Digital Conversational Agents for the Mental Health of Treatment-Seeking Youth: Scoping Review
Lisa D Hawke, Jingyi Hou, Anh T P Nguyen, Thalia Phi, Jamie Gibson, Brian Ritchie, Gillian Strudwick, Terri Rodak, Louise Gallagher

TL;DR
This review explores how chatbots can help youth with mental health issues, finding they are generally accepted and may reduce depression symptoms.
Contribution
The study provides a scoping review of chatbots for youth mental health, emphasizing acceptability and design considerations.
Findings
Eight of ten studies reported high acceptability or positive user experiences with chatbots.
Three randomized controlled trials found potential reductions in depressive symptoms.
Literature on chatbots for youth mental health is emerging but limited, with no focus on substance use alone.
Abstract
Digital conversational agents (or “chatbots”) that can generate human-like conversations have recently been adapted as a means of administering mental health interventions. However, their development for youth seeking mental health services requires further investigation. This youth-engaged scoping review synthesizes the recent research on digital conversational agents for youth seeking mental health or substance use services. Studies were included if they were published between 2016 and 2025 and examined digital conversational agents for youth aged 11 to 24 years with mental health or substance use challenges in clinical settings. Systematic literature searches were conducted in February 2024 in multiple databases and updated in March 2025. Data were extracted using codeveloped forms and synthesized narratively. Ten studies were included, all focusing on mental health. Seven…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
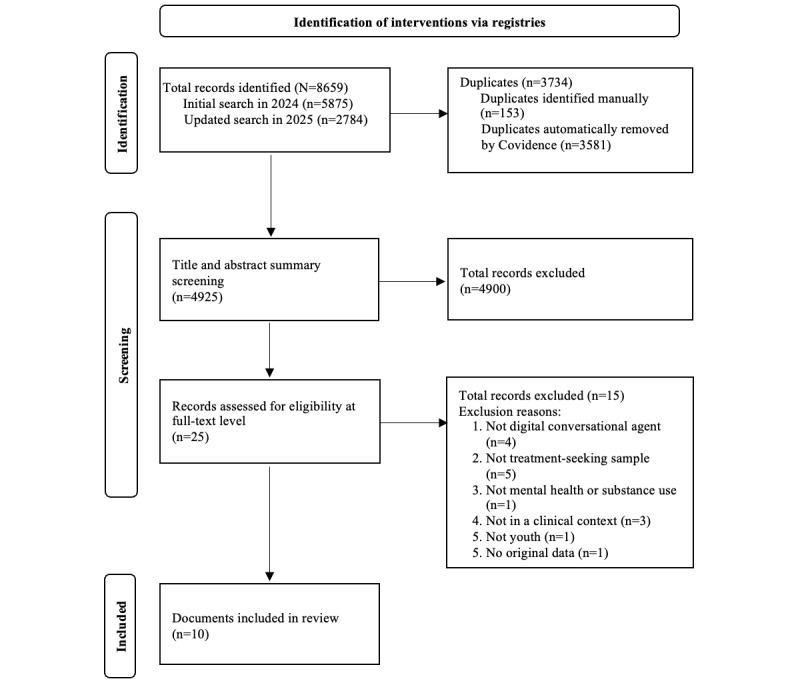 Figure 1
Figure 1| Author (year) | Country | Format | Technology described | Digital conversational agent objective | Intervention modality | Expressed digital conversational agent limitations | Codevelopment with youth |
| Wrightson-Hester et al [ | Australia | Web application | Artificial intelligence conversational agent | Help youth manage mental health using curious questioning | Method of levels therapy | Repetitive content and input comprehension issues | Yes |
| Greenwood et al [ | United States | Mobile app | Natural language processing and machine learning | Help youth develop emotion regulation skills | CBT, IPT-Ab, and DBTc | Effectiveness not rigorously tested for; not implemented in clinical practice | Not specified |
| Beilharz et al [ | Australia | Web-based chat accessible on mobile and desktop devices | Artificial intelligence conversational agent | Provide support for body image issues and eating disorders | Psychoeducation, coping skills via CBT, | Limited to psychoeducation and simultaneous coping skills | Yes |
| Fitzpatrick et al [ | United States | Instant messenger app on mobile or desktop | Decision tree methodology with predefined responses, including natural language processing at certain points within the tree | Deliver self-help CBT to young adults with anxiety and depression symptoms. | CBT | Potential risk of violating psychotherapeutic processes related to limitations in conversational abilities | Not specified |
| Robinson et al [ | United States | Mobile app | Not specified | Deliver CBT to adolescents at adolescent outpatient mental health clinic. | CBT | Not specified | Not specified |
| Mahmud and Porntrakoon [ | Thailand | Not specified | AId-generated or DCAe mental health | No specific digital conversational agent introduced | Not specified | Lack of customization, depersonalization, algorithm bias, privacy concerns | N/Af |
| Kuhlmeier et al [ | Germany | Mobile apps and web platforms | Text-based conversational agent prototype | Provide youth and young adults personalized therapy for depression | CBT, IPTg | Currently an early-stage prototype | Yes |
| Kuhlmeier et al [ | Germany | Prototype accessed via laptop | Text-based conversational agent prototype | Support youth with depression through a behavioral activation exercise | Behavioral activation | Currently an early-stage prototype | No, but participant feedback will influence the future design |
| Hasei et al [ | Japan | Accessible via mobile app LINE | GPT-4 large language model | Help pediatric, youth, and young adult cancer patient reduce anxiety and stress | Not specified | 4-turn conversations | Not specified |
| Li et al [ | Hong Kong | Accessible via Microsoft Teams | An interactive conversational system with natural language understanding | Support university students with self-reported depression through MBSRh | MBSR interventions | Technical issues with Microsoft Teams, required high self-discipline, limited interactivity | Not specified |
