Parathyroidectomy and Cardiometabolic Risks in Patients With Primary Hyperparathyroidism
Nir Tsur, Nofar Edri, Tomer Kerman, Yeela Talmor-Barkan, Shir Kushnir, Gideon Bachar

TL;DR
This study finds that primary hyperparathyroidism increases cardiometabolic risks, and surgery may lower the risk of type 2 diabetes.
Contribution
The study shows parathyroidectomy is linked to reduced type 2 diabetes risk in pHPT patients, a novel surgical benefit.
Findings
Patients with pHPT had higher long-term risks of hypertension, type 2 diabetes, cardiovascular disease, and cerebrovascular accidents.
Parathyroidectomy was associated with a 44% lower risk of type 2 diabetes compared to nonsurgical treatment.
No significant differences were observed in other cardiometabolic outcomes following parathyroidectomy.
Abstract
Is primary hyperparathyroidism (pHPT) associated with increased cardiometabolic risks, and might parathyroidectomy help reduce these risks? In this cohort study including 50 199 patients with pHPT and 150 265 matched controls, pHPT was associated with significantly increased incidence of hypertension, type 2 diabetes, cardiovascular disease, and cerebrovascular accident. Among 6654 patients with pHPT who underwent parathyroidectomy, the incidence of type 2 diabetes was significantly lower compared with those receiving nonsurgical treatment; no differences were found for other types of cardiometabolic risk. These findings suggest that parathyroidectomy may be associated with reduced risk of type 2 diabetes in patients with pHPT. This cohort study assesses the prevalence and severity of cardiovascular complications in patients with primary hyperparathyroidism and examines whether…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure
Figure| Characteristic | Control group (n = 150 265) | pHPT group (n = 50 199) | SMD |
|---|---|---|---|
| Age, y | |||
| Mean (SD) | 64 (14) | 64 (14) | 0 |
| Median (IQR) | 66 (55-75) | 66 (55-75) | |
| Range | 18-104 | 18-104 | |
| Sex, No./total No. (%) | |||
| Female | 102 591/150 265 (68.3) | 34 293/50 199 (68.3) | 0 |
| Male | 47 674/150 265 (31.7) | 15 906/50 199 (31.7) | |
| Ethnicity, No./total No. (%) | |||
| Jewish | 124 133/141 180 (87.9) | 42 300/46 945 (90.1) | 0.07 |
| Arab | 17 047/141 180 (12.1) | 4645/46 945 (9.9) | |
| SES, No./total No. (%) | |||
| Low | 19 620/143 069 (13.7) | 6556/47 791 (13.7) | 0 |
| Medium | 90 758/143 069 (63.4) | 30 279/47 791 (63.4) | |
| High | 32 691/143 069 (22.8) | 10 956/47 791 (22.9) | |
| CCI, No./total No. (%) | |||
| 0 | 18 753/150 241 (12.5) | 4621/50 189 (9.2) | 0.17 |
| 1-2 | 47 556/150 241 (31.7) | 13 486/50 189 (26.9) | |
| ≥ 3 | 83 932/150 241 (55.9) | 32 082/50 189 (63.9) | |
| Background diagnoses, No./total No. (%) | |||
| Hypertension | 67 229/150 265 (44.7) | 29 463/46 945 (58.7) | 0.28 |
| T2D | 17 927/150 265 (11.9) | 9047/46 945 (18.0) | 0.17 |
| CVD | 25 240150 265 (16.8) | 11 954/46 945 (23.8) | 0.18 |
| CVA | 12 321150 265 (8.2) | 565146 945 (11.3) | 0.10 |
| Smoking, No./total No. (%) | 15 899/97 154 (16.4) | 4745/32 868 (14.4) | 0.05 |
| BMI | |||
| Total No. of participants | 109 782 | 38 337 | NA |
| Mean (SD) | 28 (5.7) | 28.8 (6.1) | 0.13 |
| Median (IQR) | 27.3 (24.2-30.9) | 27.9 (24.6-31.9) | |
| Range | 10.2-64.9 | 11.6-65.0 | |
| Calcium level, mg/dL | |||
| Total No. of participants | 144 207 | 49 702 | NA |
| Mean (SD) | 9.3 (0.4) | 9.8 (1.0) | 0.66 |
| Median (IQR) | 9.3 (9.0-9.5) | 9.7 (9.1-10.4) | |
| Range | 3.0-17.5 | 3.7-21.2 | |
| Phosphorus level, mg/dL | |||
| Total No. of participants | 143 852 | 49 794 | NA |
| Mean (SD) | 3.6 (0.6) | 3.4 (0.9) | 0.16 |
| Median (IQR) | 3.6 (3.2-3.9) | 3.3 (2.9-3.8) | |
