Pemigatinib for previously treated metastatic or unresectable central nervous system tumors with fibroblast growth factor receptor mutations or rearrangements: FIGHT-207 results
Iben Spanggaard, Marc Matrana, Caio Rocha Lima, Amit Mahipal, Maria Vieito, Alice Hervieu, Lipika Goyal, Jordi Rodón, Maria Luisa Veronese, Natalia Oliveira, Xin Li, Michael Schaffer, Santosh Kesari

TL;DR
This study shows pemigatinib, an FGFR inhibitor, has some effectiveness and manageable safety in treating brain tumors with FGFR gene changes.
Contribution
The study is the first to evaluate pemigatinib in CNS tumors with FGFR alterations.
Findings
Three out of 13 patients with CNS tumors showed objective responses to pemigatinib.
Safety profile of pemigatinib was consistent with prior findings in other tumor types.
Patients with FGFR3-TACC3 fusions were the most common subgroup in the study.
Abstract
Central nervous system (CNS) tumors often harbor alterations in genes regulating key cellular pathways, including fibroblast growth factor receptor (FGFR) genes. Here, we report the efficacy and safety of treatment with pemigatinib, an oral, potent, selective FGFR1-3 inhibitor, in patients with advanced FGFR-altered CNS tumors. FIGHT-207 was a single-arm, open-label, phase 2 study of pemigatinib in patients with advanced solid tumors harboring FGFR fusions/rearrangements or other mutations. Patients received pemigatinib 13.5 mg once daily until disease progression or unacceptable toxicity. Endpoints included tumor response and safety. Of the 13 patients with CNS tumors in FIGHT-207, 10 had glioblastoma. Fibroblast growth factor receptor alterations were FGFR3-TACC3 fusions (n = 9), FGFR1 K656E mutations (n = 2), FGFR1 N546K mutation (n = 1), and FGFR1-MITF fusion (n = 1). Three patients…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
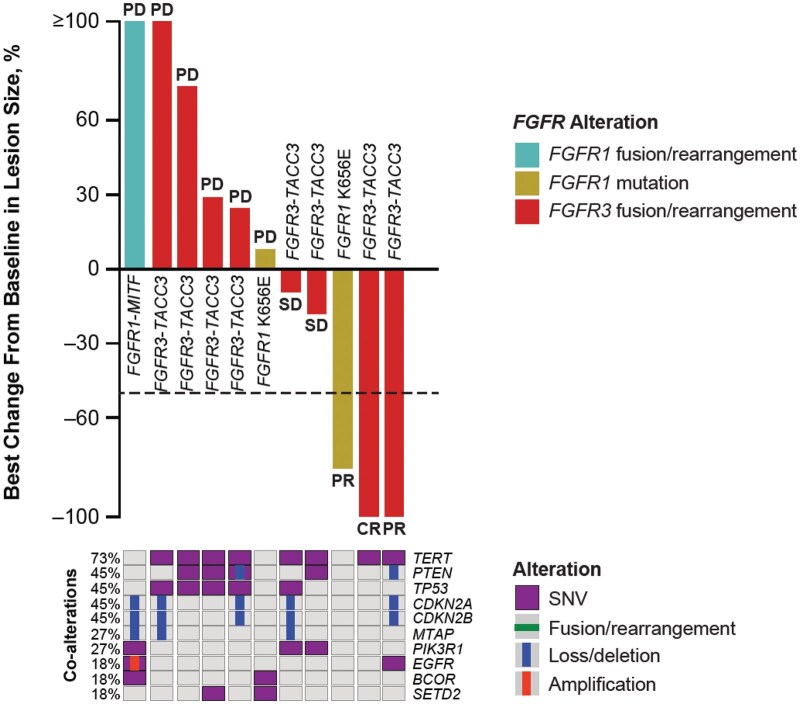 Figure 1
Figure 1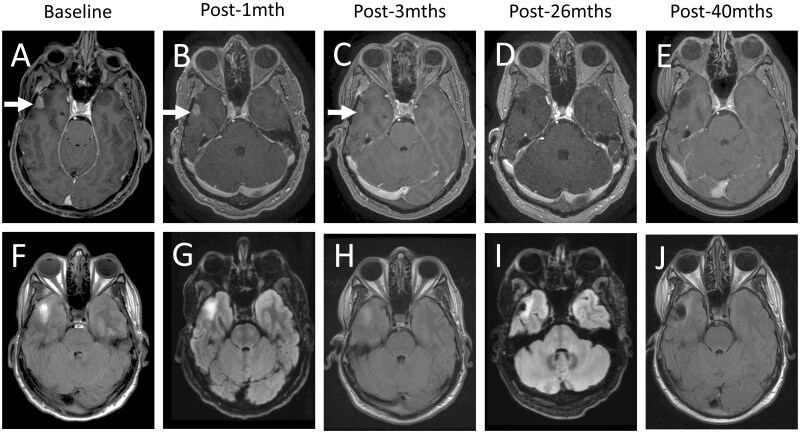 Figure 2
Figure 2- —American Academy of Neurology Annual Meeting
- —Incyte Corporation10.13039/100017655
- —Incyte Corporation10.13039/100017655
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFibroblast Growth Factor Research · Cancer, Hypoxia, and Metabolism · Microtubule and mitosis dynamics
Brief communication
Pemigatinib, an oral, potent, selective fibroblast growth factor receptor (FGFR)1-3 inhibitor, was evaluated in FIGHT-207, a phase 2 basket study in patients with previously treated, unresectable or metastatic solid tumors harboring FGFR fusions/rearrangements, activating single nucleotide variants (SNV) excluding kinase domain mutations, or variants of unknown significance (VUS). Patients received pemigatinib at starting dose of 13.5 mg once daily until disease progression or unacceptable toxicity. The FIGHT-207 results were recently published.1 Pemigatinib demonstrated antitumor activity in central nervous system (CNS), gynecologic, and pancreatic tumors, in addition to cholangiocarcinoma.