| Author (year) | Study | Sample size | Sample age (years) | Mental health or substance use conditions | Exclusion | Measurement | Amount of use of digital conversational agent within study | Outcome summary |
| Wrightson-Hester et al [ | Assess feasibility and acceptability | 13 | 16-24 | Anxiety or depression | Severe depressive symptoms or frequent suicidal thoughts | Self-report measures of depression, anxiety, QoLa, related psychological constructs, and system usability and engagement | Week 1: 1-4 days, 1-3 chats/day (average length 2-30 min); Week 2: 1-7 days, 1-5 chats/day (average length 5-15 min) | Feasible assessments; acceptable system engagement; acceptable interface; acceptable therapeutic conversations; some frustration, but resolved through use; recommendations for improvement; possible improvements in some psychological measures |
| Greenwood et al [ | Establish the feasibility, preliminary acceptability, effectiveness, and usability | 18 (17 analyzed) | 13-17 | Depression and anxiety | Parent-reported history of severe depression, substance use, psychotic illness, OCDb, PTSDc, panic disorder, or specific phobias; psychiatric hospitalization in the previous month; unaccompanied by a guardian at diagnostic visit; no access to a mobile device for regular use; unable to read and write English. | Self-report measures of depression (primary outcome), anxiety, and self-efficacy; app usage rates; acceptability, feasibility, and usability; safety monitoring. | Average use of 6 days, 55 mood check-ins, 313.17 sent messages, 13.63 lessons, and 9 tools over 4 weeks | Acceptability and feasibility confirmed; decreased depression and anxiety; increased self-efficacy; satisfactory usage rates; acceptable safety monitoring. |
| Beilharz et al [ | Evaluate the acceptability and feasibility | 25 (17 youth, 8 caregivers) | Youth: 13-18; caregivers: 46-57 | Body image concerns or eating disorders | Not specified | Focus group guide | Not specified | Appealing character and design; preference for brief content with a conversational tone; acceptable flow via button-based navigation; preference for free-text option; appreciation of accessibility. |
| Fitzpatrick et al [ | Assess feasibility, acceptability, and preliminary efficacy | 70 | 18-28 | Anxiety and depression | Not specified | Self-report measures of depression, anxiety, affect, and acceptability and usability; open-ended questions; usage tracking | Up to 20 sessions, average 12.14 check-ins over 2 weeks | Feasibility confirmed; reduction in depression symptoms, but not anxiety or positive or negative affect; high engagement and satisfaction; some positive comments on process and content; some challenges with process, technology, and content; limitations existed. |
| Robinson et al [ | Explore the feasibility and noninferiority | 141 | 13-17 | Depression or anxiety | Not specified | Self-report measure of depression and anxiety | Not specified | Noninferiority to clinician-delivered CBTd-skills group in reducing depression symptoms. |
| Mahmud and Porntrakoon [ | Explore perspectives on DCAse as alternative treatments | 15 (10 youth, 5 psychologists) | Youth: 20-25 | Depression or anxiety | Not specified | Interview guide; self-report measures of depression and anxiety. | Not specified | Interest in using DCA when experiencing depression or anxiety; concerns about privacy, confidentiality, and security; preferences varied on the extent and time of expert assistance |
| Kuhlmeier et al [ | Design a | Problem awareness phase: 15 youth; evaluation phase: 5 experts, 5 potential users | Problem awareness phase: 14-17; evaluation phase: experts: mean 29; potential users: mean 24 | Depression | Not specified | Interview guide | Not specified | Personalization of the conversational agent and content is essential, combined with structure; areas of improvement identified |
| Kuhlmeier et al [ | Investigate how youth interact with the conversational agent for depression | 15 | 14-17 | Depression | Suicidal ideation, psychosis, or low cognitive functioning. | User interaction data and think-aloud sessions documenting thoughts about the DCA | 11:54-20:38 min | Engaging interaction style; preferences varied on emoji and language use; appreciation of predefined responses, optional reminders, and clear interface; varied perceptions of responding speed and the dialogue content |
| Hasei et al [ | Assess feasibility and potential impact in pediatric, youth, and young adult cancer patients | 5 | 13 to 20s | Not specified, but cancer patients usually experience anxiety and stress from cancer | Not specified | Self-report measure of anxiety and stress; open-ended questions. | Most used every 2-3 days for about 10-15 min/session over 1-2 weeks | Reduced anxiety and stress; possible increased cancer treatment engagement; possible increased self-expression and informal help-seeking. |
