Effects of ginkgo diterpene lactone glucosamine combined with clopidogrel on hemodynamics, neurocytokines, and inflammatory responses in patients with cerebral infarction complicated by coronary heart disease
Shengjiao Zhu, Guoqiang Chen

TL;DR
Combining Ginkgo Diterpene Lactone Meglumine with Clopidogrel improves blood flow and reduces inflammation in patients with cerebral infarction and coronary heart disease.
Contribution
Demonstrates that combining GM with CLO provides better outcomes than CLO alone in patients with cerebral infarction and CHD.
Findings
The combination group showed greater improvement in hemodynamic parameters compared to CLO alone.
The combination therapy reduced inflammatory markers and improved neurological function.
No significant adverse reactions were observed in either group.
Abstract
This study investigates the effects of Ginkgo Diterpene Lactone Meglumine (GM) combined with Clopidogrel (CLO) on hemodynamics, neurocytokines, and inflammatory responses in patients with cerebral infarction (CI) complicated by coronary heart disease (CHD). A total of 152 patients diagnosed with CI complicated by CHD, admitted to our hospital between January 2024 and October 2024, were enrolled in the study. Among them, 81 patients received CLO monotherapy (control group), while the remaining 71 patients were treated with a combination of CLO and GM (observation group). Hemodynamic parameters, including plasma viscosity (PV), whole blood high (WBHSV) and low shear viscosity (WBLSV), as well as reduced viscosity (RV), were measured before and after treatment. Platelet adhesion test (PAdT) and platelet aggregation test (PAgT) were also performed. Inflammatory markers and neurocytokines…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
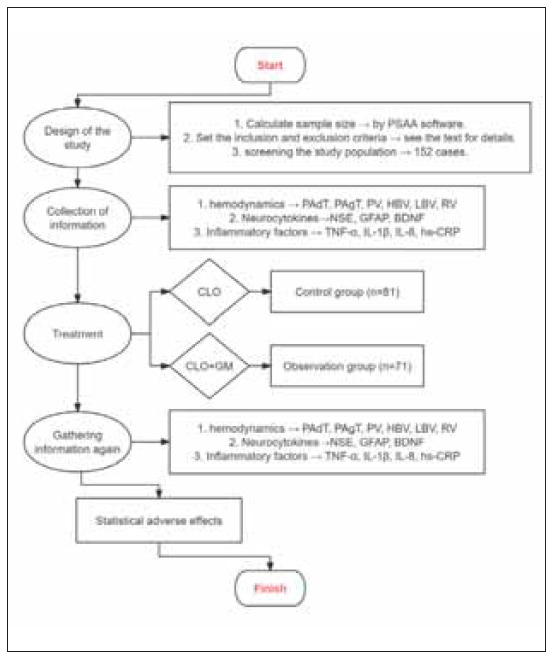 Figure 1
Figure 1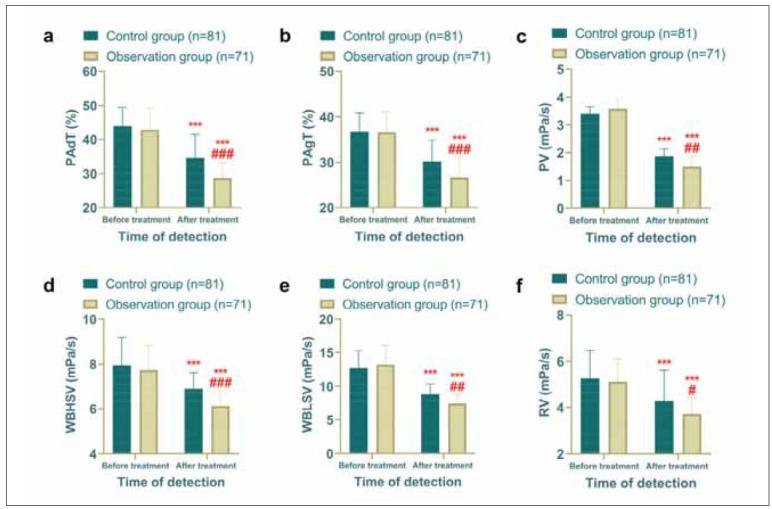 Figure 2
Figure 2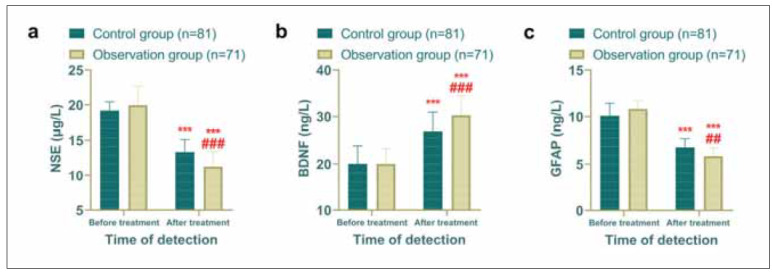 Figure 3
Figure 3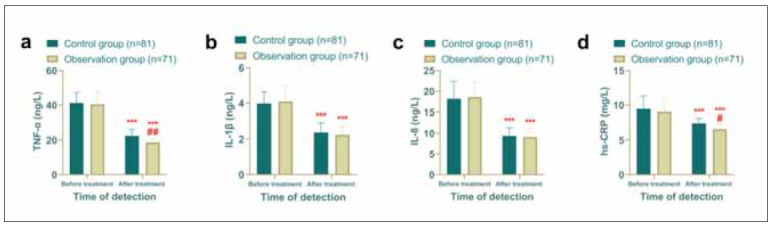 Figure 4
Figure 4| Projects | Control group<br>(n=81) | Observation group<br>(n=71) |
|
|
|---|---|---|---|---|
| Age | 66.06±3.38 | 66.65±4.09 | 0.968 | 0.335 |
| Male | 49 (60.49%) | 37 (52.11%) | 1.082 | 0.298 |
| Female | 32 (39.51%) | 34 (47.89%) | ||
| Duration of disease (h) | 16.07±2.78 | 15.82±2.82 | 0.565 | 0.573 |
| Body mass index (kg/m2) | 22.73±1.93 | 22.45±1.72 | 0.956 | 0.341 |
| Type of disease combination | 0.220 | 0.639 | ||
| CHD combined with CI | 53 (65.43%) | 49 (69.01%) | ||
| CI combined with CHD | 28 (34.57%) | 22 (30.99%) | ||
| Smoking | 42 (51.85%) | 39 (54.93%) | 0.144 | 0.704 |
