A Vignette-Based Educational Intervention to Reduce Neurophobia and Improve Knowledge for the UK Medical Licensing Assessment: A Prospective Pilot Study
Zayna S Ahmed, Nigel Mason, Clare Galton

TL;DR
A short educational session improved medical students' confidence and knowledge in neurology, which could help reduce fear of the subject and improve patient care.
Contribution
A new MLA-aligned educational intervention was developed and tested to reduce neurophobia and improve neurology knowledge among medical students.
Findings
Confidence scores increased significantly after the intervention in both study cycles.
Knowledge, measured by SBA test scores, improved dramatically from 25% to 97.9% post-session.
Five out of six SBA items achieved 100% correct responses after the session.
Abstract
Introduction: Neurophobia, an aversion to clinical neurology, undermines medical education and may affect patient safety. The UK Medical Licensing Assessment (MLA) emphasizes vignette-based Single Best Answer (SBA) items, requiring practice in applied clinical reasoning. We developed a compact, MLA-aligned educational intervention to reduce neurophobia by improving confidence and knowledge. Methods: Using the Model for Improvement, we produced a 34-page booklet and delivered a 90-min, resident-led, interactive session across two plan-do-study-act cycles at a district general hospital (QIP: 25-586). Sixteen students participated (two cohorts, n=8 each), completing paired pre- and post-session assessments. While limited by a small sample size, this pilot supports proof of concept and warrants multicenter evaluation to strengthen generalizability. The primary outcome was self-rated…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
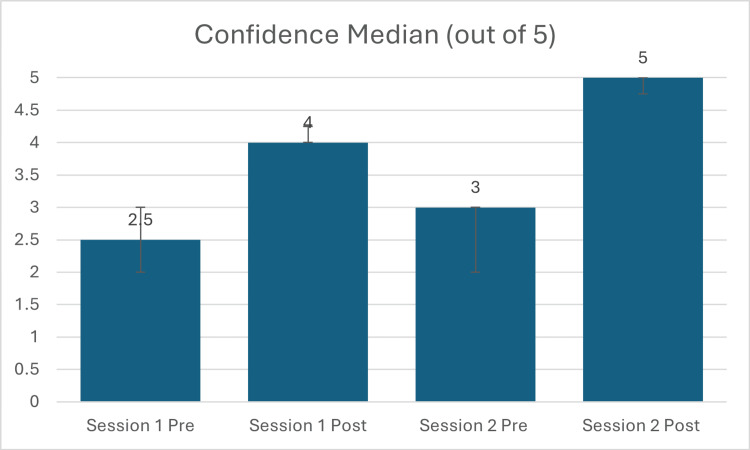 Figure 1
Figure 1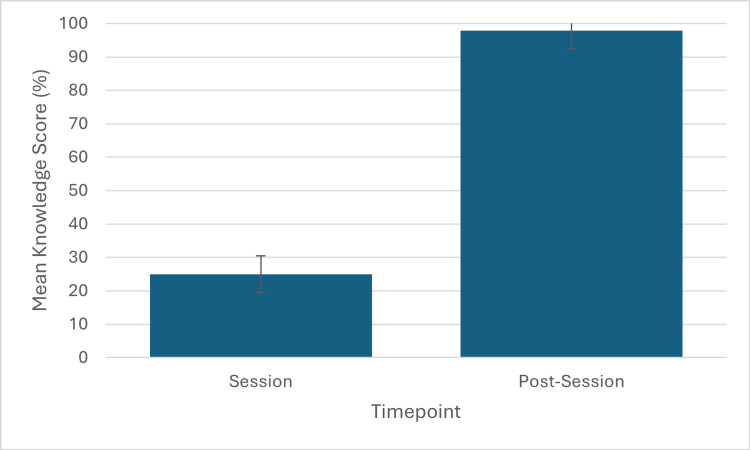 Figure 2
Figure 2| Cohort (n=8) | Outcome measures | Pre-intervention (median/mean) | Post-intervention (median/mean) | Test statistic (Z) | p-Value | Effect size (r) |
| Cycle 1 | Confidence, median (IQR/5) | 2.5 (2.0-3.0) | 4.0 (4.0-4.25) | -2.53 | <0.05 | 1.00 |
| Cycle 2 | Confidence, median (IQR/5) | 3.0 (2.0-3.0) | 5.0 (4.75-5.0) | -2.52 | <0.01 | 0.89 |
| Cycle 2 | Knowledge, mean%, (SD) → (normalized to a 5-point scale) | 25.0% (SD 8.3) ≈ 1.25/5 | 97.9% (SD 5.5) ≈ 4.90/5 | -2.55 | <0.01 | - |
| SBA question item | Pre-intervention (% correct) | Post-intervention (% correct) |
| SBA Q1 | 37.5 | 100.0 |
| SBA Q2 | 25.0 | 100.0 |
| SBA Q3 | 12.5 | 100.0 |
| SBA Q4 | 37.5 | 100.0 |
| SBA Q5 | 12.5 | 87.5 |
| SBA Q6 | 25.0 | 100.0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInnovations in Medical Education · Clinical Reasoning and Diagnostic Skills · Simulation-Based Education in Healthcare
Introduction
Clinical neurology is widely recognized as one of the more demanding areas of medicine. Students often describe how its reliance on precise anatomical localization, the complexity of neurophysiological concepts, and the habit of "lesion thinking" combine to form a cognitive barrier that erodes both confidence and competence [1,2]. The term neurophobia captures this cluster of anxieties and has been linked to avoidance behaviors and suboptimal learning outcomes across several countries [3-5].