| Li et al [ | Evaluate feasibility, acceptability, safety, and preliminary efficacy | 30 (27 completed) | 18-25 | Depression | Diagnosed with a clinical psychotic condition preintervention or were currently involved in any mindfulness-based or other psychosocial interventions. | Self-report measure of depression, stress, anxiety, and mindfulness; open-ended questions. | 8 weeks; encouraged at least 1 hour of daily interaction. | Feasibility, acceptability, safety, and preliminary efficacy confirmed; limitations identified. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDigital Mental Health Interventions · Social Robot Interaction and HRI · Mental Health via Writing
Introduction
Background
Digital conversational agents, or “chatbots,” are tools that can simulate a human interaction in text format, using artificial intelligence to respond intelligently to user inputs. They may use human-generated algorithms to produce conversations, or natural language processing to recognize and respond to inputs with a programmed personality. Digital conversational agents have been used in mental health for tasks such as providing psychoeducation, building coping skills, delivering cognitive-behavioral therapy, and providing diagnostic support [1-4].
There is emerging research available on digital conversational agents for mental health or substance use in treatment-seeking populations such as youth who are seeking or accessing services to support their mental health or substance use. A recent set of 2 reviews found minimal research on digital conversational agents for mental illness, with a specific gap around youth, and the studies were not necessarily in treatment-seeking populations [3,4]. They did find some acceptability and positive effects for the tool’s ability to establish diagnosis, but less so among youth. Some positive mental health impacts were found, but study limitations made these difficult to determine. Digital conversational agents in the psychiatric sphere have targeted various outcomes. For example, one was designed to promote activity engagement among individuals with severe mental illness [5]. Others have been designed to promote service utilization [6], develop mindfulness and emotion regulation [7], determine diagnoses [8], or promote medication adherence [9]. Evidence of the development of something akin to a therapeutic alliance has been demonstrated [10], while the responses of digital conversational agents have been rated as higher quality and more empathetic than physician responses [11]. However, the research evidence for treatment-seeking youth in clinical contexts (ie, receiving treatment) remains limited and has yet to be synthesized.
There is more research on the use of digital conversational agents as a prevention, promotion, or low-threshold mental health support tool, particularly for youth in school settings [12-15]. An acceptability study found that youth preferred to receive information through a digital conversational agent versus searching for it online, while the “personality” of the digital conversational agent was appreciated for its friendly, relational aspects [12]; the practical advice and referrals offered were also appreciated. Advantages include flexibility, accessibility, the capacity to reach more youth faster than in-person services, cost-effectiveness, and the ability to get help without stigma [12,13,15]. However, evidence on efficacy remains limited [16], and the need to empirically test these interventions has been highlighted [12,15,17].
As digital conversational agents expand around the world, a number of ethical issues have been raised. One team set out recommendations for minimal ethical standards in the use of digital conversational agents for youth mental health [17]. Some factors include ensuring confidentiality, being transparent about uses and limits, generating appropriate crisis responses, and protecting against addictive use. The article further highlighted the importance of testing efficacy, being transparent with users about the evidence base, encouraging in-person services, and explaining that these tools are not designed to treat severe mental illness. For vulnerable youth in treatment-seeking contexts, privacy and confidentiality is important, and addictive use might be a particular concern. These concerns have been reflected in discussions of the promise and necessary cautions regarding the implementation of digital conversational agents [18,19]. These issues must be attended to in the development, testing, and scale of digital conversational agents for mental health.