Molecular profiling of CNS tumor tissue has revealed genomic alterations, including oncogenic FGFR alterations, that may be appropriate for treatment with targeted therapies. The most prevalent FGFR alterations in gliomas (the most common malignant CNS tumors2) are FGFR3 rearrangements and FGFR1 mutations.3 Pemigatinib is approved to treat cholangiocarcinomas with FGFR2 fusions or alterations and myeloid/lymphoid neoplasms with FGFR1 rearrangement.4 The antitumor activity of pemigatinib for challenging-to-treat CNS tumors was previously unknown. Here, we highlight the efficacy, safety, and translational findings from the subset of patients with CNS tumors enrolled in FIGHT-207.
Of the 107 efficacy-evaluable patients enrolled in FIGHT-207, 13 patients had unresectable or metastatic CNS tumors. Of these, one patient with no prior treatment was permitted to enroll in FIGHT-207 because no treatment deemed of benefit existed for the patient’s tumor type. Ten patients harbored FGFR fusions and rearrangements and 3 had FGFR kinase domain mutations or VUS. Median (range) age was 60.0 (43-71) years, 61.5% were women, and 76.9% were White. Central nervous system tumors were classified as glioblastoma (GBM; n = 10, 76.9%), polymorphous low-grade neuroepithelial tumor of the young (PLNTY; n = 1, 7.7%), diffuse astrocytoma grade 2 (n = 1, 7.7%), and low-grade pediatric type glioma (n = 1, 7.7%). Most patients had prior radiation (n = 10), surgery (n = 10), and systemic therapies (n = 9). Fibroblast growth factor receptor alterations included FGFR3-TACC3 fusions (n = 9), FGFR1 K656E mutations (n = 2), FGFR1 N546K mutation (n = 1), and FGFR1-MITF fusion (n = 1).
Five patients (38.5%) experienced a reduction from baseline in target lesion size with pemigatinib treatment (Figure 1). Three (23%) patients had objective response per Response Assessment in Neuro-Oncology (complete response [CR], n = 1; partial response [PR], n = 2) and 3 (23%) patients had stable disease (SD; for 1 patient with SD, no target lesion measurement was available). The patient with CR had unmethylated GBM with an FGFR3-TACC3 fusion. Time to response was 4.4 months, and the duration of response was 15.9 months (Figure 2). No patient deaths were observed at the time of database lock and overall survival (OS) was censored at 20.2 months. Analysis of tumor tissue from the patient with CR indicated an unmethylated MGMT promoter. One patient with PR had GBM with a methylated MGMT promoter and an FGFR3-TACC3 fusion. The second patient had a diffuse astrocytoma grade 2, with an FGFR1 K656E mutation. Two of the 3 patients with SD harbored FGFR3-TACC3 fusions. In these 2 patients, progression-free survival (PFS) was 3.7 and 4.1 months, and OS was 6.1 and 13.3 months. The third patient with SD, who had an FGFR1 N546K mutation and had not received prior systemic therapy, experienced PFS and OS of 6.2 and 6.3 months, respectively. This patient was initially diagnosed with pediatric low-grade glioma and had received surgery as the only prior therapy. It should be noted that harboring a potentially actionable genetic alteration does not guarantee targeted treatment efficacy, and the best option for these patients at primary diagnosis may be the current standard of care.
Best percent change from baseline, best overall response, and co-alterations at baseline in patients with CNS tumors. Best percent change from baseline by RANO for all evaluable patients with CNS tumors; best overall response by IRC indicated where evaluable. Two patients were excluded: No target lesion measurement was available (n = 1), and no IRC response assessments were available (n = 1). Baseline co-alterations are from local reports, central FMI, and baseline Predicine ctDNA data. The dashed line indicates a criterion for PR per RANO (≥50% decrease in target lesion size). CNS, central nervous system; CR, complete response; ctDNA, circulating tumor DNA; FGFR, fibroblast growth factor receptor; FMI, Foundation Medicine, Inc.; IRC, independent review committee; PD, progressive disease; PR, partial response; RANO, Response Assessment in Neuro-Oncology; RECIST, Response Evaluation Criteria in Solid Tumors; SD, stable disease; SNV, single nucleotide variant. One patient had 100% tumor shrinkage (CR) for the target lesion, but had SD for a non-target lesion, and so was classified as having PR.
