Serum level of monocyte chemotactic protein 1, N-terminal brain natural peptide in patients with coronary heart disease after nutritional changes
Yueyou Ding, Wenhui Ji, Hongchao Zheng, Zhancheng Wang

TL;DR
Combining Traditional Chinese Medicine with standard treatment reduces inflammation and improves symptoms in elderly patients with coronary heart disease.
Contribution
Demonstrates the complementary benefits of Baoyuan and Taohong Siwu decoctions in managing CHD.
Findings
Significant reductions in MCP-1 and NT-proBNP levels in the treatment group after 3 months.
Improved lipid profiles and greater symptom relief in patients receiving combined therapy.
Statistically significant differences in clinical outcomes between the treatment and control groups.
Abstract
Coronary heart disease (CHD) is a leading cause of morbidity among elderly populations, with inflammation and cardiac dysfunction indicated by elevated MCP-1 and NT-proBNP levels. This study evaluated the effects of integrating Traditional Chinese Medicine (Baoyuan and Taohong Siwu decoctions) with standard Western therapy on serum MCP-1 and NT-proBNP in elderly CHD patients. Results demonstrated significant reductions in these biomarkers, supporting the complementary role of TCM in managing CHD. A total of 90 elderly CHD patients were randomly allocated into two groups (n=45 each): the control group (CG), receiving conventional Western medicine alone, and the research group (RG), treated with BYD-THSWD combined with standard Western pharmacotherapy. Serum levels of MCP-1 and NT-proBNP, lipid profiles (TG, TC, LDL-C, HDL-C), and clinical symptoms (chest pain, chest tightness, fatigue,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
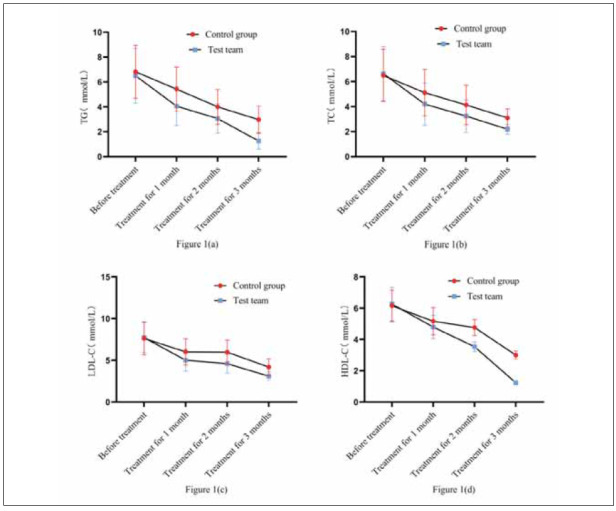 Figure 1
Figure 1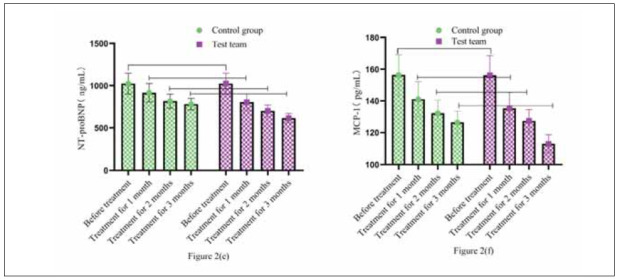 Figure 2
Figure 2| Group | n | Sex | Age<br>(year old) | BMI<br>(kg/m2) | Height (m) | Disease course<br>(year) | |
|---|---|---|---|---|---|---|---|
| Male | Female | ||||||
| CG | 45 | 26 | 19 | 62.49±1.27 | 23.54±2.06 | 1.67±0.15 | 3.56±1.16 |
| RG | 45 | 23 | 22 | 62.71±1.36 | 23.91±1.86 | 1.70±0.11 | 3.81±1.02 |
|
| 0.403 | 0.793 | 0.894 | 1.082 | 1.086 | ||
|
| 0.525 | 0.430 | 0.374 | 0.282 | 0.281 | ||
| Group | n | Merged underlying diseases | CHD grade | ||||
| Hypertension | Hyperlipidemia | Diabetes | Level | Level | Level | ||
| CG | 45 | 12 | 15 | 18 | 27 | 13 | 5 |
| RG | 45 | 14 | 11 | 20 | 23 | 15 | 7 |
|
| 0.875 | 0.796 | |||||
|
| 0.646 | 0.672 | |||||
| Group | n | Chest pain | Chest tightness | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Before | 1 month after | 2 months | 3 months after | Before | 1 month | 2 months | 3 months | ||
| CG | 45 | 2.48±0.48 | 2.01±0.34* | 1.87±0.30* | 1.69±0.19*#& | 2.51±0.38 | 1.99±0.25* | 1.81±0.17* | 1.65±0.14* |
| RG | 45 | 2.45±0.51 | 1.85±0.29* | 1.68±0.22* | 1.31±0.12*#& | 2.61±0.27 | 1.80±0.21* | 1.73±0.15* | 1.43±0.10* |
|
| 0.287 | 2.402 | 3.426 | 11.343 | 1.439 | 3.904 | 2.367 | 8.578 | |
|
| 0.775 | 0.018 | 0.001 | 0.000 | 0.154 | 0.002 | 0.020 | 0.000 | |
| n | Feeble | Sweating | |||||||
| Before | 1 month | 2 months | 3 months after | Before | 1 month | 2 months | 3 months after | ||
