Cognitive Outcomes of Children Exposed to Selective Serotonin Reuptake Inhibitors Through Breast Milk
Essi Whaites Heinonen, Kelly Kao, Sarah N. Mattson, Christina D. Chambers

TL;DR
Breastfeeding while taking SSRIs does not harm children's cognitive development, according to a study of 97 children.
Contribution
This is the first study to investigate the cognitive effects of SSRI exposure through breastfeeding.
Findings
Children exposed to SSRIs through breastfeeding had similar IQ scores to those not exposed.
Initial higher IQ scores in breastfed SSRI-exposed children disappeared after adjusting for maternal mood factors.
The study supports the safety of breastfeeding during SSRI treatment for cognitive outcomes.
Abstract
Is maternal treatment with selective serotonin reuptake inhibitors (SSRIs) during breastfeeding associated with cognitive performance of the offspring? This cohort study of 97 children who were exposed to maternal treatment with SSRIs during pregnancy with or without exposure during breastfeeding underwent testing with the Wechsler Scales of Preschool and Primary Intelligence. Fully adjusted mean full-scale, verbal, and performance IQ scores were similar among breastfed children exposed to SSRIs, breastfed children not exposed to SSRIs, and nonbreastfed children. These findings suggest that maternal treatment with SSRIs during breastfeeding does not affect the cognitive performance of the offspring. This cohort study compares cognitive performance in preschool-aged children who were exposed to selective serotonin reuptake inhibitors (SSRIs) during pregnancy and breastfeeding, those…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
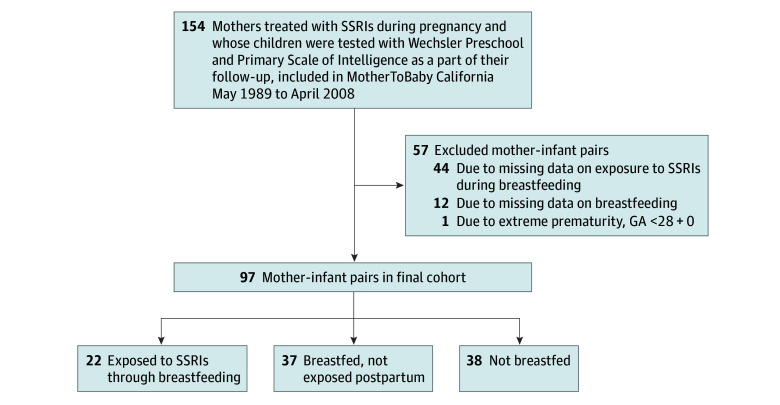 Figure 1
Figure 1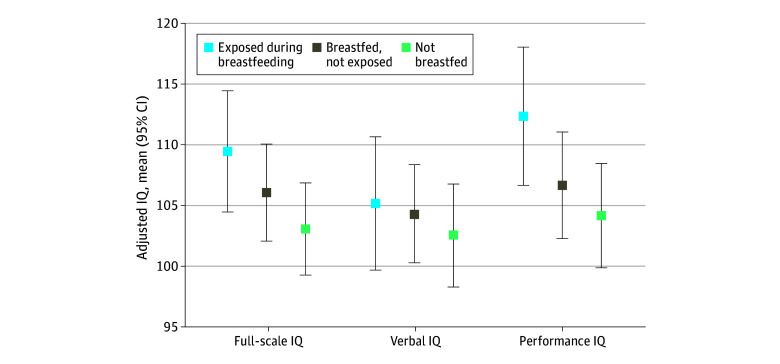 Figure 2
Figure 2| Characteristic | Participant group, No. (%) | |||
|---|---|---|---|---|
| SSRI exposure during breastfeeding (n = 22) | Breastfed but no SSRI exposure (n = 37) | Not breastfed (n = 38) | ||
|
| ||||
| Maternal age at delivery, mean (SD), y | 35.5 (5.4) | 33.2 (5.3) | 33.9 (6.0) | .18 |
| Primipara | 11 (50.0) | 18 (48.6) | 20 (52.6) | .94 |
| Race and ethnicity | ||||
| Hispanic or Latina | 1 (4.5) | 3 (8.1) | 4 (10.8) | .98 |
| Non-Hispanic White | 20 (90.9) | 32 (86.5) | 32 (86.5) | |
| Other | 1 (4.5) | 2 (5.4) | 1 (2.7) | |
| Socioeconomic scale | .32 | |||
| 1-3 | 20 (100) | 31 (88.6) | 32 (94.1) | |
| 4-5 | 0 | 4 (11.4) | 2 (5.9) | |
| Duration of treatment with SSRIs during pregnancy, mean (SD), wk | 35.0 (11.2) | 14.0 (12.4) | 28.0 (14.8) | <.001 |
| Indication for treatment with SSRIs | ||||
| Major depressive disorder | 17 (77.3) | 23 (62.2) | 28 (73.7) | .15 |
| Anxiety or panic disorder | 1 (4.5) | 4 (10.8) | 2 (5.3) | |
| Depression with other psychiatric disorders | 1 (4.5) | 0 | 4 (10.5) | |
| Other | 2 (9.1) | 10 (27.0) | 4 (10.5) | |
| Tobacco use during pregnancy | 1 (4.5) | 4 (10.8) | 9 (27.3) | .07 |
| Alcohol use during pregnancy | 13 (59.1) | 26 (70.3) | 9 (27.3) | <.001 |