Youth are high users of digital technology [20] and often use digital means of seeking information about health [21]. They may be interested in receiving support through digital conversational agent technology. However, treatment-seeking youth with potentially complex mental health challenges have different needs and may have different preferences than school-based samples. Given ethical concerns about digital conversational agents for severe mental illness [17], further exploratory work is an essential prerequisite to digital conversational agent development. It is important to gain the perspectives of treatment-seeking youth around the possible utility, functionality, acceptability, and safety of digital conversational agents to address mental health challenges among them. It is also important to continue to do up-to-date work in this area, given the fast pace of technology development that leaves older research quickly out of date.
Objective
This scoping review aims to synthesize the recent literature on digital conversational agents for youth in clinical contexts seeking treatment for mental health or substance use challenges.
Methods
Overview
We used the scoping review methodology given the breadth and nature of the research and the exploratory nature of the research question in an emerging field, using established scoping review processes [22,23]. The scoping review incorporated the following major steps: (1) defining the research question, (2) identifying relevant studies, (3) screening and selecting studies, (4) extracting the data, and (5) summarizing the data and reporting. PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews) guidelines have been followed in the reporting of this review (Multimedia Appendix 1) [24].
Youth Engagement
In accordance with the strategy for patient-oriented research [25], we engaged 2 youth engagement specialists with lived experience in the conduct of this review. We endorsed pragmatism as a fundamental worldview and valued youth contributions, as per lived experience engagement paradigms [26]. Youth engagement specialists helped identify keywords for the systematic search, coselected information to extract from the resulting studies, and assisted with interpreting and reporting on the findings. Collaboration with the youth engagement specialists helped guard against bias and ensured that the study was relevant to the real-world experiences of young people, enhancing rigor.
Defining the Research Question
This scoping review aims to understand the published academic literature on digital conversational agents for treatment-seeking youth with mental health or substance use challenges, in clinical contexts. Based on the PICO (population, intervention, comparison and outcomes) framework [27], this review focuses on youth with mental health or substance use challenges (population) and applications of digital conversational agents in treatment-seeking in clinical settings (intervention). Note that the treatment-seeking and clinical settings context was a key inclusion criterion that makes this review very specific to clinical contexts, which is a gap in the literature. It includes studies with or without comparison groups and reports on the full range of findings, regarding applications, acceptability, and outcomes related to digital conversational agents for the target population, as well as other findings highlighted in the selected literature. Literature on preventive interventions and nonclinical settings was excluded.
Identifying Relevant Studies
A comprehensive search strategy was developed with a health sciences librarian (TR). Considering the subject areas of the research question, the search was developed, tested, and finalized in Medline, then translated and run on February 22, 2024 in the following bibliographic databases: APA PsycInfo, Medline, Embase, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Web of Science, Applied Social Sciences Index and Abstracts (ASSIA), and Cochrane Central Register of Controlled Trials (CENTRAL). The search was repeated and updated on March 18, 2025. The search strategies used database-specific subject headings and keywords in natural language, as well as advanced search operators such as truncation and adjacency operators, to capture 3 main concepts: youth, digital conversational agent, and mental health or substance use. The review was limited to articles published in the past 8 years (2016-2025) due to the rapid advancement of AI technology. There were no limitations placed on language or study type. Conference abstracts were removed through the search strategy when allowed by a database, but were otherwise included. A supplementary hand search of reference lists and Google Scholar was conducted. Given the nature of the research question, the gray literature search was limited to dissertations in APA PsycInfo, registered clinical trials in the CENTRAL search, and nontraditional publications indexed in CINAHL.
Study Screening and Selection
To be included, articles had to present descriptive information or research results on digital conversational agents for youth mental health or substance use, focusing on treatment-seeking populations in clinical contexts. Articles could report on any study design and sample size and could include descriptive process papers. The digital agent and study had to be focused on youth approximately aged 11-24 years, or separate analyses had to be available for a subgroup within this age range. Articles had to be published in English or French consistent with the language skills available on the team, although no non-English language texts were found. We included any outcomes identified by the article in question, including acceptability and feasibility outcomes as well as mental health or substance use outcomes of any kind or intensity. Excluded were any studies not reporting on digital conversational agents for youth mental health or substance use, research conducted on children (majority aged younger than 11 years) or adults (majority aged older than 24 years), and commentaries that did not describe either research results or a specific digital conversational agent. Textbox 1 presents inclusion and exclusion criteria, which were developed to optimize the ability to address the research question. Selected articles were screened first at the title and abstract level by 2 of 3 research staff (include or exclude responses), with any conflicts resolved through discussion with the project lead. The resulting set of articles were screened in full using the same process. Article screening was conducted using Covidence software [28].
