Advanced age and elevated cholesterol predict diabetic neuropathy in patients with type II diabetes mellitus in Southern Ethiopia
Fasika Merid, Habtamu Esubalew, Tamirat Gezahegn Guyo, Firdawek Getahun

TL;DR
This study identifies advanced age and high cholesterol as risk factors for diabetic neuropathy in type II diabetes patients in Ethiopia.
Contribution
The study identifies advanced age and elevated cholesterol as novel predictors of diabetic neuropathy in type II diabetes patients in Southern Ethiopia.
Findings
The incidence density of diabetic neuropathy was 3.56 cases per 1,000 person months.
Advanced age and total cholesterol ≥ 200 mg/dl were significant predictors of diabetic neuropathy.
The median time to develop diabetic neuropathy was 105 months.
Abstract
Diabetic neuropathy is the debilitating most common and expensive complication of diabetes that can cause significant mortality and morbidity, resulting from foot ulceration, lower extremity amputation, and pain that reduces the quality of life. The majority of type II diabetes mellitus patients continue to develop diabetic neuropathy despite optimal glycemic control, and the identification of predictors for diabetic neuropathy is important. Thus, this study aimed to determine the predictors of diabetic neuropathy in patients with type II diabetes mellitus in Ethiopia. A hospital-based retrospective longitudinal follow-up study was conducted from January 2012 to December 2021 in patients with type II diabetes. Simple random sampling was used to select study participants, and data were collected by reviewing the medical records. Stata version 14 was used for the statistical analysis. A…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
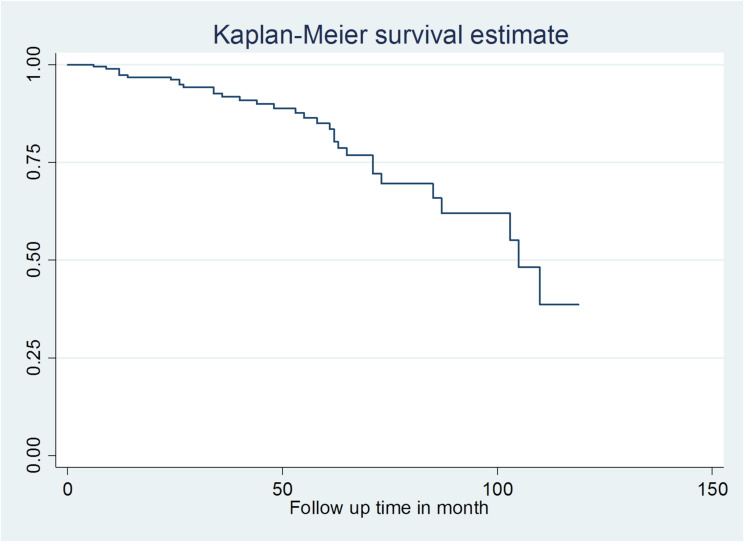 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPain Mechanisms and Treatments · Diabetes, Cardiovascular Risks, and Lipoproteins · Diabetic Foot Ulcer Assessment and Management
Introduction
Diabetes has reached alarming levels and remains a major public health concern [1]. Worldwide, more than half a billion people live with diabetes [1, 2]. Type 2 diabetes accounts for 96% of all diabetes cases [2]. By 2040, the prevalence of type 2 diabetes mellitus (DM) is projected to be 7,862 per 100,000 [3]. The alarming values indicate that type 2 diabetes has a worrisome future that varies according to geographical region, with above 80% of type 2 DM patients living in low and middle-income countries [4]. Complications of diabetes mellitus are distinguished as acute and chronic. For patients with diabetes, the biggest problem is the long-term complications, which include diabetic neuropathy [5].