| Non-smoking | 39 (48.15%) | 32 (45.07%) | ||
| Alcohol | 36 (44.44%) | 29 (40.85%) | 0.200 | 0.655 |
| Non-alcohol | 45 (55.56%) | 42 (59.15%) | ||
| Family history of CHD | 0.654 | 0.419 | ||
| yes | 7 (8.64%) | 9 (12.68%) | ||
| no | 74 (91.36%) | 62 (87.32%) | ||
| Family history of CI | 0.288 | 0.592 | ||
| yes | 5 (6.17%) | 3 (4.23%) | ||
| no | 76 (93.83%) | 68 (95.77%) | ||
| Vital signs | ||||
| Systolic blood pressure (mmHg) | 205.14±11.44 | 202.34±13.93 | 1.359 | 0.176 |
| Diastolic blood pressure (mmHg) | 116.42±8.88 | 115.62±8.82 | 0.556 | 0.579 |
| Heart rate (times/min) | 124.49±12.91 | 125.41±16.57 | 0.382 | 0.703 |
| Projects | Digestive bleeding | Bloating | Hematuria | Thrombus | Muscle pain | Electrolyte disorders | Total |
|---|---|---|---|---|---|---|---|
| Control group<br>(n=81) | 3 (3.70%) | 4 (4.94%) | 1 (1.23%) | 1 (1.23%) | 3 (3.70%) | 2 (2.47%) | 14 (17.28%) |
| Observation<br>group (n=71) | 2 (2.82%) | 3 (4.23%) | 1 (1.41%) | 0 (0.00%) | 3 (4.23%) | 1 (1.41%) | 10 (14.08%) |
|
| 0.291 | ||||||
|
| 0.589 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGinkgo biloba and Cashew Applications · Neurological Disease Mechanisms and Treatments · Neurological Disorders and Treatments
Introduction
Cardiovascular and cerebrovascular diseases remain among the leading causes of global mortality.Epidemiological data indicate that the prevalence of these diseases is approximately 724 per 100,000 individuals [1]. Notably, the associated burden has risen significantly, with the number of deaths attributed to cardiovascular diseases and cerebrovascular diseases increasing markedly from 13.406 million and 4.503 million in 1990 to 17.267 million and 9.487 million in 2010, respectively [2]. Coronary heart disease (CHD) and cerebral infarction (CI), two hallmark conditions of cardiovascular and cerebrovascular diseases, share a common pathogenesis related to atherosclerotic plaque formation, often leading to their co-occurrence [3]. Studies reveal that approximately 20–30% of CI patients also present with CHD [4]. Current clinical management strategies emphasize the protection and repair of vascular endothelial cells, plaque stabilization, and the inhibition of coagulation, oxidation, and thrombosis [5]. Among these, clopidogrel (CLO) is one of the most widely utilized therapeutic agents [6]. However, long-term CLO use is associated with limited efficacy, frequent adverse reactions, and the development of drug resistance [7]. Therefore, optimizing the treatment for patients with CI and CHD has become a critical focus in modern clinical research.