| CG | 45 | 2.71±0.26 | 1.98±0.23* | 1.76±0.15* | 1.51±0.11*#& | 2.44±0.71 | 1.93±0.54* | 1.78±0.43* | 1.34±0.34* |
| RG | 45 | 2.45±0.29 | 1.80±0.16* | 1.55±0.12* | 1.30±0.03*#& | 2.38±0.65 | 1.71±0.41* | 1.41±0.29* | 1.02±0.19* |
|
| 4.478 | 4.310 | 7.334 | 12.355 | 0.418 | 2.177 | 4.786 | 5.511 | |
|
| 0.000 | 0.000 | 0.000 | 0.000 | 0.677 | 0.032 | 0.000 | 0.000 | |
| Group | n | TG | TC | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Before | 1 month<br>after | 2 months<br>after | 3 months<br>after | Before | 1 month<br>after | 2 months<br>after | 3 months<br>after | ||
| CG | 45 | 6.82±2.13 | 5.42±1.78* | 4.00±1.39*# | 2.97±1.10*#& | 6.49±2.08 | 5.11±1.85* | 4.13±1.57*# | 3.10±0.72*#& |
| RG | 45 | 6.50±2.20 | 4.06±1.56* | 3.06±1.18*# | 1.26±0.67*#& | 6.63±2.17 | 4.20±1.69* | 3.24±1.31*# | 2.19±0.39*#& |
|
| 0.701 | 3.855 | 3.458 | 8.906 | 0.312 | 2.436 | 2.920 | 7.455 | |
|
| 0.485 | 0.000 | 0.001 | 0.000 | 0.755 | 0.017 | 0.004 | 0.000 | |
| n | LDL-C | HDL-C | |||||||
| Before | 1 month<br>after | 2 months<br>after | 3 months<br>after | Before | 1 month<br>after | 2 months<br>after | 3 months<br>after | ||
| CG | 45 | 7.63±1.99 | 6.00±1.57* | 5.97±1.45*# | 4.18±1.00*#& | 6.15±1.01 | 5.16±0.87* | 4.76±0.51*# | 3.00±0.26*#& |
| RG | 45 | 7.71±1.78 | 5.01±1.31* | 4.59±1.13*# | 3.10±0.51*#& | 6.26±1.07 | 4.79±0.75* | 3.53±0.31*# | 1.23±0.04*#& |
|
| 0.201 | 3.248 | 5.036 | 6.454 | 0.501 | 2.161 | 13.825 | 45.136 | |
|
| 0.841 | 0.002 | 0.000 | 0.000 | 0.617 | 0.033 | 0.000 | 0.000 | |
| Group | n | MCP-1 (pg/mL) | NT-proBNP (ng/mL) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Before | 1 month<br>after | 2 months<br>after | 3 months<br>after | Before | 1 month<br>after | 2 months<br>after | 3 months<br>after | ||
| CG | 45 | 156.34±<br>12.74 | 141.06±<br>11.06* | 132.18±<br>8.37*# | 126.38±<br>7.04*#& | 1024.52±<br>123.09 | 916.34±<br>110.34* | 816.39±<br>84.37*# | 781.28±<br>68.29*#& |
| RG | 45 | 156.19±<br>12.37 | 135.29±<br>10.09* | 127.34±<br>7.16*# | 113.09±<br>5.49*#& | 1024.37±<br>123.13 | 804.28±<br>98.74* | 700.25±<br>71.04*# | 614.28±<br>54.77*#& |
|
| 0.057 | 2.585 | 2.948 | 3.000 | 0.006 | 5.077 | 7.064 | 12.797 | |
|
| 0.955 | 0.011 | 0.004 | 0.004 | 0.995 | 0.000 | 0.000 | 0.000 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGDF15 and Related Biomarkers · Diet and metabolism studies
Introduction
Coronary heart disease (CHD) remains a leading cause of morbidity and mortality globally, particularly among elderly populations [1] [2] [3]. It is characterised by atherosclerotic narrowing of coronary arteries, causing myocardial ischemia and subsequent deterioration of cardiac function [4]. Aging populations often exhibit additional risk factors such as hyperlipidemia, hypertension, and diabetes mellitus, further complicating disease management [5]. Effective treatment strategies are essential to mitigate disease progression, improve cardiac function, and enhance the quality of life in elderly CHD patients [3].