Brain MRIs showing durable complete response for patient. Patient with recurrent right temporal glioblastoma failing chemoradiation with 7 cycles of adjuvant temozolomide with Optune® device, then re-resected gross total resection confirmed active glioblastoma, and subsequently progressed after 2 cycles of lomustine before starting pemigatinib on study. A-E: axial post-gadolinium MRI T1 sequences showing resolution of enhancing temporal mass over time; F-J: axial MRI T2/FLAIR sequences showing the resolution of edema over time.
In our analysis, most patients had FGFR3-TACC3 fusions (n = 9; 8 patients with GBM, 1 patient with PLNTY), with the remaining patients exhibiting FGFR1 mutations (K656E, n = 2, 1 patient with GBM, 1 patient with diffuse astrocytoma grade 2; N546K, n = 1, patient had other glioma) and an FGFR1-MITF fusion (n = 1, patient had GBM). TERT SNVs were the most common co-alterations in this patient population with a frequency of 73% and 90% in patients overall and with FGFR3-TACC3 fusions, respectively. TERT mutations have been reported in nearly 80% of the patients with GBM.5 The incidence of TERT co-alterations in our study was generally consistent with the literature. In our study, the extent to which the identified co-alterations impacted clinical outcomes in patients with CNS tumors with FGFR alterations remains unclear.
Full safety data for patients in FIGHT-207 have been previously published.1 The safety of pemigatinib in patients with CNS tumors was consistent with the overall FIGHT-207 population. All patients in FIGHT-207 and in the CNS-tumor subgroup experienced treatment-emergent adverse events (TEAEs); hyperphosphatemia was the most common TEAE (FIGHT-207 overall, 83.8%; FIGHT-207 CNS, 84.6%). In the CNS-tumor subgroup, TEAEs were grade ≥3 in 76.9% of patients and led to dose reduction, treatment interruption, or discontinuation in 38.5%, 76.9%, and 15.4%, respectively. The most common grade ≥3 TEAEs related to pemigatinib were nail changes/disorders (n = 3) and stomatitis (n = 2). Treatment-emergent adverse events leading to pemigatinib discontinuation were spinal cord compression (n = 1) and pancreatitis (n = 1). One patient had a fatal TEAE (sepsis), which was not considered to be related to pemigatinib.
In summary, treatment with pemigatinib demonstrated antitumor activity and manageable TEAEs in patients with CNS tumors harboring FGFR fusions and kinase domain mutations. These findings warrant confirmation in the ongoing phase 2 FIGHT-209 study (NCT05267106) of pemigatinib in patients with recurrent GBM and other CNS tumors with activating FGFR1-3 mutations or fusions/rearrangements.6 The findings from FIGHT-209 will provide additional data concerning the use of pemigatinib in patients with CNS tumors and susceptible FGFR alterations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rodón J , Damian S, Furqan M, et al. Pemigatinib in previously treated solid tumors with activating FGFR 1-FGFR 3 alterations: phase 2 FIGHT-207 basket trial. Nat Med. 2024;30:1645-1654.38710951 10.1038/s 41591-024-02934-7PMC 11186762 · doi ↗ · pubmed ↗
- 2Ostrom QT , Francis SS, Barnholtz-Sloan JS. Epidemiology of brain and other CNS tumors. Curr Neurol Neurosci Rep. 2021;21:68.34817716 10.1007/s 11910-021-01152-9PMC 8613072 · doi ↗ · pubmed ↗
- 3Murugesan K , Necchi A, Burn TC, et al. Pan-tumor landscape of fibroblast growth factor receptor 1-4 genomic alterations. ESMO Open. 2022;7:100641.36462464 10.1016/j.esmoop.2022.100641 PMC 9832751 · doi ↗ · pubmed ↗
- 4PEMAZYRE ® (Pemigatinib). Full Prescribing Information, Incyte Corporation, Wilmington, DE, USA, 2022.
- 5Olympios N , Gilard V, Marguet F, et al. TERT promoter alterations in glioblastoma: a systematic review. Cancers (Basel). 2021;13:1147.33800183 10.3390/cancers 13051147 PMC 7962450 · doi ↗ · pubmed ↗
- 6Ahluwalia M , Franceschi E, Veronese L, et al. CTNI-39. FIGHT-209: a phase 2, open-label, multicentre study of pemigatinib in patients with previously treated glioblastoma or other primary central nervous system tumors with activating FGFR 1-3 alterations. Neuro Oncol. 2022;24:vii 80.