At the same time, high-stakes assessments, such as the UK Medical Licensing Assessment (MLA), increasingly place an emphasis on vignette-based clinical reasoning and Single Best Answer (SBA) formats. These assessments reward the integration and application of knowledge rather than rote recall. However, the teaching students receive during neurology placements, particularly in district general hospitals, often remains fragmented and opportunistic, leaving them without the structured frameworks needed for success in both exams and early clinical practice [6,7].
Resident doctors play a significant role in bridging this gap. They are often best placed to translate complex neurological ideas into practical heuristics, though their capacity to provide structured teaching is frequently limited by clinical pressures [8]. Recognizing these systemic and pedagogical shortcomings, we registered a quality improvement project (QIP: 25-586) with our institutional QI office. Our Specific, Measurable, Achievable, Relevant, Time-bound (SMART) aim was precise, i.e., to increase the average self-assessed confidence score of medical students in neurology from 2.5/5.0 to 4.0/5.0 by May 1, 2025. This aim was implemented within the Model for Improvement framework, employing iterative plan-do-study-act (PDSA) cycles to refine both delivery and measurement.
The primary objective was to improve medical students’ self-rated confidence in neurology through an MLA-aligned, vignette-based session, and the secondary objective assessed in the second PDSA cycle was to evaluate objective knowledge gain using a six-item SBA test. By turning clinical reasoning into brief, case-based practice, the intervention sought to reduce neurophobia and better prepare students for both licensure assessments and day-to-day clinical work.
Materials and methods
This prospective quality improvement project was conducted between January and April 2025 at a district general hospital in the East of England. The study employed the Model for Improvement and two sequential plan-do-study-act (PDSA) cycles to iteratively develop and refine the intervention [8,9]. The project was registered with the East Suffolk and North Essex NHS Foundation Trust (ESNEFT) Quality Improvement Office (QIP: 25-586). As a service evaluation aimed at improving local educational delivery, the project was exempt from formal review by the UK NHS Health Research Authority’s Research Ethics Committee. All participants provided written informed consent for the anonymized use of their data for evaluation and publication. Data handling complied fully with General Data Protection Regulation (GDPR) standards.
Sixteen medical students on core clinical neurology placements were recruited across two consecutive eight-week blocks. The sample size was determined by placement cohort availability (opportunistic convenience sample). Each PDSA cycle included eight students. Participation was voluntary, and all invited students elected to take part, yielding a 100% paired response rate for all assessments.
The intervention was a 90-min, interactive, resident-facilitated teaching session supported by a purpose-designed 34-page booklet, Neurology for Medical Students. The booklet summarized high-yield concepts and included MLA-style vignettes with Single Best Answer (SBA) questions and fully explained answer rationales. Content selection prioritized syndromes and decision points relevant to routine clinical practice and MLA blueprint topics. Cycle 1 consisted of the initial booklet and facilitated session. Cycle 2 incorporated refinements based on participant feedback, including a portable clinical aid summarizing key neurological examination findings and a higher proportion of test-style questions to mirror examination conditions [10]. The full session outline and contents of the 34-page booklet are provided in appendix 1, and the pre- and post-session confidence and knowledge survey tools are provided in appendix 2.