Recent research has emphasised inflammation as a key pathogenic mechanism in the development and progression of CHD. Monocyte chemotactic protein-1 (MCP-1), a member of the C-C chemokine family, has attracted attention due to its pivotal role in recruiting monocytes to sites of inflammation, contributing to vascular damage and plaque formation [6]. Elevated MCP-1 levels have consistently been associated with increased risks of atherosclerosis, plaque vulnerability, and acute coronary events [7]. Additionally, MCP-1 is considered an early biomarker for predicting adverse cardiovascular outcomes, reflecting the severity of inflammation within coronary lesions [8].
Similarly, N-terminal pro-brain natriuretic peptide (NT-proBNP) is a widely recognised biomarkerreflecting cardiac dysfunction, particularly ventricular strain and volume overload [9]. NT-proBNP is secreted primarily from ventricular cardiomyocytes in response to myocardial stress and stretching, playing a crucial role in cardiovascular homeostasis by regulating natriuresis, diuresis, vasodilation, and inhibition of the renin-angiotensin-aldosterone system [10]. Previous studies have consistently demonstrated that elevated serum NT-proBNP levels are strong predictors of mortality, heart failure, and overall adverse cardiac events in CHD patients [11] [12]. Thus, measuring serum NT-proBNP levels is essential for assessing the cardiac function status and prognosis of patients with coronary heart disease.
Current therapeutic strategies for elderly CHD patients primarily involve pharmacological interventions such as antiplatelet agents, lipid-lowering drugs, and vasodilators, which aim to prevent thrombosis, manage dyslipidemia, and improve coronary circulation [13] [14]. Despite the efficacy of Western medicines, a significant number of elderly patients continue to experience recurrent angina, poor lipid control, and persistent inflammatory states, highlighting the need for integrated therapeutic approaches.
Traditional Chinese Medicine (TCM), mainly herbal decoctions, is increasingly employed as anadjunct therapy in cardiovascular disease treatment due to its multi-targeted therapeutic effects, minimal side effects, and potential for improving patients’ overall condition [15]. Among numerous TCM formulas, Baoyuan decoction (BYD) and Taohong Siwu decoction (THSWD) are particularly prominent. BYD primarily functions through invigorating qi, strengthening myocardial energy metabolism, and improving cardiac function. At the same time, THSWD is noted for its effects on invigorating blood circulation, eliminating blood stasis, reducing inflammation, and protecting myocardial cells [16] [17]. Clinical studies have indicated that these decoctions effectively improve symptoms such as chest tightness, fatigue, chest pain, and shortness of breath, significantly enhancing patient outcomes.
However, despite growing evidence supporting the clinical benefits of TCM in CHD management,there remains limited information on the specific biochemical changes induced by these nutritional and medicinal therapies. Particularly, the impact of BYDTHSWD combined with standard Western medicine on critical cardiovascular biomarkers, such as MCP-1 and NT-proBNP, has not yet been thoroughly explored or clearly defined.