| Range | 0.8-13.2 | 0.4-16.8 | |
| PTH level, pg/mL | |||
| Total No. of participants | 32 702 | 46 247 | NA |
| Mean (SD) | 57.8 (73.6) | 144.5 (189.8) | 0.60 |
| Median (IQR) | 41.9 (28.7-64.4) | 98.0 (64.3-149.0) | |
| Range | 0-2379.0 | 0-2487.0 | |
| Urine calcium level, mg/24 h | |||
| Total No. of participants | 21 524 | 33 562 | NA |
| Mean (SD) | 126.6 (100.6) | 172.8 (157.1) | 0.35 |
| Median (IQR) | 109.0 (56.0-175.5) | 136.0 (51.0-256.0) | |
| Range | 0-2473.0 | 0-2238/6 |
| Characteristic | Control group (n = 150 265) | pHPT group (n = 50 199) | |
|---|---|---|---|
| Time at risk, y | |||
| Mean (SD) | 8.3 (5.4) | 6.8 (5.3) | NA |
| Median (IQR) | 8 (3.1-14.5) | 5.5 (1.8-11.9) | NA |
| Range | 0-15 | 0-15 | NA |
|
| |||
| No. of participants | 83 036 | 20 736 | NA |
| No. of events, No. (%) | 25 860 (31.1) | 6438 (31.0) | NA |
| Incidence per 1000 person-years (95% CI) | 44.56 (44.02-45.11) | 55.3 (53.97-56.67) | NA |
| Unadjusted HR (95% CI) | 1 [Reference] | 1.36 (1.34-1.47) | <.001 |
| Adjusted HR (95% CI) | 1 [Reference] | 1.22 (1.17-1.33) | <.001 |
|
| |||
| No. of participants | 132 338 | 41 152 | NA |
| No. of events, No. (%) | 13 657 (10.3) | 4661 (11.3) | NA |
| Incidence per 1000 person-years (95% CI) | 12.81 (12.60-13.03) | 16.99 (16.51-17.49) | NA |
| Unadjusted HR (95% CI) | 1 [Reference] | 1.33 (1.31-1.45) | <.001 |
| Adjusted HR (95% CI) | 1 [Reference] | 1.07 (1.01-1.16) | .02 |
|
| |||
| No. of participants | 125 025 | 38 245 | NA |
| No. of events, No. (%) | 11 622 (9.3) | 4061 (10.6) | NA |
| Incidence per 1000 person-years (95% CI) | 11.47 (11.26-11.68) | 16.09 (15.60-16.59) | NA |
| Unadjusted HR (95% CI) | 1 [Reference] | 1.43 (1.41-1.57) | <.001 |
| Adjusted HR (95% CI) | 1 [Reference] | 1.28 (1.21-1.40) | <.001 |
|
| |||
| No. of participants | 137 944 | 44 548 | NA |
| No. of events, No. (%) | 15 670 (11.4) | 5625 (12.6) | NA |
| Incidence per 1000 person-years (95% CI) | 14.10 (13.88-14.32) | 19.35 (18.85-19.87) | NA |
| Unadjusted HR (95% CI) | 1 [Reference] | 1.36 (1.34-1.47) | <.001 |
| Adjusted HR (95% CI) | 1 [Reference] | 1.22 (1.17-1.33) | <.001 |
| Characteristic | Nonsurgical treatment (n = 19 962) | Parathyroidectomy (n = 6654) | SMD |
|---|---|---|---|
| Age, y | |||
| Mean (SD) | 58 (12) | 58 (12) | 0 |
| Median (IQR) | 59 (51-67) | 59 (51-67) | |
| Range | 18-94 | 19-94 | |
| Sex, No./total No. (%) | |||
| Female | 14 403/19 962 (72.2) | 4801/6654 (72.2) | 0 |
| Male | 5559/19 962 (27.8) | 1853/6654 (27.8) | |
| Ethnicity, No./total No. (%) | |||
| Jewish | 2105/19 140 (11.0) | 626/6371 (9.8) | 0.04 |
| Arab | 17 035/19 140 (89.0) | 5745/6371 (90.2) | |
| SES, No./total No. (%) | |||
| Low | 2331/19 023 (12.3) | 731/6341 (11.5) | 0.02 |
| Medium | 12 506/19 023 (65.7) | 4192/6341 (66.1) | |
| High | 4186/19 023 (22.0) | 1418/6341 (22.4) | |
| CCI, No./total No. (%) | |||
| 0 | 2574/19 955 (12.9) | 985/6653 (14.8) | 0.17 |
| 1-2 | 7524/19 995 (37.7) | 2955/6653 (44.4) | |
| ≥ 3 | 9857/19 995 (49.4) | 2713/6653 (40.8) | |
| Background diagnoses, No./total No. (%) | |||
| Hypertension | 9944/19 962 (49.8) | 2820/6654 (42.4) | 0.15 |
| T2D | 2919/19 962 (14.6) | 638/6654 (9.6) | 0.15 |
| CVD | 3385/19 962 (17.0) | 826/6654 (12.4) | 0.13 |
| CVA | 1634/19 962 (8.2) | 285/6654 (4.2) | 0.15 |
| Smoking, No./total No. (%) | 2146/13 785 (15.6) | 701/3824 (18.3) | 0.07 |
| BMI | |||
| Total No. of participants | 15 329 | 4173 | NA |
| Mean (SD) | 29.0 (6.4) | 28.4 (5.7) | 0.11 |
| Median (IQR) | 28.0 (24.5-32.4) | 27.6 (24.6-31.5) | |
| Range | 13.3-65.0 | 14.9-64.9 | |
| Calcium level, mg/dL | |||
| Total No. of participants | 19 784 | 6596 | NA |