| Psychotropic comedications during pregnancy | 2 (9.1) | 8 (21.6) | 15 (39.5) | .03 |
| CES-D score during pregnancy ≥16 | 10 (50.0) | 14 (43.8) | 19 (59.4) | .45 |
| CES-D score during pregnancy, mean (SD) | 19.5 (15.3) | 16.2 (13.3) | 24.4 (16.5) | .09 |
| CES-D score at the time of testing ≥16 | 7 (36.8) | 12 (38.7) | 15 (46.9) | .72 |
| CES-D score at the time of testing, mean (SD) | 15.0 (14.3) | 16.6 (13.4) | 17.5 (13.9) | .68 |
| Maternal IQ, mean (SD) | 120.8 (7.5) | 116.4 (5.4) | 110.1 (14.7) | .14 |
| Data availability for maternal IQ | 6 (27.3) | 11 (29.7) | 14 (36.8) | .70 |
|
| ||||
| Gestational age at delivery, mean (SD), wk | 39.5 (1.3) | 39.4 (1.4) | 39.2 (1.5) | .96 |
| Late preterm infants | 1 (4.5) | 1 (2.7) | 3 (7.9) | .84 |
| Sex | ||||
| Female | 10 (45.5) | 21 (56.8) | 21 (55.3) | .68 |
| Male | 12 (54.5) | 16 (43.2) | 17 (44.7) | |
| Admitted to neonatal intensive care | 6 (27.3) | 5 (13.5) | 6 (15.8) | .12 |
| Exclusive breastfeeding | 14 (87.5) | 18 (72.0) | NA | .44 |
| Breastfeeding duration at least, mean (SD), mo | 14.1 (9.0) | 5.0 (5.0) | NA | .002 |
| Data availability for breastfeeding duration | 11 (50.0) | 16 (43.2) | NA | .79 |
|
| ||||
| Child age at testing, mean (SD), y | 4.8 (0.6) | 4.9 (0.7) | 4.9 (0.8) | .99 |
| Year of testing | ||||
| 1996-2005 | 21 (95.5) | 37 (100) | 36 (94.7) | .44 |
| 2006-2012 | 1 (4.5) | 0 | 2 (5.3) | |
| WPPSI composite score | Participant group | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SSRI exposure during breastfeeding (n = 22) | Breastfed but no SSRI exposure (n = 37) | |||||||||||
| Mean (SD) | Adjustment 1 mean (95% CI) | Adjustment 2 mean (95% CI) | Adjustment 3 mean (95% CI) | Mean (SD) | Adjustment 1 mean (95% CI) | Adjustment 2 mean (95% CI) | Adjustment 3 mean (95% CI) | Crude | Adjustment 1 | Adjustment 2 | Adjustment 3 | |
| FSIQ | 109.4 (12.1) | 109.6 (104.4-114.8) | 109.3 (104.0-114.6) | 112.0 (105.7-118.3) | 106.2 (12.1) | 106.1 (102.1-110.1) | 106.5 (102.5-110.6) | 104.3 (99.7-109.0) | .34 | .29 | .41 | .08 |
| VIQ | 105.0 (12.9) | 105.3 (100.0-110.6) | 105.5 (100.2-110.9) | 110.3 (103.9-116.6) | 104.5 (12.2) | 104.3 (100.3-108.4) | 104.8 (100.6-108.9) | 101.7 (97.0-106.3) | .89 | .77 | .82 | .05 |
| PIQ | 112.4 (14.3) | 112.5 (106.7-118.2) | 111.6 (105.7-117.5) | 110.9 (103.5-118.3) | 106.8 (12.3) | 106.7 (102.3-111.1) | 107.1 (102.5-111.6) | 106.5 (101.0-111.9) | .11 | .12 | .23 | .38 |
| WPPSI composite score | Participant group | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SSRI exposure during breastfeeding (n = 22) | Not breastfed (n = 38) | |||||||||||
| Mean (SD) | Adjustment 1 mean (95% CI) | Adjustment 2 mean (95% CI) | Adjustment 3 mean (95% CI) | Mean (SD) | Adjustment 1 mean (95% CI) | Adjustment 2 mean (95% CI) | Adjustment 3 mean (95% CI) | Crude | Adjustment 1 | Adjustment 2 | Adjustment 3 | |
| FSIQ | 109.4 (12.1) | 109.4 (104.5-114.4) | 109.0 (103.3-114.7) | 108.3 (102.4-114.3) | 103.1 (10.9) | 103.1 (99.3-106.9) | 103.4 (98.9-107.8) | 105.6 (100.8-110.5) | .05 | .046 | .14 | .52 |