The purpose of this study, therefore, was to examine the effect of nutritional modifications incorporating Baoyuan decoction and Taohong Siwu decoction in combination with standard Western pharmacotherapy on serum levels of MCP-1 and NT-proBNP in elderly patients diagnosed with coronary heart disease. Understanding how these traditional therapies influence inflammatory and cardiac biomarkers could provide insights into their potential mechanisms of action and inform clinical decisions regarding integrated treatments for improved cardiovascular outcomes in elderly CHD patients.
Materials and methods
Research subjects
This study involved 90 elderly patients diagnosed with coronary heart disease (CHD) whoreceived medical treatment at our institution from January 2023 to December 2024. Patients wereevenly divided into two treatment groups (45 patients per group). Demographic characteristics and clinical conditions – including gender distribution, average age, body mass index (BMI), height, duration and severity of CHD, presence of comorbid conditions, and CHD grading – were statistically comparable between the two groups (P>0.05), as detailed in Table 1.
Inclusion criteria
(A) Patients diagnosed with coronary heart disease meet established diagnostic standards as defined by current clinical guidelines (reference 7).
(B) Patients receiving pharmacological treatment for CHD for the first time at our medical centre.
(C) Traditional Chinese Medicine (TCM) diagnostic standards confirm that the patient’s condition is consistent with Qi deficiency and blood stasis syndrome.
(D) Clinical documentation indicating the initial administration of CHD medications that occurred at our institution is available.
(E) Patients exhibiting stable cardiac function classified at levels I–III according to NYHA classification guidelines.
Exclusion criteria
(A) History of acute myocardial infarction or unstable angina episodes within the last 6 months.
(B) Cardiac functional classification of IV or higher (indicating severe cardiac insufficiency).
(C) Documented chronic abuse of drugs or alcohol.
(D) Severe comorbid diabetes mellitus and hypertension that cannot be effectively managed or stabilised.
(E) Co-existing severe hemorrhagic conditions, severe cerebrovascular disease, or active malignancies.
(F) History of severe psychiatric disorders or other conditions affecting adherence and cooperation in medical treatment protocols.
Treatment protocols
Control Group (CG): Patients received standardised Western medical therapy, including:
Betaloc (Metoprolol): Oral dose of 25–50 mg administered twice daily.
Aspirin and lipid-lowering therapy: Patients received Betaloc at doses of 25–50 mg twice daily orally, Rosuvastatin 10–20 mg administered orally once nightly, and additional medications as clinically indicated.
Each therapeutic course lasted one month, with a total treatment duration of three consecutive months.
Research Group (RG): Patients in the RG received standard Western medications identical tothe Control Group, supplemented with the herbal formula BYD-THSWD tailored to Qi deficiency and blood stasis syndrome:
The BYD-THSWD prescription comprised:
Ophiopogon japonicus (20 g), Ligusticum wallichii (9 g), Astragalus membranaceus (20 g), Caulis spatholobi (15 g), Angelica sinensis (10 g), Radix liquiritiae (6 g), Safflower (10 g), Fried semen ziziphi spinosae (15 g), Semen ziziphi spinosae (fried, 15 g), Angelica sinensis (10 g), Ligusticum wallichii (9 g), Ophiopogon japonicus (20 g), and Safflower (10 g).
Additional herbal ingredients were customised based on presenting symptoms:
For patients experiencing pronounced fatigue, 15 g yam and 15 g fried Atractylodes macrocephala Koidz were included.
In cases of severe insomnia, 15 g tube of flueflower stem was added.
For significant chest tightness, 15 g Fructus Aurantii was supplemented.
The herbs were prepared through water decoction, with patients consuming one dose daily.
Evaluation indices and procedures
Clinical assessment criteria included:
Symptom severity scoring (0–3 scale): Patients were assessed for symptom severity in terms of clinical manifestations such as chest pain, shortness of breath, fatigue, and insomnia, as rated on a four-point scale ranging from 0 (no symptoms) to 3 (severe symptoms). Higher cumulative scores indicated more severe clinical presentations.
Blood lipid profiling: Fasting venous blood samples (3 mL) were collected in the morning to measure triglycerides (TG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C). Samples were analysed promptly post-collection.