| Mean (SD) | 9.62 (0.93) | 10.52 (1.00) | 0.93 |
| Median (IQR) | 9.53 (9.05-10.26) | 10.54 (10.04-11.02) | |
| Range | 3.74-19.41 | 3.74-21.16 | |
| Phosphorus level, mg/dL | |||
| Total No. of participants | 19 794 | 6617 | NA |
| Mean (SD) | 3.53 (0.93) | 3.05 (0.86) | 0.54 |
| Median (IQR) | 3.40 (2.97-3.90) | 2.90 (2.53-3.32) | |
| Range | 0.71-14.29 | 0.90-12.89 | |
| PTH level, pg/mL | |||
| Total No. of participants | 18 469 | 6241 | NA |
| Mean (SD) | 136 (181) | 155 (211) | 0.10 |
| Median (IQR) | 94 (62-137) | 106 (65-168) | |
| Range | 0-2464 | 0-2487 | |
| Urine calcium level, mg/24 h | |||
| Total No. of participants | 13 236 | 5789 | NA |
| Mean (SD) | 170 (154) | 266 (183) | 0.57 |
| Median (IQR) | 137 (53-248) | 252 (128-378) | |
| Range | 0-2239 | 0-2141 |
| Characteristic | Nonsurgical treatment | Parathyroidectomy | |
|---|---|---|---|
| Time at risk, y | |||
| Mean (SD) | 6.9 (5.6) | 9.1 (5.1) | NA |
| Median (IQR) | 5.7 (1.5-12.8) | 9.8 (4.4-15) | NA |
| Range | 0-15 | 0-15 | NA |
|
| |||
| Incidence per 1000 person-years (95% CI) | 48.85 (47.32-50.43) | 45.89 (42.99-49.00) | NA |
| Unadjusted HR (95% CI) | 1 [Reference] | 1.12 (0.94-1.35) | .07 |
| Adjusted HR (95% CI) | 1 [Reference] | 1.19 (0.69-1.96) | .33 |
|
| |||
| Incidence per 1000 person-years (95% CI) | 15.18 (14.58-15.81) | 10.77 (9.8011.83) | NA |
| Unadjusted HR (95% CI) | 1 [Reference] | 0.80 (0.65-0.93) | .001 |
| Adjusted HR (95% CI) | 1 [Reference] | 0.56 (0.30-0.89) | .002 |
|
| |||
| Incidence per 1000 person-years (95% CI) | 12.49 (11.94-13.07) | 11.57 (10.57-12.66) | NA |
| Unadjusted HR (95% CI) | 1 [Reference] | 0.95 (0.78-1.13) | .42 |
| Adjusted HR (95% CI) | 1 [Reference] | 0.93 (0.85-1.02) | .92 |
|
| |||
| Incidence per 1000 person-years (95% CI) | 14.12 (13.55-14.70) | 12.93 (11.92-14.03) | NA |
| Unadjusted HR (95% CI) | 1 [Reference] | 0.81 (0.67-0.91) | <.001 |
| Adjusted HR (95% CI) | 1 [Reference] | 0.79 (0.50-1.13) | .09 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParathyroid Disorders and Treatments · Thyroid and Parathyroid Surgery · Vitamin D Research Studies
Introduction
Primary hyperparathyroidism (pHPT) is the third most common endocrine disorder worldwide, characterized by the overproduction of parathyroid hormone (PTH), which often leads to hypercalcemia and a range of systemic complications.^1,2,3^ Among the most serious complications are the cardiovascular risks associated with pHPT, including hypertension,^4^ arrhythmias, and vascular calcification, which impair patient well-being and quality of life. Although several studies have demonstrated the prevalence of these complications, the extent, underlying mechanisms, and long-term outcomes remain underexplored.^3,5,6,7,8,9^ There is ongoing debate regarding the clinical importance of these cardiovascular outcomes and the necessity of routine cardiovascular assessment in patients with pHPT.^10,11^
Parathyroidectomy effectively normalizes PTH and calcium levels, correcting metabolic abnormalities.^12^ However, its impact on long-term cardiovascular risks remains uncertain.^13,14,15,16^ While early intervention is thought to reduce these risks, its effectiveness varies substantially depending on patient demographics, disease severity, and clinical presentation.^16,17,18^ Some studies suggest cardiovascular risks in patients with pHPT can persist or only partially improve after achieving postsurgical normocalcemia.^18,19,20^ These variations highlight the complexity of pHPT as a systemic disease and underscore the need for a deeper understanding of the implications of excess PTH levels concerning cardiovascular morbidity.
