Cephalosporin allergy: R1 side-chain and penicillin cross-reactivity patterns in an Australian cohort
Brittany Stevenson, Elizabeth Klinken, Michelle Trevenen, Jack Bourke, Patricia Martinez, Michaela Lucas

TL;DR
This study examines cross-reactivity patterns between cephalosporin and penicillin allergies in an Australian cohort, finding that R1 side-chain groups largely explain these reactions.
Contribution
The study provides new data on cross-reactivity patterns in cephalosporin-allergic patients with and without penicillin allergy history.
Findings
R1 side-chain groups explained most skin testing and provocation challenge outcomes.
Most patients with penicillin allergy labels tolerated penicillin challenges and were delabeled.
Some positive penicillin skin tests occurred in patients without prior penicillin allergy history.
Abstract
Cross-reactivity between cephalosporins, and penicillins, is mainly explained by R1 side-chain similarity. However, data on cross-reactivity patterns in cephalosporin-allergic patients, with and without preexisting penicillin allergy labels, are lacking. We sought to determine whether R1 side-chain groups account for cross-reactivity between cephalosporins, and penicillins with similar R groups, in a cohort of patients with cephalosporin allergy labels, with and without a penicillin allergy history. A retrospective audit (February 2016 to November 2021) of adult outpatients with cephalosporin allergy labels, who underwent skin prick / intradermal testing and/or oral provocation challenges, was performed at 2 Australian tertiary hospitals. We identified 212 patients with a single cephalosporin allergy label; 97 had coexisting penicillin allergy labels. Fifty-eight (27.4%) patients…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
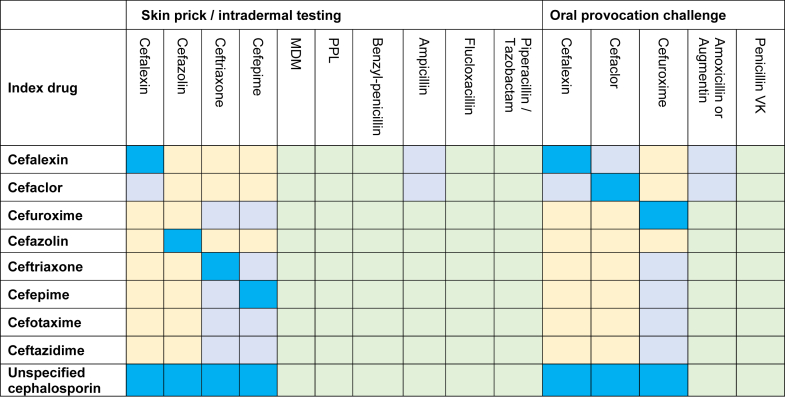 Figure 1
Figure 1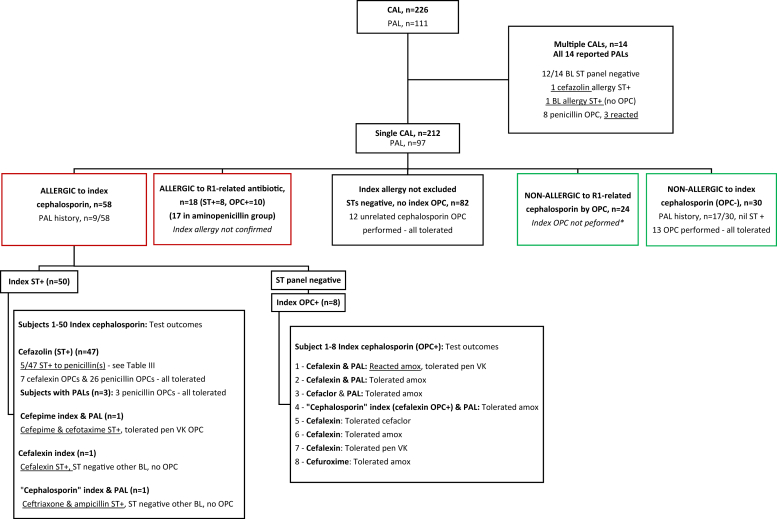 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDrug-Induced Adverse Reactions · Contact Dermatitis and Allergies · Antimicrobial Resistance in Staphylococcus
Introduction
Cephalosporins are commonly implicated in drug hypersensitivity reactions.1, 2, 3, 4 In Australia and the United States, 0.8% to 6.9% of patients report a cephalosporin allergy label (CAL) and cefazolin is the most frequently implicated antibiotic in perioperative anaphylaxis.1^,^2^,^5 Contemporary evidence has established the cephalosporin R1 side-chain as the dominant antigen explaining most cross-reactivities within cephalosporins, and with penicillins.6^,^7 This raises the question as to whether beta-lactam (BL) cross-reactivities exist outside R1 side-chain groups. Data on this issue are sparse. Most studies on cephalosporin allergies have excluded subjects with multiple cephalosporin and/or penicillin allergies; thus, these cannot comprehensively address this question.7^,^8