Serum biomarkers of cardiac function and inflammation: Venous blood (5 mL) was drawn after overnight fasting to determine the levels of NT-proBNP and MCP-1. NT-proBNP was measured via electrochemiluminescence immunoassay (ECLIA), while MCP-1 levels were evaluated using enzyme-linked immunosorbent assay (ELISA) [18] [19].
Statistical analysis
Statistical analyses were conducted using SPSS software (version 26.0). Continuous data were expressed as mean ± standard deviation (x̄ ± s), while categorical data were presented as frequencies and percentages. Differences between groups were assessed using independent-sample t-tests for normally distributed continuous data. Chi-square tests were utilised to evaluate categorical variables. A p-value less than 0.05 (P<0.05) was defined as statistically significant, indicating meaningful differences between the two groups.
Results
The study involved 90 elderly patients diagnosed with coronary heart disease (CHD), with a mean age of approximately 62 years. Participants were randomly assigned to two groups: the control group (CG) receiving conventional Western medicine and the research group (RG) receiving a combination of Baoyuan and Taohong Siwu decoctions along with Western therapy. The baseline characteristics, including gender, body mass index (BMI), height, disease duration, and severity of CHD, were comparable between the two groups. Both groups included individuals with comorbid conditions such as hypertension, hyperlipidemia, and diabetes, with no significant differences in these conditions or the severity of CHD across groups. The study was conducted over a period from January 2023 to December 2024, and all participants provided informed consent to participate.
Comparison of baseline data
The demographic and clinical baseline characteristics of participants in both the control group (CG)and research group (RG) were comparable. There were no statistically significant differences between the two groups concerning gender distribution, age, BMI, height, duration of illness, prevalence of underlying diseases (hypertension, hyperlipidemia, diabetes), or coronary heart disease (CHD) severity grading (all P>0.05).
TCM symptom scores
Both groups had similar Traditional Chinese Medicine (TCM) symptom scores prior to treatment (P>0.05). However, after treatment at different time points, symptoms, including chest pain, chest tightness, fatigue, and sweating, significantly improved in both groups. Notably, the improvements were more significant in the RG compared with the CG at each time interval (1 month, 2 months, and 3 months after treatment), with statistically significant differences (P<0.05). Table 2 Table 3
**Table 2: TCM Symptom Scores for Two Groups (x̄±s, point).Note: * Compared with before treatment, P<0.05. # Compared with the 1-month treatment, P<0.05. #& Compared with the 2-month treatment, P<0.05.
**Table 3: TG, TC, LDL-C, and HDL-C (x̄±s, mmol/L).Note: * Compared with before treatment, P<0.05. # Compared with the 1-month treatment, P<0.05. #& Compared with the 2-month treatment, P<0.05.
Comparison of TG, TC, LDL-C, and HDL-C
Initially, no significant differences existed between RG and CG for triglycerides (TG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), or high-density lipoprotein cholesterol (HDL-C) (P>0.05). Post-treatment, both groups showed significant reductions in these lipid parameters. Notably, after 3 months of treatment, RG (treated with BYD-THSWD combined with Western medicine) exhibited significantly lower levels of TG, TC, LDL-C, and HDL-C compared to CG (treated with Western medicine alone) (all P<0.05).
Compared with CG treated with Western medicine alone, RG with BYD-THSWD showed a decreasein TG, TC, LDL-C, and HDL-C levels. Figure 1(a), Figure 1(b), Figure 1(c), and Figure 1(d) showed the trend changes of various indicators. Two groups had the same TG, TC, LDL-C, and HDL-C levels before treatment (P>0.05) and were treated for 1 and 2 months. After 3 months, the levels of TG, TC, LDL-C, and HDL-C in RG were lower than CG’s (P<0.05). Table 4
Comparison of TG, TC, LDL-C, and HDL-C.<br>Note: Figure 1(a) shows TG, Figure 1(b) shows TC, Figure 1(c) shows LDL-C, and Figure 1(d) shows HDL-C. The red circular curverepresents CG. The blue square curve represents RG. The curve fluctuation indicates the changes in various blood lipid indicators before and after treatment in both groups.