This study aims to assess the prevalence and severity of cardiovascular complications in patients with pHPT. Additionally, we examine the association of parathyroidectomy with these cardiovascular risks and metabolic outcomes.
Methods
Study Design and Population
This population-based cohort study was conducted at Rabin Medical Center, a university-affiliated hospital run by Clalit Health Service (CHS), the largest of 4 state-mandated health management organizations in Israel with approximately 4.4 million members. The CHS database includes information on diagnoses, hospitalizations, clinic visits, demographic characteristics of patients, laboratory values, and medications. Members’ low turnover (approximately 1%) enables accurate long-term follow-up. The study was conducted in accordance with the Declaration of Helsinki^21^ and was approved by the Ethics Committee of Rabin Medical Center, which waived the need for informed consent due to the retrospective nature of the study and the use of deidentified data. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
The study cohort consisted of patients 18 years or older registered with CHS between January 1, 2000, and November 29, 2023. The study group included patients with pHPT, defined by elevated PTH levels, excluding secondary causes such as chronic kidney disease, vitamin D deficiency, or malabsorption. The control group included individuals without pHPT, matched in a 1:3 ratio by birth year, sex, and socioeconomic status (SES).
Variables and Data Collection
Data on cardiovascular-related conditions were extracted, specifically the first recorded diagnoses of hypertension, type 2 diabetes (T2D), cardiovascular diseases (CVD; including ischemic heart disease, acute myocardial infarction, and heart failure), and cerebrovascular accidents (CVA; including cerebral infarction). Additional demographic, clinical, and laboratory data, including age, sex, ethnicity, SES (low, medium, or high), smoking status, body mass index (BMI), and laboratory results, were also extracted. The Charlson Comorbidity Index (CCI) was calculated for each patient to assess the burden of comorbid conditions. SES was classified according to the Israeli Central Bureau of Statistics methodology.^22^ Ethnicity was assessed based on national registry data and reported using standard categories (Jewish or Arab); these data were collected to account for potential confounding by ethnicity, as Jewish and Arab populations in Israel represent 2 distinct groups that have been shown to differ in demographic and clinical characteristics.^23^ Sex was reported as male or female (no other categories were recorded). Patients with missing baseline data or lost to follow-up were excluded from each relevant analysis. All data were obtained through the CHS data-sharing platform powered by MDClone.^24^
Outcome Definitions
Incident cases of hypertension, T2D, CVD (ischemic heart disease, myocardial infarction, and heart failure), and CVA were identified using International Classification of Disease, Ninth Revision (ICD-9), diagnostic codes registered in the CHS database. For T2D, ascertainment required a new ICD-9 diagnosis code in patients without a prior T2D diagnosis, without prior use of antidiabetic medication, and with normal hemoglobin A_1c_ levels (<6.5%) prior to the index date. CVD and CVA outcomes were defined based on validated ICD-9 coding algorithms that were previously applied in CHS research.^25^ Only first incident events were considered, and patients with preexisting diagnoses of the respective outcome were excluded from each outcome-specific analysis.
Statistical Analysis
Data were analyzed from November 1, 2024, to April 1, 2025. All statistical tests were 2 tailed, and P < .05 was considered statistically significant. Data were analyzed using R software, version.3.6.1 (R Program for Statistical Computing).
Patients With pHPT vs Matched Controls
Continuous variables were summarized using means and SDs and medians and IQRs, while frequencies and percentages represented categorical variables. Standardized mean differences (SMDs) were calculated for all baseline covariates, with values less than 0.10 indicating good balance between groups.