Inclusion and exclusion criteria for literature search.Inclusion criteria
- Addresses digital conversational agents
- Agent designed for youth aged 11-24 years
- Participants with mental health or substance use challenges (disorders or symptoms)
- Participants seeking mental health or substance use treatment (ie, connected with clinical contexts)
- Published between 2016 and 2025
- Reports on efficacy, effectiveness, feasibility, or acceptability
- Reports on youth perspectives using youth-reported data (any method) Exclusion criteria
- Not a youth-focused agent and study
- Prevention or promotion that does not support known mental health or substance use challenges
- Youth were not treatment-seeking or were not exposed to the digital conversational agent in a clinical context
- Published before 2016
- Papers without original data
Data Extraction
A data extraction form was developed collaboratively among team members, including youth. From the final selected articles, data were extracted by 1 staff member and verified by a second staff member using a spreadsheet. The data extraction form included (1) study general information (eg, reference, location, and data collection years), (2) digital conversational agent description (eg, goal or objective, application and content, context of use, development and testing, youth engagement, software and data strategy, feedback learning integration, delivery method, financial investment, privacy, content monitoring, and sustainability plan), (3) study methods (eg, study objective, design, sampling method, sample size, sample description, exclusion criteria, measures, and other treatments), (4) outcomes (eg, finding overview, youth perspectives, digital conversational agent benefits and limitations, adverse events, and study limitations), (eg, 5) ethical issues (privacy and confidentiality, efficacy, safety, and mitigating strategies), and (eg, 6) other information (author conclusions and recommendations).
Data Summarization and Reporting
The data were summarized narratively and in table format. Quality assessment was not conducted, as this is not a priority in scoping reviews in which a wide range of diverse research is mapped.
Ethical Considerations
Since this is a scoping review of the literature, ethics board approval was not required. There are no human participants in this article and informed consent is not required.
Results
Study Selection
Our search identified 8659 records, including 5875 records from the initial search in 2024 and 2784 from the updated search in 2025. After removing 3734 duplicates, we screened 4925 titles and abstracts, excluding 4900. We further assessed 25 full-text articles. Fifteen were excluded due to not meeting our inclusion criteria, which resulted in 10 studies included in the review. The study selection process is illustrated in the PRISMA flow diagram (Figure 1).
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart.
Table 1 summarizes the included articles and digital conversational agents studied. The 10 studies examined 9 digital conversational agents for youth mental health in clinical care contexts. Studies emerged from the United States [2,29,30], Germany [31,32], Australia [1,33], Thailand [34], Japan [35], and Hong Kong [36], with publication years ranging from 2017 to 2025. Only 3 articles stipulated that the digital conversational agents were co-designed with youth [1,31,33].
Study Characteristics
Of the 10 included studies, 7 assessed feasibility or usability or the preliminary efficacy or effectiveness [1,2,29,33,35,36], while others investigated perceptions of using the agent [34], perceptions of their design [31], and youth’s interaction experience with them [32]. Three studies used qualitative methods [1,31,32], 1 used quantitative methods [30], and 6 used mixed methods [2,29,33-36]. Three studies used randomized controlled trials to evaluate 2 digital conversational agents [2,29,30]. Participant demographics varied in the studies, covering age groups from adolescents to young adults with depression [31,32,36], anxiety or depression [2,29,30,33,34], anxiety and stress [35], and eating disorders [1]. None focused on substance use disorders. Some studies also included mental health professionals [31,34] and caregivers [1] as participants.
Intervention Characteristics
The technology driving the digital conversational agent was not always specified but included artificial intelligence, for example natural language processing, machine learning, and decision trees. While publications were dated 2016 to 2025, the year of the development of the digital conversational agent under examination was not reported. The interventions were delivered via a mobile app [2,29-31,35,36] or a computer browser [1,31-33]. Treatment modalities included cognitive behavioral therapy or components thereof [1,2,29-32]; an integration of cognitive behavioral therapy, interpersonal psychotherapy, and dialectical behavior therapy [29]; a method-of-levels approach [33]; mindfulness-based stress reduction interventions [36]; and unspecified modalities [34,35]. Some studies included screenshots or sample interactions to illustrate the digital conversational agent’s responses [1,31-33,35]. For example, one study shows a screenshot of coping skill recommendations made by the chatbot [1]. Another shows a screenshot of behavioral activation recommendations [32]. However, others did not provide details about the exact nature of the responses of the digital conversational agent. The digital conversational agents were not generally described as being integrated into a system of care to accompany clinical services, except for one that was designed for young cancer patients [35].