**Table 4: Comparison of NT-proBNP and MCP-1 (x̄±s).Note: * Compared with before treatment, P<0.05. # Compared with the 1-month treatment, P<0.05. #& Compared with the 2-month treatment, P<0.05.
Comparison of Serum Factors NT-proBNP and MCP-1
No significant differences in cardiac biomarkers (NT-proBNP and MCP-1) were observed between groups at baseline (P>0.05). After treatment durations of 1, 2, and 3 months, both groups displayed reductions in NT-proBNP and MCP-1. However, the RG experienced more pronounced decreases compared to the CG at all post-treatment time points, demonstrating statistically significant differences (all P<0.05). This indicates that combination therapy (BYD-THSWD plus Western medicine) provided greater benefits in reducing serum NT-proBNP and MCP-1 than Western medicine alone.
Compared to the control group (CG), which received only Western medicine, the research group (RG) treated with BYD-THSWD combined with Western medicine exhibited more significant reductions in serum NT-proBNP and MCP-1 levels. Figure 2(e) and Figure 2(f) illustrate the trends of these indicators throughout treatment. Initially, no significant differences were found between the two groups (P>0.05). However, after treatment at various time points, NT-proBNP and MCP-1 were significantly lower in RG than in CG (P<0.05) (Figure 2).
Comparison of serum factors NT-proBNP and MCP-1.<br>Note: Figure 2(e) shows NT-proBNP, and Figure 2(f) shows MCP-1. The green circular bar chart is CG. The purple square bar chart shows RG. The high and low levels of the bar chart represent the changes in various serum indicators before and after treatment in both groups.
Discussion
This study demonstrated that elderly patients with coronary heart disease (CHD) treated with acombination of Baoyuan decoction (BYD), Taohong Siwu decoction (THSWD), and standard Western medical therapy experienced significant improvements in both clinical symptoms and biochemical markers compared to those receiving Western medication alone. The primary findings included a marked reduction in serum levels of monocyte chemotactic protein-1 (MCP-1) and N-terminal probrain natriuretic peptide (NT-proBNP), along with substantial improvements in lipid profiles (TG, TC, LDL-C, HDL-C). Additionally, significant symptomatic relief, including decreased chest pain, chest tightness, fatigue, and sweating, was observed in the integrated therapy group. These results demonstrate that incorporating BYD-THSWD into conventional Western medicine can effectively enhance cardiac function, alleviate inflammation, and improve lipid metabolism. This suggests a beneficial adjunctive role for Traditional Chinese Medicine in managing elderly CHD patients.
The observed significant reduction in MCP-1 levels among patients receiving combined treatment aligns with the growing body of evidence highlighting the critical role of inflammation in CHD pathogenesis. Elevated MCP-1 is well-established as an early inflammatory marker predictive of increased cardiovascular risk, reflecting the active inflammatory status and plaque vulnerability within coronary arteries. By substantially decreasing MCP-1, BYD-THSWD appears to exert anti-inflammatory effects, potentially reducing atherosclerotic progression and enhancing plaque stability. The mechanism underlying this benefit may involve herbal components known for their anti-inflammatory and antioxidative properties, particularly Astragalus membranaceus and Angelica sinensis, which are integral constituents of the BYD-THSWD formula. Thus, the improvement in MCP-1 provides biochemical evidence supporting the clinical efficacy of BYD-THSWD in managing inflammatory responses associated with coronary heart disease.
In a study by Martín-Reyes et al. [20], elevated plasma levels of monocyte chemoattractant protein-1 (MCP-1) and N-terminal pro-brain natriuretic peptide (NT-proBNP) were independently associated with greater complexity of coronary artery disease (CAD), as measured by the Syntax Score. Additionally, low calcidiol (vitamin D metabolite) levels predicted more severe coronary artery calcification, indicating its role in mineral metabolism and CAD progression. Our findings align with these results, as we similarly observed elevated MCP-1 and NT-proBNP levels among elderly coronary heart disease (CHD) patients. Importantly, our study demonstrated that combining Traditional Chinese Medicine (Baoyuan and Taohong Siwu decoctions) with conventional Western treatment significantly reduced MCP-1 and NT-proBNP levels, improved lipid profiles, and alleviated clinical symptoms. While Martín-Reyes et al. highlighted biomarker associations, our findings suggest that integrative therapeutic approaches could actively reduce these markers and potentially impact CAD severity. Future studies should investigate the influence of TCM on biomarkers like calcidiol further to understand its therapeutic benefits in CAD management fully.