A retrospective audit of adult subjects (≥16 years) with a CAL, including subjects with a coexisting penicillin allergy label (PAL) or multiple CALs, was conducted at 2 tertiary Western Australian drug hypersensitivity clinics between February 2016 and November 2021. During this study period, BL skin testing (ST) was available only at these 2 tertiary clinics. The morphology and chronology of the index reaction was assessed by a clinical immunologist, and subjects with definite non–IgE-mediated reactions, and subjects who declined testing, were excluded. Allergic reactions were graded according to the World Allergy Organization (WAO) Systemic Allergic Reaction Grading System, which, unlike other grading systems, classifies hypotension as grade 4.9 Subjects underwent ST with nonirritant skin prick and intradermal test concentrations with a panel of BLs, based on recommended ST concentration ranges in Australasian Society of Clinical Immunology and Allergy and other guidelines10^,^11 (Table I). Cephalosporin ST concentrations (1-2 mg/mL) were chosen from the suggested ST concentration ranges, based on local experience. Oral provocation challenges (OPCs) were performed as 2- or 3-dose graded challenges with a penicillin and/or cephalosporin selected by the drug allergy specialist. Intravenous challenges were not performed. Study aims were to (1) compare cephalosporin cross-/co-reactivity with predicted R1 side-chain patterns and (2) assess whether the R1 side-chain model was applicable in patients with PALs. Cephalosporins and aminopenicillins were categorized by R1 side-chain similarity on the basis of previous evidence (Fig 1).12 Approval was granted, with waiver of consent, by the relevant ethics boards (GEKO#40051 and GEKO#40317).Table ISkin prick and intradermal test concentrationsSkin prick test PPL6.0 × 10^-5^ mol/L MDM1.5 × 10^-3^ mol/L Benzylpenicillin10,000 U/mL Amoxicillin20 mg/mLIntradermal test Cefazolin1 mg/mL Ceftriaxone1 mg/mL Cefalexin∗2 mg/mL Cefepime1 mg/mL PPL6.0 × 10^-5^ mol/L MDM1.5 × 10^-3^ mol/L Benzylpenicillin1,000 U/mL, 10,000 U/mL Amoxicillin20 mg/mL Ampicillin∗20 mg/mL Flucloxacillin†2 mg/mL Piperacillin/tazobactam†4.5 mg/mLThe BL panel was used for all subjects, with the exception of cefalexin, ampicillin, and piperacillin/tazobactam. MDM and PPL manufactured by Diater Laboratorio de Diagnostico, Madrid, Spain.MDM, Minor determinant mixture; PPL, penicilloyl polylysine.∗Cefalexin test, and ampicillin intradermal test, was available for testing at only 1 hospital.†Flucloxacillin was not always included, depending on clinician preference. Piperacillin/tazobactam was included if implicated in the index reaction.Fig 1BL skin test and OPC antibiotics were categorized according to their R1 side-chain similarity. Bright blue, testing with index drug; pale blue, testing within the R1 side-chain group; yellow, testing with an unrelated cephalosporin; green, testing with an unrelated penicillin. Antibiotics with a similar, but nonidentical R1 side-chain have been grouped, that is, cefalexin and cefaclor with amoxycillin (similar R1 side-chain) and cefuroxime with cefepime, cefotaxime, ceftriaxone, and ceftazidime (nonidentical R1 side-chain, but some evidence of clinical cross-reactivity). MDM, Minor determinant mixture; PPL, penicilloyl polylysine.