The incidence rates of cardiovascular-related conditions (hypertension, T2D, CVD, and CVA) were compared between the 2 groups. Each condition was analyzed separately, and individuals with a prior diagnosis of that specific condition were excluded from the analysis of that outcome. This approach ensured that only first incident events were assessed, thereby preventing distortion of the results by individuals at higher baseline risk of recurrence and preserving comparability between groups.
For the study group, follow-up began at the time of pHPT diagnosis, while for the control group, follow-up began at the diagnosis date of the matched case. Follow-up was censored at death, parathyroidectomy, the end of the study period (November 29, 2023), or after 15 years of follow-up. Incident rates per 1000 person-years and 95% CIs were calculated to account for varying follow-up durations. Cumulative incidence was estimated using the 1-minus Kaplan-Meier method, and differences between the survival curves were assessed using the log-rank test. Stratified Cox proportional hazards regression models were applied for each condition with stratification by the matching factors (birth year, sex, and SES) to account for the matched study design. The models were further adjusted for CCI, ethnicity, and BMI. The proportional hazards assumption was evaluated using Schoenfeld residuals and graphical diagnostics, with no major violations observed. Robust CIs were obtained using nonparametric bootstrapping (1000 replications) to ensure stable variance estimation.
Parathyroidectomy vs Nonsurgical Management
Patients with pHPT who underwent parathyroidectomy were compared with those who received nonsurgical treatment. Each parathyroidectomy case was matched in a 1:3 ratio to controls by age at diagnosis, sex, and SES. Consistent with the approach used in the patient vs control analysis, each cardiovascular condition was analyzed separately, excluding individuals with a prior diagnosis of the respective condition. Time-dependent stratified Cox proportional hazards regression models were then applied, with parathyroidectomy status included as a time-varying covariate and stratification by the matched sets. The models were further adjusted for CCI, ethnicity, BMI, corrected calcium level, and PTH. Robust CIs were derived using nonparametric bootstrapping with 1000 replications to ensure stable variance estimation.
Results
Status at Diagnosis