In a similar by Blanco-Colio et al. [21], elevated plasma levels of monocyte chemoattractant protein-1 (MCP-1) were significantly associated with recurrent cardiovascular events, particularly acute coronary syndrome and ischemic stroke, in patients with persistent inflammation indicated by elevated C-reactive protein. This finding underscores MCP-1’s role as a critical marker of cardiovascular risk, especially in inflammatory states. Similarly, our own research identified elevated MCP-1 and NT-proBNP as biomarkers indicating increased inflammation and cardiac dysfunction in elderly coronary heart disease (CHD) patients. Importantly, our intervention, which combined Traditional Chinese Medicine (Baoyuan and Taohong Siwu decoctions) with conventional Western therapy, successfully lowered MCP-1 and NT-proBNP levels, improved lipid profiles, and relieved clinical symptoms. This suggests that therapeutic targeting of inflammatory markers like MCP-1 through integrative approaches could potentially reduce recurrent cardiovascular events in patients with persistent inflammation, complementing and extending Blanco-Colio et al.’s findings by highlighting the clinical utility of integrated therapies.
Similarly, NT-proBNP levels significantly decreased in patients undergoing combined therapy compared to the control group, reinforcing the cardiac-protective effect of integrating BYD-THSWD with Western medication. NT-proBNP, a well-established biomarker for cardiac dysfunction, correlates strongly with myocardial stress and ventricular overload conditions. The greater reduction in NT-proBNP levels observed in the RG group highlights an improvement in cardiac function, possibly due to the multi-targeted cardiovascular protective effects of BYD-THSWD. Specifically, BYD is traditionally recognised for invigorating qi and enhancing myocardial energy metabolism, while THSWD promotes blood circulation, reduces blood stasis, and has cardioprotective and endothelial-reparative actions. Together, these herbal decoctions may mitigate myocardial remodelling and reduce ventricular strain, thus lowering NT-proBNP levels.
Furthermore, this study demonstrated notable improvements in lipid metabolism parameters, including triglycerides (TG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C) in patients receiving the integrated nutritional therapy. Dyslipidemia is a primary risk factor in CHD progression, and effective lipid control remains essential in therapeutic management strategies. The significant reductions in lipid profiles observed in patients treated with BYD-THSWD, beyond those receiving conventional therapy alone, suggest additional metabolic regulatory effects conferred by these decoctions. The lipid-lowering effects of BYD-THSWD may be attributed to components such as Ligusticum wallichii and Safflower, which have documented lipid-regulating and anti-atherosclerotic activities. These herbal components might inhibit lipid absorption, enhance lipid metabolism, or improve endothelial function, contributing to improved lipid profiles observed in this research.
Clinically, patients in the RG demonstrated superior improvements in symptomatology assessed by TCM scores, including reduced chest pain, chest tightness, fatigue, and sweating. These symptomatic improvements, coupled with biochemical evidence, further substantiate the holistic therapeutic potential of TCM decoctions. BYD-THSWD not only targets physiological pathways involved in inflammation, lipid metabolism, and cardiac function but also addresses patient-specific syndromes consistent with Qi deficiency and blood stasis in traditional diagnostic frameworks. This individualised approach enhances patient adherence and may offer broader quality-of-life improvements beyond those achieved by Western medication alone.
However, several limitations must be acknowledged. First, the sample size was relatively small, limiting generalizability and necessitating further studies with larger, more diverse populations. Second, the follow-up duration was limited to three months, precluding the assessment of long-term sustainability and its impact on cardiovascular outcomes, such as myocardial infarction incidence or cardiovascular mortality. Long-term follow-up studies are needed to clarify whether sustained reductions in MCP-1, NT-proBNP, and lipid levels translate into meaningful clinical benefits. Additionally, specific molecular mechanisms underlying the beneficial effects of BYD-THSWD were not elucidated in this investigation and warrant further exploration.