| VIQ | 105.0 (12.9) | 105.1 (99.5-110.7) | 105.5 (99.0-111.9) | 105.2 (98.4-112.0) | 102.6 (12.7) | 102.6 (98.3-106.8) | 102.8 (97.8-107.8) | 105.6 (100.2-111.0) | .49 | .48 | .54 | .93 |
| PIQ | 112.4 (14.3) | 112.3 (106.7-118.0) | 112.0 (105.6-118.4) | 110.8 (104.0-117.7) | 104.2 (12.2) | 104.2 (99.9-108.5) | 103.9 (99.0-108.9) | 105.1 (99.6-110.6) | .03 | .03 | .06 | .23 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal Mental Health During Pregnancy and Postpartum · Breastfeeding Practices and Influences · Infant Development and Preterm Care
Introduction
The cognitive development of children exposed to maternal treatment with selective serotonin reuptake inhibitors (SSRIs) during pregnancy has been studied extensively.^1,2,3,4,5^ Most previous studies have shown either no significant effects of prenatal SSRI exposure on the child development or effects that were attenuated or eliminated after adjustments for factors related to the underlying maternal disorder.^1,5^ However, to our knowledge, the association between child cognitive performance and exposure to SSRIs through breastfeeding has not been previously examined. This question is of clinical importance, as some breastfeeding mothers still avoid antidepressant use due to the effects treatment may pose for the breastfed infant.^6,7,8,9^
SSRIs are known to transfer to breast milk with maximum relative infant doses of 4% to 12%, with fluoxetine hydrochloride, citalopram, and escitalopram transferring to the highest degree.^10,11,12^ Although the level of drug exposure is lower through breastfeeding than through placental transfer, there is at least a theoretical risk that the highly lipophilic SSRIs ingested by the breastfed infant could negatively affect the infant’s brain maturation.^10,13,14,15,16,17^ However, breastfeeding itself is known to have numerous positive effects, including on the cognitive development of the child.^15,18,19^ These benefits may well outweigh any potential negative effects that exposure to SSRIs through breast milk may have. Exclusive breastfeeding for at least 6 months is recommended for all infants, and hence, it is essential to provide adequate safety data for the long-term development of children exposed to SSRIs through breastfeeding to address remaining avoidant behavior regarding breastfeeding among mothers treated with SSRIs.^6,7,20^
In this study, we compared the cognitive performance measured with the Wechsler Primary and Preschool Test of Intelligence (WPPSI) in preschool-aged children among those who were exposed to SSRIs during pregnancy and breastfeeding, those who were breastfed but only exposed during pregnancy, and those who were not breastfed. We hypothesized that the IQ scores of children exposed to SSRIs during breastfeeding would be comparable to the scores of children breastfed without postnatal SSRI exposure and somewhat higher than the scores of nonbreastfed children.