The primary outcome was self-assessed confidence in neurology, recorded using a five-point Likert scale administered immediately before and after each session. The secondary outcome was objective knowledge, measured in both cycles using a six-item SBA test administered immediately pre- and post-session. The SBA items, authored by the lead investigator and reviewed by a consultant neurologist for content validity, were thematically aligned with the session but distinct from the worked examples in the booklet. An example item is provided to illustrate the question format and level of reasoning assessed. A 62-year-old woman presents with stiffness and weakness when climbing stairs. Examination reveals mild upper-arm weakness, hip flexion 4/5 bilaterally, quadriceps fasciculations, brisk ankle reflexes, and a positive Babinski sign. Sensory examination is normal. What is the most likely diagnosis? (A) Multiple sclerosis, (B) myositis, (C) diabetic neuropathy, (D) motor neuron disease, or (E) myasthenia gravis.
As the data were paired and not assumed to follow a normal distribution, Wilcoxon signed-rank tests were used to compare pre- and post-intervention scores. Effect sizes were reported as absolute values ( \begin{document}|r| = \frac{|Z|}{\sqrt{N}}\end{document} ) for interpretability. Statistical significance was defined as p<0.05. The internal consistency of the six-item SBA test was evaluated using Cronbach’s alpha, with α≥0.70 considered acceptable [11]. Analyses were performed using IBM SPSS Statistics version 28 (Chicago, IL: IBM Corp.).
Results
All 16 participants completed paired pre- and post-session measures. The intervention produced substantial and statistically significant improvements in confidence and objective knowledge, as detailed in Table 1. Item-level question performance and teaching content converted into question and answer (Q&A) format are presented in appendix 3 (table in appendix 3).
In cycle 1 (n=8), the median self-assessed confidence score (out of 5) increased from 2.5 (IQR: 2.0-3.0) to 4.0 (IQR: 4.0-4.25). This change was statistically significant (p<0.05) and associated with a large effect size (|r|=1.00). In cycle 2 (n=8), median confidence (out of 5) rose from 3.0 (IQR: 2.0-3.0) to 5.0 (IQR: 4.75-5.0) (p<0.01; |r|=0.89). These results are illustrated in Figure 1.
Change in medical student self-assessed confidence in neurology following the educational intervention.Median confidence scores (out of 5, with IQR error bars) for cycle 1 (n=8) and cycle 2 (n=8), before and after the session. Both increases were statistically significant.
Objective knowledge, measured in cycle 2 (n=8), increased from a mean SBA score of 25.0% (SD: 8.33) pre-session to 97.9% (SD: 5.5) post-session. This represented a highly significant improvement (p<0.01) with a large effect size (|r|=0.90). The six-item SBA instrument illustrated acceptable internal consistency (Cronbach's α=0.76). An item-by-item analysis demonstrated pre-session correct response rates ranging from 12.5% to 37.5%. Post-session, performance on five of the six items reached 100% correct, while the sixth item was answered correctly by 87.5% of participants (Table 2). These findings are illustrated in Figure 2.
Improvement in objective knowledge scores in cycle 2.Mean percentage scores (with SD error bars) on a six-item SBA test: pre-session 25.0% (SD: 8.33) vs. post-session 97.9% (SD: 5.5), p<0.01.SBA: Single Best Answer
Qualitative feedback from free-text surveys consistently emphasized the session's interactivity and strong alignment with examination practice. All the students reported that the SBA format encouraged active engagement and helped them understand the reasoning behind correct and incorrect answers, while the accompanying booklet served as a portable reference that reinforced key concepts. As outcomes were measured immediately post-session, the reported improvements represent short-term learning gains and should be interpreted as indicative of immediate efficacy rather than long-term retention.
Discussion
Brief, MLA-aligned vignette practice produced significant, immediate gains in both confidence and objective knowledge among medical students. Given the pilot design and immediate post-testing, these data should be interpreted as proof of concept that warrants controlled, multisite evaluation.
Neurophobia persists because neurology uniquely obliges learners to synthesize complex anatomy, physiology, and clinical signs into localization-based reasoning [1,2]. In district general hospitals, teaching is often opportunistic rather than organized, and resident doctors face competing clinical demands that limit consistent instruction [7,8]. Our intervention operationalized lesion-based and syndromic reasoning utilizing MLA-style vignettes that facilitated stepwise localization and differential prioritization. This use of context-rich problems aligns with established principles for the promotion of clinical reasoning skills in trainees [12]. This alignment likely explains the rapid translation into objective test performance, as learners practiced the exact cognitive tasks that the assessments evaluate.