Conclusion
In conclusion, combining Baoyuan and Taohong Siwu decoctions with Western medicine effectively reduces inflammatory and cardiac biomarkers, improves lipid metabolism, and relieves symptoms in elderly CHD patients. This integrated approach offers a promising complementary therapy for managing coronary heart disease. Further studies are needed to explore its long-term benefits.
Dodatak
Acknowledgements
The authors would like to express their gratitude to the medical and nursing staff at Shanghai Eighth People’s Hospital, Huajing Community Health Service Centre, and Central Hospital of Xuhui District for their valuable assistance and support during the study. Special thanks also go to all participants who consented to take part in this research.
Funding
This research did not receive specific funding from any agencies in the public, commercial, or not-for-profit sectors.
Ethics statement
The study protocol was approved by the Ethics Committee of Shanghai Eighth People’s Hospital, and all participants provided informed written consent prior to enrollment. The ethical guidelines outlined in the Declaration of Helsinki were strictly followed.
Authors’ contributions
Z.W. conceived the study, supervised research activities, and provided overall direction. Y.W., W.J., and H.Z. performed data collection and conducted patient assessments and laboratory analyses. W.J. and Y.W. conducted statistical analyses and prepared the initial manuscript draft. Z.W. critically reviewed and revised the manuscript. All authors have read, revised, and approved the final manuscript.
Data availability
All relevant data supporting the findings of this study are available upon request from the corresponding author.
Conflict of interest statement
All the authors declare that they have no conflict of interest in this work.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 11111119202410.5334/gh.1288 di Cesare M Perel P Taylor S Kabudula C Bixby H Gaziano T A Mc Ghie D V Mwangi J Pervan B Narula J Pineiro D Pinto F J Glob Heart The Heart of the World 38273998 PMC 10809869 · doi ↗ · pubmed ↗
- 272211535201010.1016/j.cpcardiol.2009.10.002 Gaziano T A Bitton A Anand S Abrahams-Gessel S Murphy A Curr Probl Cardiol Growing Epidemic of Coronary Heart Disease in Low- and Middle-Income Countries 20109979 PMC 2864143 · doi ↗ · pubmed ↗
- 3256132564201610.21037/atm.2016.06.33 Sanchis-Gomar F Perez-Quilis C Leischik R Lucia A Ann Transl Med Epidemiology of coronary heart disease and acute coronary syndrome 27500157 PMC 4958723 · doi ↗ · pubmed ↗
- 433466334623202210.3390/ijms 23063346 Jebari-Benslaiman S Galicia-García U Larrea-Sebal A Olaetxea J R Alloza I Vandenbroeck K Benito-Vicente A Martín C Int J Mol Sci Pathophysiology of Atherosclerosis 35328769 PMC 8954705 · doi ↗ · pubmed ↗
- 5188618823202210.31083/j.rcm 2306188 Díez-Villanueva P Jiménez-Méndez C Bonanad C García-Blas S Pérez-RiveraÁ Allo G García-Pardo H Formiga F Camafort M Martínez-Sellés M Ariza-SoléA Ayesta A Rev Cardiovasc Med Risk Factors and Cardiovascular Disease in the Elderly 39077174 PMC 11273864 · doi ↗ · pubmed ↗
- 6313632629200910.1089/jir.2008.0027 Deshmane S L Kremlev S Amini S Sawaya B E J Interferon Cytokine Res Monocyte Chemoattractant Protein-1 (MCP-1): An Overview 19441883 PMC 2755091 · doi ↗ · pubmed ↗
- 730479304713202110.3390/nu 13093047 Makarewicz-Wujec M Henzel J Kępka C Kruk M WardziakŁ Trochimiuk P Parzonko A Dzielińska Z Demkow M Kozłowska-Wojciechowska M Nutrients Usefulness of MCP-1 Chemokine in the Monitoring of Patients with Coronary Artery Disease Subjected to Intensive Dietary Intervention: A Pilot Study 34578925 PMC 8467171 · doi ↗ · pubmed ↗
- 8131213811200910.1007/s 11883-009-0021-y Gonzalez-Quesada C Frangogiannis N G Curr Atheroscler Rep Monocyte chemoattractant protein-1/CCL 2 as a biomarker in acute coronary syndromes 19228487 PMC 2787514 · doi ↗ · pubmed ↗