A total of 200 464 individuals were included in the study (median age, 66 [IQR, 55-75] years; 136 884 [68.3%] female and 63 580 [31.7%] male): 50 199 patients in the pHPT group and 150 265 matched controls. Both groups were well-matched for age, sex, and SES. The CCI showed more pronounced comorbidities in the pHPT group: 32 082 of 50 189 (63.9%) had a comorbidity score of 3 or greater compared with 83 932 of 150 241 (55.9%) in the control group (eFigure in Supplement 1). Notably, being in the pHPT group was associated with higher rates of preexisting hypertension (29 463 [58.7%] vs 67 229 [44.7%]), T2D (9047 [18.0%] vs 17 927 [11.9%]), CVD (11 954 [23.8%] vs 25240 [16.8%]), and CVA (5651 [11.3%] vs 12 321 [8.2%]). These values describe the entire cohort at baseline. In the outcome-specific analyses, patients with a prior diagnosis of the respective condition were excluded. Further baseline characteristics and metabolic values are presented in Table 1.
Status During Follow-Up
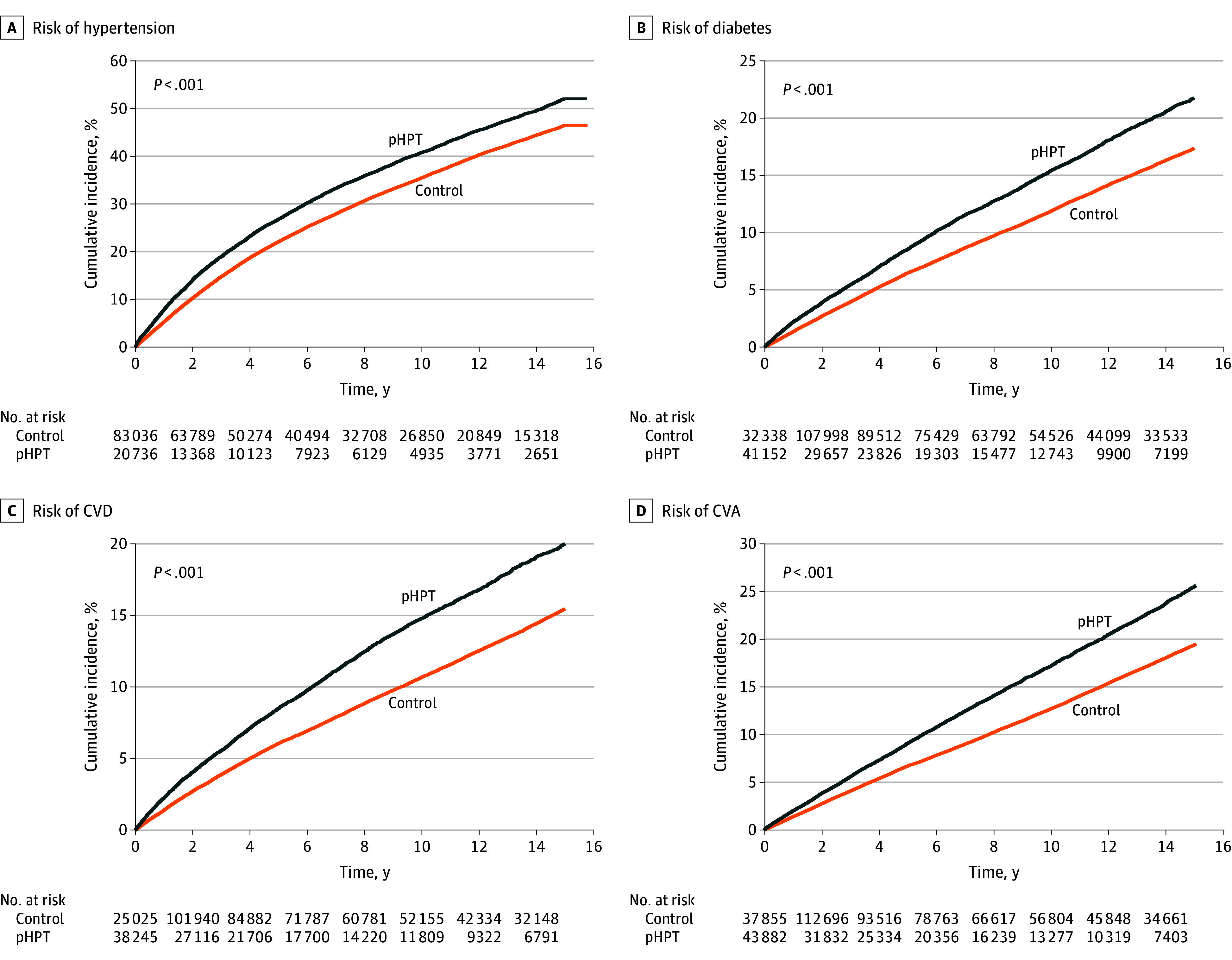
Table 2 provides an overview of cardiovascular-related outcomes in patients with pHPT compared with matched controls. During the follow-up period, incidence rates per 1000 person-years were significantly higher in the pHPT group across all outcomes: hypertension (55.3 [95% CI, 53.97-56.67] vs 44.56 [95% CI, 44.02-45.11]), T2D (16.99 [95% CI, 16.51-17.49] vs 12.81 [95% CI, 12.60-13.03]), CVD (16.09 [95% CI, 15.60-16.59] vs 11.47 [95% CI, 11.26-11.68]), and CVA (19.35 [95% CI, 18.85-19.87] vs 14.10 [95% CI, 13.88-14.32]). Adjusted hazard ratios (AHRs) confirmed the elevated risk in the pHPT group for hypertension (1.22; 95% CI, 1.17-1.33]), T2D (1.07; 95% CI, 1.01-1.16), CVD (1.28; 95% CI, 1.21-1.42), and CVA (1.22; 95% CI, 1.17-1.33). The Figure shows the cumulative incidences of these outcomes, with corresponding tabular data in eTables 1 to 4 in Supplement 1.
Estimated Cardiometabolic Risk Among Patients With Primary Hyperparathyroidism and Matched ControlsKaplan-Meier survival curves are shown for the development of hypertension (A), type 2 diabetes (B), cardiovascular disease (CVD) (C), and cerebrovascular accident (CVA) (D) in patients with primary hyperparathyroidism (pHPT) and matched controls. Estimates were adjusted for age, sex, body mass index, smoking status, and relevant comorbidities.
Nonsurgical Treatment vs Parathyroidectomy
The matched cohort included 6654 patients who underwent parathyroidectomy and 19 962 patients who did not undergo surgery. Baseline characteristics were well balanced between groups, with SMDs less than 0.10 for age, sex, ethnicity, and SES. The mean (SD) age was 58 (12) years in both groups. In the nonsurgical management group, 14 403 patients (72.2%) were female and 5559 (27.8%) were male; in the parathyroidectomy group, 4801 (72.2%) were female and 1853 (27.8%) were male. Comorbidity burden and background diagnoses were comparable, with only minor imbalances that remained within acceptable thresholds for matched analyses. Among patients who underwent parathyroidectomy, the mean (SD) time from diagnosis to surgery was 879 (1219) days (Table 3).