Qualitative and Acceptability Findings
The methodology and outcomes of the included articles are summarized in Table 2. Most studies reported that the digital conversational agents were acceptable to youth, with high utilization [2,29], high satisfaction [2], and overall positive perceptions [1,2,31-33]. Participants appreciated the ease of use [33], appealing and accessible design [1,32], and friendly characters [1,32]. They also found that the content was helpful and appropriate [1,2,35], equipped them with new mental health insight [2], and offered them empathy [2,32]. Youth identified advantages, namely the neutrality, anonymity, and availability of these tools compared to traditional psychotherapy [31,35,36]; some youth indicated their willingness to use digital conversational agents for depression and anxiety, with cautions regarding privacy and security [34].
A number of problems, challenges, or barriers were identified by participants across the studies. These included limited natural conversation [2,33,35], limited customization [1,31,33,34], technical glitches [2,36], and concerns regarding the quality of the therapeutic interventions [1,31,34]
Quantitative Findings
Six studies provided quantitative results on the digital conversational agents’ ability to improve participants’ mental health. A randomized controlled trial (RCT) of a digital conversational agent called Woebot found that, compared to a self-help e-book, the intervention significantly reduced depressive symptoms after 2 weeks, with a moderate effect size (d=0.44) [2]. In another RCT, 4 weeks of using Woebot was found to be noninferior to a standard clinician-led CBT group in reducing depression when comparing pre-post average scores and the number of participants with elevated depression; the effect size was not provided [30]. In a pilot RCT, the treatment group showed greater mean improvement in depression than the waitlist control group (d=0.98) [29]. No significance testing was reported for these trials [29,30]. A single arm study found a large effect size (d=1.26) for reducing problem-related distress and a medium effect size (d=–0.66) for improving goal conflict reorganization among participants with anxiety or depression [33]. Additionally, a single arm pretest-posttest study of a digital conversational agent delivering a mindfulness intervention reported significant and large improvements in depression, anxiety, stress, and mindfulness levels, with large effect sizes across all outcomes, at d=–1.95 for stress, d =–1.53 for depression, and d=–1.09 for anxiety [36].
Ethical and Safety Considerations
The minimal ethical standards proposed for digital conversational agents revolve around (1) privacy and confidentiality, (2) efficacy, and (3) safety [17]. One study encompassed these requirements by providing user participants with an information package regarding privacy, efficacy, and safety issues as part of the application onboarding process [29]. Another study emphasized rigorous approval and safety measures that include anonymized and secure data handling and adherence to the Declaration of Helsinki [35]. However, most of the included articles did not discuss ethical issues in depth. While concerns over privacy and confidentiality were mentioned by many youths and stakeholders [29,31,33,34], only half of the articles included any information on their privacy policies. A case series assessing feasibility and acceptability for depression or anxiety reported that secure user identification and anonymized data collection was not conducted within the study, but would be implemented in the future [33]. One study informed participants that they would not be monitored by a counsellor [1], while another disclosed that a psychologist would monitor participants’ activities asynchronously [2].
Despite the ethical importance of ensuring efficacy, most of the articles described pilot trials examining acceptability and feasibility without adequate power to determine efficacy. Prominent limitations were small sample sizes and the lack of diversity. As a result, while many of the interventions were reportedly inspired by evidence-based therapeutic approaches [1,2,29,33,36], the delivery of the interventions via these tools has not been demonstrated efficacious or effective in real-world settings and thus requires further evaluation.
Safety issues are also worthy of note. Only 6 of the selected studies described safety features [1,2,29,33,35,36]. Among these, 3 reported that participants were informed of about the tool and given explanation of its function and capacities [1,2,29]. Only 1 study mentioned having a crisis response measure, in which the digital conversational agent could identify concerning language and confirm it with users [29]. One study emphasized that their safety measures include automated escalation systems for distress detection and professional involvement during development and testing [35]. Another study involved continuous monitoring by mental health professionals, weekly participants check-ins, and mental health support resources and referral pathways [36]. The digital conversational agents featured in these 4 trials offered additional mental health resources and provided easily accessible channels to connect users with suicide helplines or emergency services.
Discussion
Principal Findings
This review synthesized the recent literature on digital conversational agents for youth with mental health or substance use conditions, specifically in treatment-seeking clinical contexts. It was found that the literature is quite preliminary and is focused entirely on mental health, not substance use conditions. Yet, this is an emerging area of work that is a high priority to some research teams and health care organizations. Several of the digital conversational agents reviewed applied the principles of cognitive behavioral therapy, but this was not universal. Promising findings were identified in terms of feasibility and acceptability, together with reasonable usage rates and positive youth perspectives of acceptability. Preliminary findings suggested that digital conversational agents might be an acceptable means of delivering therapeutic content to treatment-seeking youth, with positive impacts on their mental health.