Diabetic neuropathy is a subclinical or clinically manifested disease of the peripheral nerves that occurs as a consequence of DM without other underlying causes [6]. Diabetic neuropathy is the debilitating most common and expensive complication of diabetes that occurs in up to 50% of diabetic patients during their lifetime [7–9]. It is more common among patients with longstanding diabetes, after five years and at ten years 26% and 41% respectively have diabetic neuropathy [10]. A systematic review and meta-analysis revealed that the global prevalence of diabetic neuropathy was 35.78% among individuals with type 2 diabetes, 46% in Africa and 22% in Ethiopia among patients with diabetes [11–13]. Diabetic neuropathy can cause significant mortality and morbidity, resulting from foot ulceration, lower extremity amputation, and pain that reduces quality of life [8, 14–16]. Diabetic neuropathy is a leading cause of foot ulceration [17, 18]. During their lifetime around 25% of diabetes patients will experince foot ulceration [19]. Among diabetic neuropathy patients with foot ulceration, approximately 14 to 24% will require amputation [19]. Lower extremity amputation is 10–20% higher in patients with diabetes and more common in those with type 2 diabetes [20]. The 1 and 5 year mortality following lower limb amputation is between 10 and 50% and 30 to 80% respectively, representing a devastating impact that leads to a loss of function, financial stability, and quality of life [17]. Neuropathic pain is a major disabling consequence of diabetic neuropathy, and is estimated to affect ranging from 25 to 50% of patients with diabetes [16, 18, 21, 22]. Painful neuropathic symptoms cause significant suffering in patients, which commonly leads to anxiety, sleep disorders, depression, and a reduced quality of life and societal burden [16, 18, 23].
The incidence of diabetic neuropathy is greater in patients with T2DM [14, 15]. The most common predictors in previous studies for incidence were age, poor glycemic control, comorbid hypertension, and duration of diabetes [24–27]. The global epidemic of DM and its most common complication, diabetic neuropathy, necessitate a public health directive to address modifiable predictors with the rising urgency [15]. Early identification of diabetic neuropathy in clinical practice is essential for optimal therapeutic management and to modify any risk factors to reduce disease progression and complications [7, 14]. The majority of T2DM patients continue to develop diabetic neuropathy despite optimal glycemic control, and the identification of modifiable predictors for diabetic neuropathy is important [18]. Globally, comprehensive diabetes management has been established and practiced; all of these methods are not fully attainable, particularly in developing or low-income countries with relatively high rates of poverty [28]. Most of the studies on diabetic neuropathy originated from high-income countries [29]. Thus, this study aimed to determine the predictors of diabetic neuropathy in patients with type 2 diabetes mellitus in Ethiopia.
Methods and materials
Study design, period, and setting
A hospital-based retrospective longitudinal follow-up study was conducted in newly diagnosed patients with type 2 DM from 1^st^ January 2012 to 31^st^ December 2021 at Hawassa University Comprehensive Specialized Hospital (HUCSH).
Study populations and eligibility criteria
Patients with T2DM at HUCSH were the source population. Newly diagnosed patients with T2DM who were on follow-up during the study period at HUCSH were the study population. Newly diagnosed type II diabetes mellitus patients aged 18 years and above who were on follow-up in the study setting were included in the study. Those with unknown diagnosis dates, and those who had developed diabetic neuropathy at the time of T2DM diagnosis were excluded.
Sample size determination and sampling procedure and technique
The sample size was determined via Stata software version 14 power analysis on the basis of the following assumptions: α = 0.05, power = 80%, adjusted hazard ratio (AHR) = 2.78 from a previous study conducted [25], variability of covariates of interest = 0.5, probability of event = 0.1663, and a 0.1 proportion of withdrawals. The study’s final sample size was 201. Simple random sampling was used to select participants in a study from a sampling frame.
Study variables
Diabetic neuropathy was the dependent variable and the independent variables were sociodemographic characteristics (age, sex, residence), clinical and treatment-related characteristics (fasting blood sugar (FBS), hypertension, aneamia, duration of diabetes, diastolic blood pressure (DBP), systolic blood pressure (SBP), proteinuria, family history of DM, high-density lipoprotein (HDL), low-density lipoprotein (LDL), triglyceride, cholesterol, cardiovascular disease (CVD), nephropathy, retinopathy, and type of anti-diabetic treatment).