Methods
Design and Setting
This cohort study was a secondary analysis of data in the MotherToBaby California cohort that was open for enrollment for all English- and Spanish-speaking women in California. Women were eligible to enroll in the study if they did not have prior knowledge of the pregnancy outcome and agreed to the study protocol. The study design and methods have been described in detail elsewhere.^21,22,23^ Briefly, pregnant women were referred or self-referred into the single site research center during pregnancy and all liveborn infants were followed up to a minimum of 1 year after birth. Depending on their exposures, some participants, including those treated with SSRIs, were also invited to take part in face-to-face neurodevelopmental testing of the child when the child reached preschool age. Exposure, outcome, and covariate information during pregnancy and in the postpartum period were obtained through repeated telephone interviews and confirmed by medical records when available. Additional information was obtained at the time of neurodevelopmental testing.
For this analysis, eligible participants who enrolled in the MotherToBaby California cohort between May 18, 1989, and April 14, 2008, were treated with SSRIs at the time of enrollment in early pregnancy, and their children were tested with the WPPSI between April 30, 1996, and August 21, 2012. Mothers with missing information on breastfeeding and postnatal SSRI treatment as well as 1 extremely preterm child were excluded (Figure 1). The data were analyzed from January 10 to May 16, 2025. Institutional Review Board approval was obtained for the parent study from the University of California, San Diego, and San Diego State University. All participants provided written informed consent. The study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
Flowchart of Study CohortGA indicates gestational age (in weeks and days); SSRI, selective serotonin reuptake inhibitor.
Exposures
All mothers were treated with SSRIs during pregnancy at inclusion to the cohort. In this study, the children who were exposed to SSRIs through breastfeeding were compared with children whose mothers discontinued SSRI treatment before breastfeeding. Secondarily, the children exposed to SSRIs through breastfeeding were compared with the children who were not breastfed (Figure 1). Breastfeeding was defined as a known breastfeeding duration of at least 1 month, and hence, participants with breastfeeding data only from newborn records were excluded.
Outcomes
The main outcomes were the composite scores of Full-Scale (FSIQ), Verbal (VIQ), and Performance IQ (PIQ) measured with the version of WPPSI available at the time of testing, the WPPSI Revised (WPPSI-R) or the WPPSI, Third Edition (WPPSI-III).^24,25^ The composite scores of the WPPSI tests are standardized to the age and sex of the child with a mean (SD) score of 100 (50) points. Secondary outcomes were scaled scores of 4 verbal and 8 nonverbal subtests of the WPPSI-R, with results from children tested with WPPSI-III included for the subtests that were similar to those in the WPPSI-R. These were also standardized to age and sex of the child with a mean (SD) of 10 (3) points. Included verbal subtests were Information, Comprehension, Vocabulary, and Similarities; nonverbal subtests were Picture Completion, Object Assembly, Block Design, Sentences, Arithmetic, Animal Pegs, Geometric Design, and Mazes. In a secondary analysis, we studied the correlations of the child IQ scores with maternal IQ and depressive symptoms.