The literature was largely made up of feasibility and acceptability studies rather than efficacy trials. The digital conversational agents were not described as being embedded in intervention contexts, such as being integrated with in-person clinical care. Sample sizes were small and diversity was limited. People with different sociodemographic profiles and different clinical needs might be differentially interested in using e-health innovations [38,39], although differences across population subgroups have not been definitively established. This leaves the evidence base in a very premature state. For example, there is a lack of exploration of the impact the tools might have as an integrated component of youth mental health care among diverse youth.
All of the articles addressed mental health; none addressed substance use. It is important to consider mental health and substance use together, given the high levels of overlap and increasing trends toward treating concurrent disorders together [40]. Examining digital conversational agents for substance use challenges, or for concurrent mental health and substance use challenges, is a pressing area for future work. Investigations into suitability using different treatment modalities for specific diagnostic groups might also be worthy of consideration, given that specific symptoms may interact with whether and how one might use such a tool (eg, low motivation, paranoia, suicidal ideation, and mood instability).
This review focused on very recent literature on digital conversational agents, given the fast pace of technology. However, any article published in 2016 was likely examining a digital conversational agent developed at the latest in 2015, potentially earlier. These tools were not leveraging today’s latest technology, and the technology used was not thoroughly described. The rapid pace of technology advancement is not a new challenge, but rather one that the health care sector has been grappling with for years [41]. This leaves two problems: (1) the technology is already out of date by the time the research is complete, and (2) the evidence base that a new study leverages is out of date and may no longer be relevant by the time it is used. Ongoing rapid research and publication in this area is essential, with thorough descriptions of the technology underpinning the tool, including the year of tool development to help readers understand the state of technological advancement of the digital conversational agent in question.
In digital intervention development, co-design with the end users is critical [42]. This can be done using appropriate patient engagement frameworks [43]. Co-design helps ensure that the digital tool is appropriate for the end users and relevant to their needs. However, multiple articles reviewed did not discuss co-design, which may reduce acceptability. Future digital design teams should adhere to patient engagement principles for e-health innovation [43] as well as youth engagement principles [44]. Co-design has the potential to be a meaningful opportunity for young people to gain experience in technology development and clinical research, supporting their personal and professional growth and development [45]. In conducting co-design, teams should incorporate principles of equity, diversity, inclusion and accessibility to ensure that a diverse range of voices are included, to generate a digital conversational agent that is appropriate for a wide range of diverse youth, and to mitigate the harms that can come from biases, discrimination, and inequities. Specifically, a lack of diversity at the co-design stage could perpetuate algorithmic bias, which should be guarded against. Engagement can also be leveraged to increase digital literacy and the use of resulting tools, potentially with the support of digital navigators [46].
From our review, it was clear that the minimum ethical standards for digital conversational agents were not adequately attended to [17]. Few studies reported directly on privacy, confidentiality, and safety, and efficacy has not been definitively established. We call on developers and trialists to directly attend to the proposed ethical standards in their initiatives, proactively integrate these minimum standards into their technology and trials, integrate an ethical review stage into their initiative, and report clearly on the use of these standards. The ethics of delivering evidence-based intervention modalities via digital conversational agents should be considered—and when which modality is appropriate and for whom—since a clinician may naturally adapt their services to the individual youth, while digital tools may function differently using artificial intelligence in attempt to do the same. Matching the tool’s aim to the youth’s need, ensuring youth can withdraw at any time, and offering access to a person to talk to would all further enhance tools’ ethics and should be considered by interventionists. It should be transparent that a digital conversational agent can supplement clinical care but is not a replacement for it; integrating tools into clinical care rather than leaving them as stand-alone tools might address this challenge [47].
The use of digital conversational agents is not without risk. A recent news story highlights a case of youth suicide after the youth’s ongoing interaction with a digital conversational agent [48]. It should be noted that youth are using digital conversational agents for mental health support even if these agents are not designed for that purpose. By developing a digital conversational agent with and for youth, with the explicit purpose of supporting mental health in appropriate ways using evidence-based content, it may be possible to provide young people with a safer tool and prevent such tragedies from occurring.