Operational definitions
Diabetic neuropathy: the presence of diabetic neuropathy diagnosed by physicians based on if there is a combination of two or more of the following sensory symptoms, decreased distal sensation, or unequivocally decreased or absent ankle reflexes and found in the patient’s medical record.
Event: diabetic neuropathy development within the follow-up period.
Censored: Those who did not develop diabetic neuropathy at the end of the study, loss to follow-up, died, or transferred out before diabetic neuropathy developing during the study period.
Data collection procedures and quality control
The data extraction checklist included sociodemographic characteristics, clinical, and treatment-related characteristics. The tool was developed after reviewing different studies. The data were collected by reviewing the medical records of T2DM patients who were on follow-up during the study period at HUCSH, Southern Ethiopia.
Before actual data collection training was given to the data collectors on how to retrieve records and the objective of the study. A pretest was conducted, and on the basis of the findings of the pretest; an adjustment was made to the data extraction checklist. Completeness and consistency were checked for the extracted data during the data collection period, and corrections were made accordingly.
Data processing and analysis
The data collected were entered using EpiData version 3.1 and for statistical analysis, Stata version 14 was used. Descriptive statistics, including median with interquartile range (IQR), mean with standard deviation (SD), and frequencies with percentages according to the type of variables were performed. A Kaplan-Meier (KM) survival curve was used to compare the survival time differences between categorical variables. A bivariable and multivariable Cox regression analysis was performed between the dependent and independent variables to identify predictors of diabetic neuropathy. A variable in the bivariate Cox regression analysis with a p-value less than 0.25 was used as a candidate for multivariable Cox regression analysis. In the multivariable Cox regression analysis, a p-value less than 0.05 was considered statistically significant. The mean-variance inflation factor was 1.02, which was used to check for multicollinearity. The Schoenfeld residuals test was used to check the assumption of Cox proportional hazard (Prob > chi^2^ = 0.7974). The goodness of fit of the model was checked via the Cox-Snell residual. The AHR with 95% CI and p-value was used to examine the strength of the association and statistical significance.
Results
Study participant characteristics
A total of 200 T2DM patients were included in the analysis. The study participants’ mean age was 48.73 years with an SD of ± 12.58. Almost three-fourths (72.5%) were urban residents. Among the study participants, nearly half (45%) had comorbid hypertension and 12% had cardiovascular disease. More than one-fourth (29%) of the participants had HDL cholesterol levels less than 40 mg/dl and more than one-third (35.5%) had total cholesterol levels ≥ 200 mg/dl. Among the total study participants, twenty-eight (14%) developed diabetic nephropathy. More than half (55%) of the study participants were on oral hypoglycemic agents (Table 1).
Table 1. Study participant characteristicsVariableCategoriesFrequency (%)AgeMean (SD) 48.73 ± 12.58SexMale106 (53.00)Female94 (47.00)ResidenceUrban145 (72.50)Rural55 (27.50)Fasting blood sugarMedian (IQR) 171.5 (74.5-268.5)HypertensionYes90 (45.00)No110 (55.00)Family history of DMYes69 (34.50)No131 (65.50)AnemiaYes11 (5.50)No189 (94.50)ProteinuriaPositive43 (21.50)Negative157 (78.50)Diabetic retinopathyYes10 (5.00)No190 (95.00)Cardiovascular diseaseYes24 (12.00)No176 (88.00)Triglyceride< 150 mg/dl122 (61.00)≥ 150 mg/dl78 (39.00)HDL< 40 mg/dl58 (29.00)≥ 40 mg/dl142 (71.00)LDL< 100 mg/dl138 (69.00)≥ 100 mg/dl62 (31.00)Total cholesterol< 200 mg/dl129 (64.50)≥ 200 mg/dl71 (35.50)TreatmentOral hypoglycemic agent110 (55.00)Insulin73 (36.50)Both17 (8.50)Diabetic nephropathyYes28 (14.00)No172 (86.00)Duration of T2DM< 5 years117 (58.50)≥ 5 years83 (41.50)
Incidence of diabetic neuropathy
Thirty-two (16.0%) patients with type 2 diabetes developed diabetic neuropathy with an incidence rate of 3.56 cases per 1,000 person months of observation with 95% CI (2.51, 5.03) in 8,999 person months of observation or 4.27 per 100 person year observations with 95% CI (3.01, 6.04). The median time to develop diabetic neuropathy was 105 months (Fig. 1). The cumulative survival probability was 89.56% at 48 months, 69.26% at 84 months, and 34.14% at 120 months.