Outcomes After Parathyroidectomy
Table 4 provides a detailed comparison of outcomes in patients with pHPT who underwent parathyroidectomy vs those who underwent nonsurgical management. During follow-up, T2D incidence was lower in the surgical group (10.77 [95% CI, 9.80-11.83] vs 15.18 [95% CI, 14.58-15.81] per 1000 person-years; AHR, 0.56 [95% CI, 0.30-0.89]; P = .002). For CVA, incidence was 12.93 (95% CI, 11.92-14.03) vs 14.12 (95% CI, 13.55-14.70) per 1000 person-years (AHR, 0.79; 95% CI, 0.50-1.13; P = .09), indicating a nonsignificant pattern. CVD occurred at an incidence of 11.57 (95% CI, 10.57-12.66) vs 12.49 (95% CI, 11.94-13.07) per 1000 person-years (AHR, 0.93; 95% CI, 0.85-1.02; P = .92), and hypertension at an incidence of 45.89 (95% CI, 42.99-49.00) vs 48.85 (95% CI, 47.32-50.43) per 1000 person-years (AHR, 1.19; 95% CI, 0.69-1.96; P = .33), with no significant differences between groups.
Discussion
This nationwide cohort study provides comprehensive insights into the cardiometabolic implications of pHPT and the impact of parathyroidectomy. In our analysis of 50 199 patients with pHPT compared with 150 265 matched controls, we found that pHPT was associated with significantly increased long-term risks of hypertension, T2D, CVD, and CVA. Among the 6654 patients who underwent parathyroidectomy, surgery was associated with a significantly reduced incidence of T2D, whereas no associations were observed for hypertension, CVD, or CVA. These findings highlight both the systemic burden of pHPT and the selective metabolic benefit of surgical intervention.
The observed associations suggest that pHPT contributes to the development and progression of multiple cardiometabolic conditions through systemic effects that extend beyond calcium and bone metabolism. Prolonged elevations in PTH levels have been linked to vascular endothelial dysfunction, insulin resistance, left ventricular hypertrophy, and increased arterial stiffness. These mechanisms may underlie the increased incidence of hypertension, T2D, and atherosclerotic events observed in this cohort, underscoring the importance of early recognition and comprehensive management of pHPT.
Our findings align with previous findings from the literature concerning the cardiovascular burden in patients with pHPT.^4,17^ Antignani et al^4^ highlighted that pHPT contributes to vascular stiffness and hypertension due to hypercalcemia affecting vascular smooth muscle function, an observation that aligns with our reported outcomes. Moreover, Agarwal et al^17^ discussed broader cardiovascular mechanisms, such as vascular calcification and endothelial dysfunction, supporting our observations of the systemic nature of pHPT’s association with cardiovascular health. While these mechanisms are well established, our study quantifies the clinical impact across a broad range of cardiovascular outcomes, particularly T2D and a possible pattern of cerebrovascular events, which have been less emphasized in previous literature. Notably, the large scale of our cohort allows for high-quality comparisons with strong statistical power, positioning it among the most comprehensive retrospective analyses of pHPT-related cardiovascular risk to date.^22^
Besides confirming elevated cardiovascular risk, we provide critical insights into the impact of parathyroidectomy. Our results show that parathyroidectomy was associated with reduced incidence of T2D (AHR, 0.56; 95% CI, 0.30-0.89; P = .002). Our results align with those recently reported by Liu et al,^26^ who demonstrated that parathyroidectomy was associated with a lower risk of incident T2D in patients with pHPT, particularly among younger individuals and those with more severe biochemical disease. While their study focused primarily on glycemic outcomes in a smaller cohort, our nationwide analysis extends these observations by evaluating the impact of parathyroidectomy on a broader range of cardiometabolic outcomes in more than 26 000 patients with pHPT. Consistent with the findings reported by Liu et al,^26^ we found that parathyroidectomy was associated with reduced incidence of T2D. However, in contrast to some previous reports,^22,27,28^ no clear benefits were observed for hypertension, CVD, or CVA. This discrepancy may stem from long-term vascular remodeling caused by chronic hypercalcemia and elevated PTH levels, which might not fully reverse after surgery, especially given the prolonged time to intervention (mean 879 [1219] days). Taken together, these findings reinforce the metabolic benefit of surgery on glycemic outcomes while suggesting that other cardiometabolic risks may persist despite surgical intervention.
