a-2648 d 3420132382482810.1093/eurheartj/eht 210 · doi ↗ · pubmed ↗
- 6Cardiovascular magnetic resonance in nonischemic myocardial inflammation: expert recommendations J Am Coll Cardiol Ferreira VM Schulz-Menger J Holmvang G 315831767220183054545510.1016/j.jacc.2018.09.072 · doi ↗ · pubmed ↗
- 7Dilated cardiomyopathy secondary to Bordetella pertussis infection in a 4-month-old: a case report Acta Pediatr Mex Clavero-Adell M Palanca-Arias D Ayerza Casas A López-Ramón M Jiménez-Montañés L 2125412020
- 8Myocarditis following diphtheria, whole-cell pertussis, and tetanus toxoid vaccination in a young infant Ann Pediatr Cardiol Kumar V Sidhu N Roy S Gaurav K 2242261120182992202810.4103/apc.APC_107_17PMC 5963245 · doi ↗ · pubmed ↗