In recent years, traditional Chinese medicine (TCM) has garnered increasing attention in the management of cardiovascular and cerebrovascular diseases due to its favorable safety profile and consistent therapeutic effects. Ginkgo Diterpene Lactone Meglumine (GM), a proprietary Chinese medicine composed of the active components of Ginkgo biloba, is recognized for its ability to enhance blood circulation, re solve blood stasis, and improve meridian function [8]. In CI treatment, a meta-analysis by Li J et al. [9] de mon strated the efficacy and safety of GM. Furthermore, recent pharmacological studies by Li Y et al. [10] highlighted the cardioprotective effects of GM in cardiovascular diseases, including CHD, providing a scientific basis for its potential application in CI complicated by CHD.
Despite these promising findings, clinical evidence validating the efficacy of this combination therapy in this specific patient population remains scarce. Against this background, the aim of this study was to evaluate the therapeutic effect of GM combined with CLO in patients with CI combined with CHD, and to further investigate in depth the changes in hemodynamics, neurocytokines and inflammatory factors before and after treatment, so as to determine the clinical value of GM combined with CLO as a treatment option and to provide new insights and guidance for the treatment of this complex condition.
Materials and methods
Study subjects
This retrospective study included 152 patients diagnosed with both CI and CHD who were admitted to our hospital between January 2024 and October 2024. All patients received CLO as part of their treatment regimen. Among them, 71 patients were additionally administered GM and assigned to the observation group, while the remaining 81 patients served as the control group. All patients and data collectors were unaware of their subgroups. The study workflow is presented in Figure 1. The study protocol was approved by the Ethics Committee of our hospital (NO. HGYY-KY-2025-001) and conducted in compliance with the principles outlined in the Declaration of Helsinki. Written informed consent was obtained from all participants prior to their inclusion in the study.
Flow of this study.
Inclusion and exclusion criteria
Inclusion criteria: (1) Diagnosis of CHD [11] and CI [12] confirmed by clinical examination. (2) Age 60 years. (3) Presentation beyond the thrombolytic therapy time window (4.5h). (4) Normal cognitive function.
Exclusion criteria: (1) Presence of autoimmune diseases. (2) Coagulation disorders. (3) Impaired function of other major organs. (4) Diagnosis of malignant tumors. (5) Comorbid conditions such asmyocarditis, rheumatic heart disease, or cardiomyopathy. (6) History of brain surgery. (7) Known allergy to any of the medications used in this study.
Treatment protocol
Upon admission, all patients were treated with CLO (CSPC Pharmaceutical Group Limited, Ou Yi Pharmaceutical Co., Ltd., H20193160), administered as one tablet once daily for 14 consecutive days. In addition, the patients were given oral aspirin (Shenyang Aojina Pharmaceutical Co., Ltd, H20065051), 100 mg/d, 1 time/d. Patients in the observation group additionally received GM (Jiangsu MyKanion Biological Medicine Co., Ltd., Z20120024) via intravenous infusion. GM was administered at a dose of 5 mL, diluted in 250 mL of 0.9% sodium chloride injection, once daily. The initial infusion rate was set at 15 drops per minute, and if no significant adverse reactions were observed within 30 minutes, the rate was increased to 40 drops per minute. The treatment duration was also 14 consecutive days.