Covariates
Data on baseline characteristics and covariates were collected through maternal telephone interviews and are presented in Table 1. Due to both SSRI use and breastfeeding frequency varying by race and ethnicity, maternal self-reported race and ethnicity were collected at the interviews. Race and ethnicity were collected as 2 separate variables and combined for this analysis. The original categories for race in the interviews were American Indian or Alaska Native, Asian, Black, Native Hawaiian or Other Pacific Islander, White, other, refused, not asked, and unknown; categories for ethnicity included Hispanic or Latina and non-Hispanic or non-Latina. For the present study, we combined these categories as Hispanic or Latina (including White, other, unknown, and Hispanic or Latina), non-Hispanic Black (including Black and non-Hispanic or non-Latina), non-Hispanic White (including White and non-Hispanic or non-Latina), and other (including American Indian or Alaska Native, Asian, Native Hawaiian or Other Pacific Islander, other, and non-Hispanic or non-Latina). Socioeconomic status was measured with the Hollingshead 4-Factor Index representing maternal and paternal educational attainment and occupation scored from 1 to 5 and categorized into high (1-3) and low (4-5) socioeconomic status.^26^ Maternal depressive symptoms were estimated with the Center for Epidemiological Studies Depression Scale (CES-D) administered at the time of neurodevelopmental testing or later, as the CES-D was not initially a part of the testing procedure and was in some cases administered retroactively. In all cases, the mother was asked to rate their symptoms of depression both currently and retrospectively during the target pregnancy. A cutoff of 16 points was set for depressive symptoms, indicating a potential risk of clinical depression.^27^ In a subset of the cohort, maternal IQ was measured at the time of the child neurodevelopmental testing with the Wechsler Adult Scale of Intelligence. Covariates included in the adjusted analyses were child age at testing (continuous), child sex (binary), and prematurity (born at 34-36 weeks of gestation [binary]). In sensitivity analyses, maternal use of other psychotropic comedications (binary) and alcohol (binary) during pregnancy as well as the duration of treatment with SSRIs during pregnancy (continuous) and maternal CES-D scores during pregnancy (continuous) were included as covariates.
Statistical Analysis
First, distributions of the IQ scores were analyzed, and all scores and their residuals were determined to be approximately normally distributed. Baseline characteristics were compared between groups using the Pearson χ^2^ and Kruskal-Wallis tests, as appropriate. To study the potential association of the postnatal SSRI exposure with the child IQ scores separately from the association with breastfeeding, children exposed to SSRIs during breastfeeding were compared separately with breastfed children without postnatal SSRI exposure and nonbreastfed children. The crude results of both composite scores and scaled scores were measured as means (SDs) and compared between groups with an independent samples t test. The adjusted mean scores and their 95% CIs were analyzed with 1-way analysis of covariance adjusted for child age at testing, child sex, and prematurity (adjustment 1). In sensitivity analyses, the use of other psychotropic comedications and alcohol during pregnancy (adjustment 2) and duration of treatment with SSRIs during pregnancy and maternal CES-D scores during pregnancy (adjustment 3) were added to the model in a stepwise manner. The level of statistical significance was set as a 2-sided P < .05. In a secondary analysis, the Spearman correlation was used for exploring correlations between child IQ scores and maternal IQ scores and depressive symptoms. Cases with missing data on included covariates were excluded from adjusted analyses. Statistical analyses were performed with SPSS Statistics for Windows, version 29.0 (IBM Corporation).
Results
Participants
After exclusions for missing data on breastfeeding or postnatal SSRI exposure and prematurity, the final cohort consisted of 97 mother-child dyads (Figure 1). Of the 97 children, 52 (53.6%) were female and 45 (46.4%) male, and the mean (SD) age at cognitive testing was 4.9 (0.7) years. The mean (SD) maternal age at delivery was 34.0 (5.6) years. All 97 mothers identified as women. Eight women (8.2%) identified as Hispanic or Latina, 84 (86.6%) as non-Hispanic White, and 4 (4.1%) as other race or ethnicity, with 1 missing.