Fig. 1. Overall Kaplan survival curve
Predictors of diabetic neuropathy
Age, family history of DM, aneamia, diabetic retinopathy, cardiovascular disease, and total cholesterol were significantly associated predictors with p-values less than 0.25 in the bivariable Cox proportional hazard regression analysis. In the multivariable Cox proportional hazard regression analysis age and total cholesterol were statistically significant predictors with p-values < 0.05. For a one year increase in age the hazard of developing diabetic neuropathy increases by 3% (AHR 1.03 (95% CI: 1.01, 1.06)). Type 2 diabetes patients whose total cholesterol level was ≥ 200 mg/dl had a 2.52 fold (AHR 2.52 (95% CI: 1.25, 5.09)) higher hazard of developing diabetic neuropathy than did those whose total cholesterol level was < 200 mg/dl (Table 2).
Table 2. Multivariable Cox regression analysis of predictors of diabetic neuropathyVariableCategoryEvent (%)Censored (%)CHR (95% CI)AHR (95% CI)Age1.03 (1.01, 1.06)1.03 (1.01, 1.06)Family history of DMYes8(4.00)61 (30.50)0.40 (0.17, 0.94)0.45 (0.19, 1.08)No24 (12.00)107 (53.50)11AnemiaYes4 (2.00)7 (3.50)2.07 (0.72, 6.00)2.32 (0.79, 6.84)No28 (14.00)161 (80.50)11Diabetic retinopathyYes5 (2.50)5 (2.50)2.49 (0.94, 6.59)1.64 (0.52, 5.21)No163 (81.50)27 (13.50)11Cardiovascular diseaseYes9 (4.50)15 (7.50)1.86 (0.85, 4.07)1.80 (0.81, 4.01)No23 (11.50)153 (76.50)11Total cholesterol< 200 mg/dl14 (7.00)115 (57.50)11≥ 200 mg/dl18 (9.00)53 (26.50)2.49 (1.24, 5.02)2.52 (1.25, 5.09)
Discussion
The current study aimed to determine the predictors of diabetic neuropathy in patients with type 2 diabetes mellitus. The overall incidence density of diabetic neuropathy was 3.56 cases per 1,000 person months. Age and total cholesterol were statistically significant predictors. The findings of this study have implications for physicians, program planners, policymakers, healthcare professionals, and the general public.
In our study, the incidence rate of diabetic neuropathy was 3.56 cases per 1,000 person month observation. The finding was higher than those of studies conducted in the United States of America 26.9 per 1000 person years [26], Gondar, Ethiopia 2.01 per 100 person years [25], and Northwest, Ethiopia 2.14 per 100 person year [24]. However, lower than those reported in studies done in Karachi, Pakistan 106.2 per 1000 person years [27] and Thailand 3.13 cases per 100 person months [30]. The difference might be due to the study setting, health care service provision, sample size, and duration of the follow-up period.