Laboratory assessments
Fasting venous blood was collected from patients before and after treatment and divided into 2 portions. Blood rheology parameters, including plasma viscosity (PV), whole blood high shear viscosity (WBHSV), whole blood low shear viscosity (WBLSV), and reduced viscosity (RV), were measured using a blood rheology analyzer (HT-100A, Zibo Hengtuo Analytical Instrument Co., Ltd.). Platelet adhesion test (PAdT) and platelet aggregation test (PAgT) were also conducted. Additionally, serum levels of tumor necrosis factor-α (TNF-α), interleukin-1β (IL-1β), interleukin-8 (IL-8), hypersensitive C-reactive protein (hs-CRP), neuron-specific enolase (NSE), glial fibrillary acidic protein (GFAP), and brain-derived neurotrophic factor (BDNF) were quantified using enzyme-linked immunosorbent assays (ELISA). The kits were purchased from Wuhan Fion Bio-technology Co. Ltd, and the operation process was carried out in strict accordance with the instructions of the kits.
Outcome measures
The primary outcomes included changes in hemodynamic parameters (PV, WBHSV, WBLSV, RV, PAdT, and PAgT), neurocytokine levels (NSE, GFAP, and BDNF), and inflammatory markers (TNF-α, IL-1β, IL-8, and hs-CRP) before and after treatment in both groups. Secondary outcomes included the incidence of adverse reactions during the treatment period.
Statistical analysis
Data analysis was performed using SPSS 26.0 software. Categorical variables, expressed as percentages (%), were compared using the chi-square test. For continuous variables, the Shapiro-Wilk test was used to assess data distribution. Normally distributed data, presented as mean ± standard deviation, were analyzed using independent t-tests for between-group comparisons and paired t-tests for within-group comparisons. Non-normally distributed data, expressed as median (interquartile range), were analyzed using the Mann-Whitney U test for between-group comparisons and the Wilcoxon signed-rank test for within-group comparisons. For the simultaneous analysis of multiple indicators, the Benjamini-Hochberg (BH) method was used to control for the false discovery rate (FDR) and to calculate corrected q-values. A P-value<0.05 was considered statistically significant.
Results
Baseline characteristics were comparable between groups
A comparison of baseline characteristics, including age, gender, and disease duration, revealed no statistically significant differences between the observation group and the control group (P>0.05, Table 1). This confirmed that the two groups were well-matched and suitable for comparative analysis.
Hemodynamic improvements were more pronounced in the observation group
Given that both CI and CHD are rooted in vascular obstruction caused by atherosclerosis [13], hemo dynamic parameters were the primary focus of this study. Post-treatment comparisons showed significant reductions in PAdT, PAgT, PV, WBHSV, WBLSV, and RV in both groups compared to the pre-treatment levels (P<0.05). Importantly, the observation group exhibited greater reductions in PAdT, PAgT, WBLSV, and RV than the control group (P<0.05), suggesting that the addition of GM to CLO therapy led to more substantial hemodynamic improvements (Figure 2).
*Comparison of hemodynamics, observation group had better hemodynamics after treatment. (a) Comparison of PAdT before and after treatment. (b) Comparison of PAgT before and after treatment. (c) Comparison of PV before and after treatment. (d) Comparison of WBHSV before and after treatment. (e) Comparison of WBLSV before and after treatment. (f) Comparison of RV before and after treatment. Comparison with before treatment **P<0.001, comparison with control group #P<0.05, ##P<0.01, ###P<0.001.
Neurological function showed greater improvement in the observation group
To evaluate neurological function, neurocytokine levels were measured in both groups. Similarly,there was no difference in the comparison of NSE, GFAP and BDNF before treatment between the two groups (p>0.05). Post-treatment results indicated that levels of NSE and GFAP decreased significantly in both groups, with the observation group demonstrating lower levels than the control group (P<0.05). Conversely, BDNF levels increased in both groups, with the observation group showing a more pronounced elevation compared to the control group (P<0.05). These findings suggest enhanced neurological recovery in the observation group (Figure 3).
*Comparison of neurocytokine, observation group had better hemodynamics after treatment. (a) Comparison of NSE before and after treatment. (b) Comparison of BDNF before and after treatment. (c) Comparison of GFAP before and after treatment. Comparison with before treatment **P<0.001, comparison with control group ##P<0.01, ###P<0.001.
Inflammatory response was more effectively suppressed in the observation group
Inflammatory markers were also assessed to evaluate the systemic inflammatory response. Post-treatment levels of TNF-α, IL-1β, IL-8, and hs-CRP were significantly reduced in both groups compared to pre-treatment levels (P<0.05). While no significant differences were observed in IL-1β and IL-8 levels between the two groups (P>0.05), the observation group exhibited significantly lower levels of TNF-α and hs-CRP than the control group (P<0.05), indicating a more robust anti-inflammatory effect in the observation group (Figure 4).