From a clinical management perspective, whether cardiovascular screening should become routine in pHPT remains unanswered. Despite accumulating evidence of heightened risk, current guidelines do not consistently recommend cardiovascular evaluation in these patients. Our findings highlight the increased cardiovascular risk in patients with pHPT and the potential for parathyroidectomy to mitigate some of these risks, particularly T2D and cerebrovascular events. While these associations suggest possible benefits of integrating cardiovascular risk assessment into the management of pHPT, further prospective studies are needed to determine whether such strategies improve long-term outcomes and to clarify the role of surgical referral practices and health care access in shaping these results. This study was conducted within CHS, the largest integrated health care organization in Israel, which provides universal coverage to more than half of the national population and includes a diverse patient population across ethnic and socioeconomic backgrounds; this fact enhances the potential applicability of our findings to other universal health care systems that care for heterogeneous populations. While all patients in our cohort were covered under the same nationwide health maintenance organization, which reduces heterogeneity in access and insurance coverage, unmeasured factors such as geographic variation, physician referral practices, and patient preferences may still influence surgical decision-making. These aspects could not be fully assessed in our study and warrant further investigation.
Limitations
The retrospective design of this study introduces several inherent limitations, including potential residual confounding and dependence on the accuracy of medical record data. Although we used a large and comprehensive database, some variables, particularly lifestyle factors (eg, diet, physical activity, smoking), were unavailable, limiting our ability to fully adjust for all relevant confounders. Another limitation is the absence of detailed symptom documentation, which prevented assessment of symptom resolution. To address baseline imbalances, we performed propensity score matching on age, sex, and SES, which achieved good balance across groups (all SMDs <0.10). Nonetheless, residual confounding may persist, particularly due to unmeasured factors such as comorbidity burden, biochemical disease severity, or physician referral practices that may have influenced surgical referral. In addition, excluding patients with preexisting cardiometabolic conditions may have underestimated the overall burden of pHPT, as undiagnosed cases might have been missed. Finally, lack of consistent postoperative calcium and PTH data precluded analysis of whether biochemical normalization mediates risk reduction. These limitations may affect the precision of our estimates.
Conclusions
In this cohort study of patients with pHPT, the condition was associated with increased long-term cardiometabolic risks. Parathyroidectomy was associated with a significantly reduced incidence of T2D, while no associations were observed for hypertension, CVD, or CVA. These findings support a potential role for surgical intervention in modifying selected cardiometabolic outcomes in this population. Further prospective studies are needed to confirm these observations and to clarify the broader impact of parathyroidectomy on long-term cardiovascular health.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Beysel S, Caliskan M, Kizilgul M, . Parathyroidectomy improves cardiovascular risk factors in normocalcemic and hypercalcemic primary hyperparathyroidism. BMC Cardiovasc Disord. 2019;19(1):106. doi:10.1186/s 12872-019-1093-4 31068134 PMC 6505186 · doi ↗ · pubmed ↗
- 2Macfarlane DP, Yu N, Leese GP. Asymptomatic and mild primary hyperparathyroidism. Ann Endocrinol (Paris). 2015;76(2):120-127. doi:10.1016/j.ando.2015.03.001 25882891 · doi ↗ · pubmed ↗
- 3Pepe J, Cipriani C, Sonato C, Raimo O, Biamonte F, Minisola S. Cardiovascular manifestations of primary hyperparathyroidism: a narrative review. Eur J Endocrinol. 2017;177(6):R 297-R 308. doi:10.1530/EJE-17-0485 28864535 · doi ↗ · pubmed ↗
- 4Antignani PL, Jezovnik MK, Blinc A, . Hyperparathyroidism and peripheral arterial disease. Curr Vasc Pharmacol. 2024;22(2):88-94. doi:10.2174/0115701611280905231227045826 38284694 · doi ↗ · pubmed ↗
- 5Iglesias P, Arias J, López G, Romero I, Díez JJ. Primary hyperparathyroidism and cardiovascular disease: an association study using clinical natural language processing systems and big data analytics. J Clin Med. 2023;12(21):6718. doi:10.3390/jcm 12216718 37959184 PMC 10650925 · doi ↗ · pubmed ↗
- 6Bernardi S, Giudici F, Barbato V, Zanatta L, Grillo A, Fabris B. Meta-analysis on the effect of mild primary hyperparathyroidism and parathyroidectomy upon arterial stiffness. J Clin Endocrinol Metab. 2021;106(6):1832-1843. doi:10.1210/clinem/dgab 157 33693666 · doi ↗ · pubmed ↗
- 7Modica R, Liccardi A, Minotta R, Benevento E, Cannavale G, Colao A. Parathyroid diseases and metabolic syndrome. J Endocrinol Invest. 2023;46(6):1065-1077. 36773188 10.1007/s 40618-023-02018-2PMC 10185585 · doi ↗ · pubmed ↗
- 8Purra S, Lone AA, Bhat MH, . Cardiac structural and functional abnormalities in primary hyperparathyroidism. J Endocrinol Invest. 2022;45(2):327-335. doi:10.1007/s 40618-021-01645-x 34324161 · doi ↗ · pubmed ↗