Background Characteristics
The children were categorized into those exposed to SSRIs with breastfeeding (22 [22.7%]), breastfed children without postnatal SSRI exposure (37 [38.1%]), and nonbreastfed children, (38 [39.2%]). Eighty-one mothers (83.5%) were treated with fluoxetine hydrochloride. Other SSRIs included sertraline hydrochloride (9 [9.3%]), paroxetine (8 [8.2%]), and citalopram (2 [2.1%]). Three participants (3.1%) switched between SSRIs during pregnancy. The mean (SD) duration of treatment with SSRIs during pregnancy was 24.2 (15.6) weeks, with mothers who breastfed without SSRI treatment having a significantly shorter mean treatment duration than the 2 other groups (14.0 [12.4] weeks vs 35.0 [11.2] and 28.0 [14.9] weeks; P < .001) (Table 1). Twenty-five mothers (25.8%) were also treated with other psychotropic medications during pregnancy, including significantly fewer of the mothers who breastfed while treated with SSRIs (2 of 22 [9.1%]) than mothers who breastfed without SSRI treatment (8 of 37 [21.6%]) and mothers who did not breastfeed (15 of 38 [39.5%]) (P = .03) (Table 1). The other psychotropic medications used during pregnancy included benzodiazepines (16 of 97 [16.5%]), antipsychotics (5 of 97 [5.2%]), antiepileptic drugs (3 of 97 [3.1%]), tricyclic antidepressants (2 of 97 [2.1%]), lithium (2 of 97 [2.1%]), and buspirone hydrochloride (2 of 97 [2.1%]). During breastfeeding, 9 of 59 mothers (15.3%) reported any comedications, but none of these were other psychotropic medications. No participants reported any use of illicit drugs or cannabis during pregnancy, but 14 of 89 with data available (15.7%) reported use of tobacco and 48 of 89 (53.9%) reported use of alcohol at some point during pregnancy, with a significantly higher percentage of mothers who breastfed with and without SSRI use (13 of 22 [59.1%] and 26 of 37 [70.3%]) than mothers who did not breastfeed (9 of 38 [23.7%]) reporting alcohol use during pregnancy (Table 1). There were no differences between groups in maternal IQ, tested in a subset of 31 mothers (32.0%), or maternal depressive symptoms during pregnancy or at the time of developmental testing (Table 1).
Of the 97 children, 5 (5.2%) were born late preterm between gestational weeks 34 0/7 and 36 6/7. There was no significant difference in prematurity rates between exposure groups (Table 1). Seventeen children (17.5%) needed neonatal intensive care, without any significant differences among exposure groups. The mean (SD) documented duration of breastfeeding across the sample was 8.4 (8.2) months. Cognitive testing was performed with the WPPSI-R for 92 children (94.8%) and with the WPPSI-III for 5 children (5.2%).
Composite Child IQ Scores
The mean (SD) FSIQ was 105.8 (11.8), corresponding to the 62nd percentile; VIQ, 103.9 (12.5), corresponding to the 58th percentile; and PIQ, 107.0 (13.0), corresponding to the 64th percentile. The adjusted mean FSIQ in children exposed to SSRIs through breastfeeding (109.4; 95% CI, 104.5-114.4) was similar to that in breastfed children not exposed to SSRIs through breastfeeding (106.1; 95% CI, 102.1-110.1; P = .29) and 6.3 points higher than in nonbreastfed children (103.1; 95% CI, 99.3-106.9; P = .046) (Table 2, Table 3, and Figure 2). The adjusted mean PIQ of the breastfeeding-exposed children was not significantly higher than of breastfed children not exposed to SSRIs post partum (112.3 [95% CI, 106.7-118.0] compared with 106.7 [95% CI, 102.3-111.1]; P = .12) but 8.1 points higher than the adjusted mean PIQ of nonbreastfed children (104.2; 95% CI, 99.9-108.5; P = .03). The adjusted mean VIQ scores were similar among all exposure groups. The differences in mean FSIQ and PIQ between the children exposed to SSRIs through breastfeeding and the nonbreastfed children were no longer statistically significant after further adjustments for factors related to maternal mood during pregnancy (Tables 2 and 3).