*Comparison of inflammatory factors, observation group had better hemodynamics after treatment. (a) Comparison of TNF-α before and after treatment. (b) Comparison of IL-1β before and after treatment. (c) Comparison of IL-8 before and after treatment. (d) Comparison of IL-8 before and after treatment. Comparison with before treatment **P<0.001, comparison with control group #P<0.05, ##P<0.01.
There was no difference in the incidence of adverse reactions between the two groups
Finally, the safety of the treatment regimens was assessed by comparing the incidence of adverse reactions. No significant differences were observed between the observation group and the control group (P>0.05), indicating comparable safety profiles (Table 2).
Discussion
This study demonstrated that the combination of GM and CLO significantly enhanced hemodynamic parameters and neurological function while effectively alleviating inflammatory responses in patients with CI complicated by CHD. These results underscore the clinical efficacy of this combined treatment regimen and offer valuable insights for optimizing the management of CI combined with CHD in the future.
As highlighted earlier, hemodynamic stability is a critical factor in the progression of both CI and CHD. The disruption of cerebral blood flow leading to localized ischemic necrosis of brain tissue, as well as coronary artery stenosis or occlusion causing myocardial ischemia, are the fundamental pathological mechanisms underlying these conditions [14]. In this study, both treatment groups exhibited significant improvements in hemodynamic parameters following the treatment, reaffirming the feasibility of both therapeutic strategies for managing CI complicated by CHD. The efficacy of CLO, a cornerstone in the clinical management of CI, has been extensively validated in prior research [15] [16]. Therefore, the observed improvements in hemodynamics in both groups were consistent with expectations. However, although no significant inter-group differences were observed in post-treatment PV and WBHSV, the observation group demonstrated further reductions in PAdT, PAgT, WBLSV, and RV. These findings suggest that the combination of GM and CLO has a more pronounced effect on improving hemodynamics in patients. In an animal study investigating lung injury and pulmonary fibrosis, Li GP et al. [17] found that ginkgolides, the primary active components of GM, exert antiplatelet aggregation effects by antagonizing the PI3K/AKT signaling pathway, thereby inhibiting thrombus formation. Based on this evidence, we propose that the combination of GM and CLO may have a synergistic effect in patients with CI and CHD, significantly enhancing cerebral blood flow and mitigating brain damage. These results align with the findings of Chen R et al. [18], who analyzed the efficacy of GM in treating CI, further corroborating our conclusions.
To further evaluate the therapeutic efficacy of GM combined with CLO in patients with CI complicated by CHD, we assessed neurocytokine levels in both groups. Neurocytokines are known to directly influence neuronal plasticity by interacting with neurons that express cytokine receptors [19]. In this study, we focused on three key neurocytokines: NSE, BDNF, and GFAP. BDNF plays a pivotal role in neuronal regeneration and the regulation of synaptic plasticity [20]. GFAP, a structural protein in the cytoskeleton, helps maintain cellular tension, and its levels rise in response to neural injury [21]. NSE, a critical enzyme in the glycolytic pathway, is elevated following braintissue damage [22]. In this study, post-treatment results showed that the observation group had lower levels of NSE and GFAP but higher levels of BDNF compared to the control group, confirming the significant neurorestorative effects of GM combined with CLO. Supporting this, Fan XX et al. [23] demonstrated in an in vitro study that ginkgolide B, a primary active component of GM, exerts profound neuroprotective effects by scavenging free radicals and mitigating oxidative stress. Furthermore, research by Chen A et al. [24] demonstrated the beneficial effects of ginkgolides on neuronal activity and functional recovery, further corroborating our findings.
Furthermore, previous evidence has confirmed the anti-inflammatory properties of ginkgolides in patients with inflammatory conditions such as Alzheimer’s disease [25]. Liu Q et al. [26] also high-lighted that the neuroprotective mechanisms of Ginkgo biloba are largely mediated through its anti-inflammatory effects. Consistent with these findings, our study measured inflammatory cytokine levels in both groups and found that post-treatment levels of TNF-α and hs-CRP were significantly lower in the observation group compared to the control group. This further supports the superior anti-inflammatory efficacy of GM combined with CLO in patients with CI and CHD. The therapeutic mechanism is likely attributed to the γ-lactone ring structure of ginkgolides, which confers a wide range of pharmacological activities, including anti-hepatotoxicity, immune stimulation, and inhibition of angiotensin release. Additionally, ginkgolides modulate the production of pro-angiogenic and anti-angiogenic factors while downregulating inflammatory cytokine levels [27]. These mechanisms are highly beneficial in alleviating the pathological progression of both CI and CHD.