While some articles discussed soliciting youth feedback as part of a study, none discussed collecting youth feedback within the digital platform. Providing opportunities to submit feedback within the platform is a potential mechanism to enable continuous improvement and incremental alignment with the needs and preferences of the users. The feedback could be directed to programming teams for programming feedback, and potentially separately to clinical teams to support clinical care as part of an integrated treatment plan. It would be important to determine means to balance the importance of privacy and confidentiality [17] with the potential for identified clinical support.
The next steps in this line of work would be to address some of the limitations, such as co-design and ethical concerns, with the ultimate goal of moving forward to full-scale trials to examine efficacy. This would have to be followed by implementation and ongoing refinement. The evaluation of complex interventions is expected to begin with iterative stages of intervention development, feasibility testing, evaluation, and implementation [49,50], and the research for this type of intervention is in the early stages of this process.
Limitations
Strengths and limitations of this review should be kept in mind. Important partners were engaged in the review, including industry partners and youth with lived experience. These partnerships ensured that the search terms, data extraction, and interpretations are relevant to the artificial intelligence industry and youth. However, readers should note the methodological and scope limitations: the search included only an 8-year period to ensure that the findings are as relevant as possible to recent technology, but may have missed early findings. We excluded any articles focusing on prevention or promotion, which may have relevant findings. Any publications indexed after March 2025 were not captured. The search was run only in English-based databases.
Conclusions
Emerging but preliminary literature is examining digital conversational agents for treatment-seeking youth with mental health conditions, but not substance use challenges. Digital technology already exists and will inevitably expand, making it essential that we support its expansion with rigorous research. This research must therefore continue, with attention to establishing efficacy, as well as ensuring appropriate protection of privacy and confidentiality and attention to safety and ethical concerns. While digital technology comes with challenges, it also comes with potential benefits. Co-design with youth, for youth, should be a priority. Nevertheless, promising early research justifies continuing this work with the possibility of codeveloping safe, accessible, youth-friendly, and potentially efficacious tools for youth mental health.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Beilharz F Sukunesan S Rossell SL Kulkarni J Sharp G Development of a positive body image chatbot (KIT) with young people and parents/carers: qualitative focus group study J Med Internet Res 20210616236 e 27807 10.2196/2780734132644 v 23i 6e 2780734132644 PMC 8277317 · doi ↗ · pubmed ↗
- 2Fitzpatrick KK Darcy A Vierhile M Delivering cognitive behavior therapy to young adults with symptoms of depression and anxiety using a fully automated conversational agent (Woebot): a randomized controlled trial JMIR Ment Health 2017060642 e 19 10.2196/mental.778528588005 v 4i 2e 1928588005 PMC 5478797 · doi ↗ · pubmed ↗
- 3Vaidyam AN Linggonegoro D Torous J Changes to the psychiatric chatbot landscape: a systematic review of conversational agents in serious mental illness: changements du paysage psychiatrique des chatbots: une revue systématique des agents conversationnels dans la maladie mentale sérieuse Can J Psychiatry 202104664339348 10.1177/07067437209664293306352633063526 PMC 8172347 · doi ↗ · pubmed ↗
- 4Vaidyam AN Wisniewski H Halamka JD Kashavan MS Torous JB Chatbots and conversational agents in mental health: a review of the psychiatric landscape Can J Psychiatry 201907647456464 10.1177/07067437198289773089795730897957 PMC 6610568 · doi ↗ · pubmed ↗
- 5Liu HT Development of a chatbot to promote activity participation for people with serious mental illness University of Alberta [dissertation]20212025-09-24University of Alberta https://ualberta.scholaris.ca/items/dacf 408d-89af-453c-bb 51-f 146e 62d 3af 8
- 6Shah J De Pietro BD'Adamo L Firebaugh M Laing O Fowler LA Smolar L Sadeh-Sharvit S Taylor CB Wilfley DE Fitzsimmons-Craft EE Development and usability testing of a chatbot to promote mental health services use among individuals with eating disorders following screening Int J Eat Disord 20220955912291244 10.1002/eat.237983605664836056648 PMC 10053367 · doi ↗ · pubmed ↗
- 7Denecke K Vaaheesan S Arulnathan AA mental health chatbot for regulating emotions (SERMO) - concept and usability test IEEE Trans Emerg Topics Comput 202171931170118210.1109/tetc.2020.2974478 · doi ↗
- 8Philip P Micoulaud-Franchi J Sagaspe P Sevin ED Olive J Bioulac S Sauteraud A Virtual human as a new diagnostic tool, a proof of concept study in the field of major depressive disorders Sci Rep 20170216742656 10.1038/srep 4265628205601 srep 4265628205601 PMC 5311989 · doi ↗ · pubmed ↗