Adjusted Mean IQ Score of Children Exposed to Selective Serotonin Reuptake Inhibitors Through Breastfeeding, Breastfed Children Not Exposed Post Partum, and Nonbreastfed ChildrenAdjusted means calculated between groups with 1-way analysis of covariance adjusted for child age at testing, child sex, and prematurity.
Scores of Subtests
Comparisons of the scaled scores of the common subtests of WPPSI-R and WPPSI-III, as well as the subtests only included in WPPSI-R, are presented in eTables 1 and 2 in Supplement 1. All of the adjusted mean scores of the subtests across the groups were within 2 points of the standardized mean (SD) score of 10 (3) points, apart from Picture Completion. For Picture Completion, the adjusted mean scores were 1 SD above the standardized mean in all exposure groups (eTables 1 and 2 in Supplement 1). The adjusted mean results from 2 nonverbal subtests, Geometric Design and Mazes, were statistically significantly higher among children exposed to SSRIs during breastfeeding than nonbreastfed children, but the differences between adjusted group means were less than 2 points, and the adjusted mean scores of the remaining 10 subtests did not differ between exposure groups (eTable 2 in Supplement 1).
Correlations
In the 83 children (85.6%) with available data on maternal CES-D scores, the FSIQ and VIQ scores were negatively correlated with the maternal estimated CES-D scores for the pregnancy period (R = −0.26 [P = .02] and R = −0.26 [P = .02], respectively). After stratification by exposure group, these correlation coefficients stayed constant but were no longer significant. There was no significant correlation between maternal CES-D scores during pregnancy and PIQ or between maternal CES-D scores at the time of neurodevelopmental testing and child IQ. In the 31 children (32.0%) with data available on maternal IQ, there was no significant correlation between maternal and child IQ.
Discussion
In this cohort study of children born to mothers treated with SSRIs during pregnancy, the mean FSIQ, VIQ, and PIQ scores were similar between breastfed children with and without postnatal exposure to SSRIs. In the comparison between breastfed, postnatally SSRI-exposed children and nonbreastfed children, the FSIQ and PIQ scores of the breastfed, SSRI-exposed children were approximately one-half of an SD higher than the scores of their nonbreastfed counterparts. However, these differences were no longer significant after further adjustments for factors related to maternal mood during pregnancy. These results are supported by the comparison of the adjusted means of the subtests of WPPSI, which showed no significant differences between groups in the mean scores of the verbal subtests and slightly, but statistically significantly, higher mean scores of 2 of the nonverbal subtests in children exposed to SSRIs during breastfeeding than in nonbreastfed children.
The differences in FSIQ and PIQ scores between breastfed and nonbreastfed children in this SSRI-exposed cohort are of the same magnitude as the positive effects of breastfeeding seen on the cognitive development in the general population and in children exposed to maternal antiepileptic medications.^18,19^ This is, to our knowledge, a novel finding, supporting breastfeeding in mothers in need of treatment with SSRIs. However, the differences in FSIQ and PIQ between the breastfed SSRI-exposed and the nonbreastfed infants were no longer significant after adjustment for maternal factors, and there was a significant negative correlation between depressive symptoms during pregnancy and child IQ. Hence, these results also support the association between maternal mood disorders and the long-term development of the children described by previous studies.^28,29^
Strengths and Limitations
The largest strength of this study was the standardized face-to-face testing of the exposed infants, which has previously been performed in only a limited number of studies on children prenatally exposed to SSRIs, and the differentiation on whether the children had been exposed during breastfeeding or not, which to our knowledge was unique.^2,4,30^ However, others have had a wider definition of cognitive performance and development, combining tests of cognitive performance, motor development, and parental questionnaires, or studied the relevant codes of International Classification of Diseases diagnoses in national registries.^1,2,31^ As these previous studies have not studied exposure during breastfeeding, our findings of the children exposed to SSRIs during breastfeeding performing as well as breastfed children without postnatal SSRI exposure are novel. These findings need to be confirmed by other studies with different outcome measures to acquire a more complete picture of the development of postnatally SSRI-exposed children.