Finally, the absence of significant differences in adverse reaction rates between the two groups reaf-firms the favorable safety profile of GM. As a TCM, GM has consistently demonstrated excellent safety in prior clinical studies [28] [29], further supporting its potential for combined use with CLO in future clinical applications.
Nevertheless, it is essential to address several limitations in this study. For example, the relativelysmall sample size may limit the representativeness and comprehensiveness of the findings. Furthermore, the short study duration precludes an assessment of the long-term prognostic impact of GM combined with CLO in patients with CI and CHD. Future research should aim to include larger patient cohorts, extend the follow-up period, and incorporate additional objective measures to provide a more comprehensive understanding of the therapeutic efficacy and mechanisms of GM combined with CLO.
Conclusion
The combination of GM and CLO demonstrates significant efficacy in improving hemodynamic parameters, enhancing neuroprotective effects, and mitigating inflammatory responses in patients with CI complicated by CHD, while maintaining an excellent safety profile. This regimen represents a promising therapeutic option for the management of CI combined with CHD.
Dodatak
Availability of data and materials
The data used to support the findings of this study are available from the corresponding author upon request.
Funding
No funding was received for conducting this study.
Acknowledgements
Not applicable.
Conflict of interest statement
All the authors declare that they have no conflict of interest in this work.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1e 0107447 e 0107448201910.1161/jaha.118.010744 Iyer D G Shah N S Hastings K G Hu J Rodriguez F Boothroyd D B Krishnan A V Falasinnu T Palaniappan L J Am Heart Assoc Years of Potential Life Lost Because of Cardiovascular Disease in Asian-American Subgroups, 2003-201230890022 PMC 6509739 · doi ↗ · pubmed ↗
- 2315420492015 Liu J Liu Y Wang L Yin P Liu S You J et al Zhonghua Yu Fang Yi Xue Za Zhi The disease burden of cardiovascular and circulatory diseases in China, 1990 and 201026081539 · pubmed ↗
- 3e 2092048 e 2092041022024 Zhou Z You S Sakamoto Y Xu Y Ding S Xu W et al Neurology Covert Cerebrovascular Changes in People With Heart Disease: A Systematic Review and Meta-Analysis 3853101010.1212/WNL.0000000000209204 · doi ↗ · pubmed ↗
- 41010821110108247202210.1016/j.cpcardiol.2021.101082 Shamaki G R Markson F Soji-Ayoade D Agwuegbo C C Bamgbose M O Tamunoinemi B Curr Probl Cardiol Peripheral Artery Disease: A Comprehensive Updated Review 34906615 · doi ↗ · pubmed ↗
- 51409653140965315202410.3389/fendo.2024.1409653 Xu D Xie L Cheng C Xue F Sun C Front Endocrinol (Lausanne)Triglyceride-rich lipoproteins and cardiovascular diseases 38883601 PMC 11176465 · doi ↗ · pubmed ↗
- 652363192024 Li Y Li J Wang B Jing Q Zeng Y Hou A et al JAMA Cardiol Extended Clopidogrel Monotherapy vs DAPT in Patients With Acute Coronary Syndromes at High Ischemic and Bleeding Risk: The OPT-BIRISK Randomized Clinical Trial 3863048910.1001/jamacardio.2024.0534 PMC 11024736 · doi ↗ · pubmed ↗
- 7190125619012562022202210.1155/2022/1901256 Chang R Zhou W Ye Y Zhang X Liu Y Wu J Genet Res (Camb)Relationship between CYP 2C 19 Polymorphism and Clopidogrel Resistance in Patients with Coronary Heart Disease and Ischemic Stroke in China 36325266 PMC 9616677 · doi ↗ · pubmed ↗
- 8e 23288288 e 232882862023 Zhang Q Wang A Xu Q Xia X Tian X Zhang Y et al JAMA Netw Open Efficacy and Safety of Ginkgo Diterpene Lactone Meglumine in Acute Ischemic Stroke: A Randomized Clinical Trial 3757879110.1001/jamanetworkopen.2023.28828 PMC 10425831 · doi ↗ · pubmed ↗