Addressing neurophobia is a matter of patient safety and workforce preparedness. For a resident doctor, failing to recognize a hemiparetic stroke at the door of the emergency department is not a theoretical risk but a daily hazard. Similarly, hesitation in identifying a first seizure or an acutely raised intracranial pressure can carry profound consequences for patient outcomes. Gaps in neurology confidence, therefore, contribute not only to delayed recognition of emergencies but also to avoidance of neurology as a career choice at a time when the specialty faces workforce shortages [3-5]. By aligning teaching activities with assessment requirements - a principle known as constructive alignment - this intervention practises the reasoning skills required by both the MLA and safe clinical practice [13,14]. From a cognitive load theory perspective, the booklet reduced extraneous cognitive demands by consolidating concepts, while the SBAs provided structured, deliberate practice [15]. These educational principles likely contributed to the large effect sizes we observed. The small-group format enabled personalized feedback and open discussion, which may have amplified the effect [16].
This pragmatic model pairs near-peer facilitation with standardized, portable materials that are inexpensive to reproduce and can be scaled by running parallel small groups or embedding the booklet in curricula. The intervention's advantages over resource-intensive alternatives are notable, as high-fidelity simulation requires infrastructure and staffing commitments that many institutions will have difficulty sustaining [17].
This study’s limitations must be acknowledged. The sample size was small and from a single center, limiting generalizability. Knowledge was assessed immediately post-intervention, by design, to capture the direct educational impact of a single exposure; however, this approach does not evaluate long-term retention - a critical determinant of durable learning, as single-session gains often decay without reinforcement or retrieval practice [18,19]. The absence of a control group means that a testing effect cannot be ruled out, although the magnitude of improvement suggests this is an incomplete explanation [20]. In addition, volunteer bias may have influenced the results, as students with a pre-existing interest in neurology might have been more engaged. The possibility of partial overlap between teaching and testing content, as well as ceiling effects on the confidence scale, could also have inflated post-session scores. These limitations are common in early QI work, and this project therefore serves as a robust pilot demonstrating feasibility and effect magnitude [21-23].
The following steps include a cluster-randomized, multisite trial and delayed retention testing at 4-12 weeks to evaluate durability. Embedding the intervention into the formal curriculum would enable longitudinal evaluation of both educational outcomes and, eventually, impact on patient care, such as earlier recognition of neurological emergencies by resident doctors [24,25].
Conclusions
Neurophobia undermines medical education and patient safety, leaving students underconfident and ill-prepared for clinical practice. This pilot study demonstrates that a single, resident-led session, supported by a vignette-based booklet aligned to MLA SBA formats, can deliver large and statistically significant gains in both confidence and objective knowledge. Developed and refined using QI methodology, the intervention is compact, low-cost, and reproducible. Its alignment with national assessment standards positions it as a practical model for broader use. Future work should extend to multicenter evaluations and delayed retention testing to confirm its long-term impact and support formal curricular integration.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Is clinical neurology really so difficult?J Neurol Neurosurg Psychiatry Schon F Hart P Fernandez C 5575597220021197103310.1136/jnnp.72.5.557PMC 1737866 · doi ↗ · pubmed ↗
- 2Demystifying neurology: preventing “neurophobia” among medical students Nat Clin Pract Neurol Lim EC Seet RC 462463420081859450410.1038/ncpneuro 0849 · doi ↗ · pubmed ↗
- 3Neurophobia among medical students Neurosciences Lukas RV Albert DV 20201510.17712/nsj.2015.4.20150500 PMC 472764526492127 · doi ↗ · pubmed ↗
- 4National survey of UK medical students on the perception of neurology BMC Med Educ Pakpoor J Handel AE Disanto G 14201410.1186/1472-6920-14-225PMC 429533725335431 · doi ↗ · pubmed ↗
- 5Perception of neurology among undergraduate medical students - what can be done to counter neurophobia during clinical studies?BMC Med Educ JuknaŠ Puteikis K MameniškienėR 23202310.1186/s 12909-023-04405-y PMC 1027643337328733 · doi ↗ · pubmed ↗
- 6Reflecting reality: pager simulations in undergraduate education Clin Teach Dickinson M Pimblett M Hanson J Davis M 4214241120142521292510.1111/tct.12185 · doi ↗ · pubmed ↗
- 7Structure of neuroscience clerkships in medical schools and matching in neuromedicine Neurology Albert DV Yin H Amidei C 1721768520152607034210.1212/WNL.0000000000001731 · doi ↗ · pubmed ↗
- 8The role of residents in medical students’ neurology education: current status and future perspectives BMC Med Educ Keser Z Rodriguez YA Tremont J Hsieh PH Mc Cullough LD Sandrone S Stimming EF 1151102020203229942810.1186/s 12909-020-02036-1PMC 7164350 · doi ↗ · pubmed ↗