This study also has some limitations. The secondary analysis of data previously collected for pregnancy studies was limited by the availability of breastfeeding data. Approximately one-third of the initial cohort was excluded due to missing data on breastfeeding and/or postpartum exposure to medications. After comparing the background characteristics and child IQs of these excluded mother-infant dyads with the rest of the cohort, we concluded that the missingness of breastfeeding questionnaires in these dyads was not differentially related to either the measured background characteristics or child IQ. Another limitation was that maternal depressive symptoms during pregnancy were measured retrospectively. Therefore, these scores were not included in the main analyses. Last, the cohort was based on volunteers and may not be representative of the general population. For example, all adjusted mean FSIQ, VIQ, and PIQ scores were above the average standardized means for the testing instrument. Therefore, caution should be used when comparing the IQ scores with those of other cohorts. However, as the background demographic characteristics were similar between exposure groups, there is support for the internal validity of the study. Larger and more diverse samples are needed to support the generalizability of these findings.
Conclusions
In this prospective cohort study of children prenatally exposed to SSRIs, breastfed infants whose mothers were treated with SSRIs during breastfeeding had similar FSIQ, PIQ, and VIQ as breastfed infants who were SSRI exposed during pregnancy but not breastfeeding, and before adjustment for factors related to maternal mood during pregnancy, with somewhat higher FSIQ and PIQ scores than those of nonbreastfed children exposed to SSRIs during pregnancy. These findings are in line with previous studies that have shown positive effects of breastfeeding on child IQ. Based on these results, as well as other studies in the field, we conclude that mothers in need of treatment with SSRIs post partum may be encouraged to breastfeed without discontinuation of the treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Suarez EA, Bateman BT, Hernández-Díaz S, . Association of antidepressant use during pregnancy with risk of neurodevelopmental disorders in children. JAMA Intern Med. 2022;182(11):1149-1160. 36190722 10.1001/jamainternmed.2022.4268 PMC 9531086 · doi ↗ · pubmed ↗
- 2Galbally M, Lewis AJ, Buist A. Child developmental outcomes in preschool children following antidepressant exposure in pregnancy. Aust N Z J Psychiatry. 2015;49(7):642-650. 25698806 10.1177/0004867415569800 · doi ↗ · pubmed ↗
- 3Hermansen TK, Røysamb E, Augusti EM, Melinder A. Behavior and inhibitory control in children with prenatal exposure to antidepressants and medically untreated depression. Psychopharmacology (Berl). 2016;233(8):1523-1535. 26924747 10.1007/s 00213-016-4248-3 · doi ↗ · pubmed ↗
- 4Nulman I, Koren G, Rovet J, . Neurodevelopment of children following prenatal exposure to venlafaxine, selective serotonin reuptake inhibitors, or untreated maternal depression. Am J Psychiatry. 2012;169(11):1165-1174. 23128923 10.1176/appi.ajp.2012.11111721 · doi ↗ · pubmed ↗
- 5Rommel AS, Bergink V, Liu X, Munk-Olsen T, Molenaar NM. Long-term effects of intrauterine exposure to antidepressants on physical, neurodevelopmental, and psychiatric outcomes: a systematic review. J Clin Psychiatry. 2020;81(3):19r 12965. 32412703 10.4088/JCP.19r 12965 PMC 8739257 · doi ↗ · pubmed ↗
- 6Gorman JR, Kao K, Chambers CD. Breastfeeding among women exposed to antidepressants during pregnancy. J Hum Lact. 2012;28(2):181-188. 22344850 10.1177/0890334411429782 · doi ↗ · pubmed ↗
- 7Whaites Heinonen E, Johnson DL, Todd A, Chambers CD. Lower adherence to breastfeeding recommendations in mothers treated with antirheumatic and antidepressant medications. J Hum Lact. 2025;41(3):412-422. 40432295 10.1177/08903344251337384 PMC 12238658 · doi ↗ · pubmed ↗
- 8Passier A, Woestenberg P. Chronic medication and breastfeeding, avoiding behavior in Dutch women. Neurotoxicol Teratol. 2023;98:107209.