Advanced age strongly predicts the development of diabetic neuropathy among type 2 diabetes mellitus patients. The finding was in line with studies conducted in India [31], Indonesia [32], Gondar Ethiopia [25], China [33], and, North West Ethiopia [24]. A number of advanced age patients with diabetes mellitus progress to develop diabetic neuropathy [34]. During the aging process, several biological changes occur, which might be associated with the exacerbation with age including activation of advanced glycation end products, oxidative stress, an increase in inflammatory cells within peripheral nerve, aberrant cytokine expression, ischemia, and proinflammatory changes in the bone marrow [34, 35].
Patients with hypercholesterolemia had a higher hazard of developing diabetic neuropathy. The study finding supported by the studies done in Saudi Arabia and Bahrain [36, 37]. In patients with type 2 diabetes, there is a high incidence of dyslipidemia which is linked with diabetic neuropathy [18]. In diabetic neuropathy, lipids adversely affect the peripheral nervous system [15, 38]. The identified underlying mechanisms were the free fatty acid, plasma proteins, and oxidation of cholesterol to oxysterols that can cause injury [15, 18]. Elevated cholesterol along with glycemic control in the development of neuronal alterations should be monitored. Neurological alterations once started therapies depend on the progression of the disease [39].
Limitations of the study
Some variables, like occupational status, alcohol consumption, cigarette smoking and body mass index were unavailable and incomplete because of the retrospective nature of the study which was based on record review and was not considered in the analysis.
Conclusion
Age and total cholesterol were found to be independent predictors of diabetic neuropathy among patients with type 2 diabetes mellitus. Cholesterol level measurement for type 2 diabetes patients attending follow-up clinics needs to be undertaken regularly to delay and prevent the development of diabetic neuropathy, particularly in advanced-age patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1International Diabetes Federation. IDF Diabetes Atlas, 10th edn. Brussels, Belgium. 2021. Available online from: https://www.diabetesatlas.org
- 2Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet (London England). 2023;402(10397):203–34.10.1016/S 0140-6736(23)01301-6PMC 1036458137356446 · doi ↗ · pubmed ↗
- 3Galicia-Garcia U, Benito-Vicente A, Jebari S, Larrea-Sebal A, Siddiqi H, Uribe KB et al. Pathophysiology of type 2 diabetes mellitus. Int J Mol Sci. 2020;21(17).10.3390/ijms 21176275 PMC 750372732872570 · doi ↗ · pubmed ↗
- 4Gandhi M, Fargo E, Prasad-Reddy L, Mahoney KM, Isaacs D. Diabetes: how to manage diabetic peripheral neuropathy. Drugs Context. 2022;11.10.7573/dic.2021-10-2PMC 920556835775075 · doi ↗ · pubmed ↗
- 5Burgess J, Frank B, Marshall A, Khalil RS, Ponirakis G, Petropoulos IN et al. Early detection of diabetic peripheral neuropathy: a focus on small nerve fibres. Diagnostics (Basel Switzerland). 2021;11(2).10.3390/diagnostics 11020165 PMC 791143333498918 · doi ↗ · pubmed ↗
- 6Pop-Busui R, Ang L, Boulton AJM, American Diabetes Association. Diagnosis and treatment of painful diabetic peripheral neuropathy. Arlington (VA): 2022 Feb. Available from: https://www.ncbi.nlm.nih.gov/books/NBK 580224/10.2337/db 2022-0135544662 · pubmed ↗
- 7An J, Nichols GA, Qian L, Munis MA, Harrison TN, Li Z et al. Prevalence and incidence of microvascular and macrovascular complications over 15 years among patients with incident type 2 diabetes. BMJ Open Diabetes Res Care. 2021;9(1).10.1136/bmjdrc-2020-001847 PMC 778351833397671 · doi ↗ · pubmed ↗
- 8Alshammari NA, Alodhayani AA, Joy SS, Isnani A, Mujammami M, Alfadda AA et al. Evaluation of risk factors for diabetic peripheral neuropathy among Saudi type 2 diabetic patients with longer duration of diabetes. Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy. 2022:3007-14.10.2147/DMSO.S 364933 PMC 952761736200063 · doi ↗ · pubmed ↗