Results and discussion
Data were collected from 226 patient records: 212 subjects had a single CAL and 14 subjects had multiple CALs. Of the 212 subjects, 164 (77.4%) were female, mean age 50.5 years (range, 15-89 years). Implicated cephalosporins were cefalexin (n = 94 [44.3%]), cefazolin (n = 73 [34.4%]), ceftriaxone (n = 14 [6.6%]), cefaclor (n = 12 [5.7%]), cefepime (n = 7 [3.3%]), cefuroxime (n = 2 [0.9%]), cefotaxime (n = 1 [0.5%]), cetazidime (n = 1 [0.5%]), and “unspecified cephalosporin” (n = 8 [3.8%]). The grade of index reaction was mild (WAO grade 1-2) in 91 (42.0%) subjects, anaphylaxis (WAO grade 3-4) in 120 subjects (56.7%), and unknown in 1 (0.5%) subject. Time to testing was less than 1 year since index reaction in 86 (40.6%) subjects, 1 to 5 years in 55 (25.9%) subjects, and more than 5 years in 9 (4.3%) subjects. PALs were documented in 97 (45.8%) subjects, being most common with index reactions to cefalexin and cefaclor (62 of 106 [58.5%]).
Testing outcomes for the whole cohort are summarized in Fig 2. Overall, 58 (27.4%) subjects were confirmed allergic to the index cephalosporin by ST (n = 50) or OPC (n = 8). Forty-seven (81.0%) of the 58 subjects had an index reaction to cefazolin confirmed by ST, and 50 (86.2%) subjects had anaphylaxis as the index reaction (most due to intraoperative anaphylaxis). Nine (15.5%) of these 58 subjects had a previous PAL.Fig 2. Skin prick / intradermal test and OPC outcomes for all subjects with CALs. Test outcomes relating to PALs are also summarized. Amox, Amoxicillin. ∗ST result negative, index OPC not performed for clinical or logistical reasons, noting intravenous challenges are not routinely performed.
Multivariate logistic regression analysis was performed to assess predictors of positive ST results. Subjects with a history of anaphylaxis as the index reaction, or an intravenous culprit cephalosporin, were significantly more likely to have a positive ST result to the culprit or an R1 side-chain–related cephalosporin (index reaction anaphylaxis vs nonanaphylaxis: odds ratio, 6.05, 95% CI, 2.51-14.6, P < .0001; intravenous vs oral culprit cephalosporin: odds ratio, 9.68, 95% CI, 4.23-22.2, P < .0001) (Table II).Table IIUnivariate and multivariate logistic regression results comparing patient and index characteristics with ST result (event = positive index or R1 side-chain ST) and OPC (event = reacted to index or R1 side-chain OPC)CharacteristicSTOPCUnivariateMultivariateUnivariateMultivariateOR (95% CI)P valueOR (95% CI)P valueOR (95% CI)P valueOR (95% CI)P valueAge For a 10-y increase0.90 (0.76- 1.06).1861Not significant1.13 (0.81- 1.56).4837Not significantSex Male vs Female2.22 (1.10- 4.48).0257Not significant1.29 (0.29- 5.71).7411Not significantGrade 3/4 vs 1/2/Unknown6.69 (2.95- 15.2)<.00016.05 (2.51- 14.6)<.00011.11 (0.35- 3.49).8644Not significantTiming Intermediate vs Remote/Unknown1.13 (0.42- 3.06).0005Not significant1.43 (0.37- 5.46).8444Not significant Recent vs Remote/Unknown3.88 (1.74- 8.65)1.37 (0.33- 5.75)Culprit route Intravenous vs Oral10.4 (4.71- 23.1)<.00019.68 (4.23- 22.2)<.00011.47 (0.12- 17.4).7612Not significantCulprit group Single CAL only vs single CAL + PAL4.70 (2.25- 9.85)<.0001Not significant0.59 (0.18- 1.98).3932Not significant“Cephalosporin not specified” culprits excluded. No variables (age, sex, severity/timing of index reaction, drug route, presence of PAL) were statistically related to index or R1 side-chain OPC outcomes.
All 58 subjects with confirmed CALs underwent ST with a panel of BLs, followed by OPCs selected with the aim of safely broadening future BL options (Fig 2). R1 side-chain cross-reactivity was assessed in 11 subjects, excluding 47 subjects with cefazolin allergy due to its unique R1 side-chain. ST from 1 subject demonstrated R1 side-chain cephalosporin cross-reactivity (cefepime culprit and cefotaxime ST+). Six of the 11 subjects underwent an OPC with an R1-related antibiotic (all aminopenicillins), of which only 1 subject (cefalexin culprit) reacted with urticaria during an amoxicillin OPC.
We next assessed cross-reactivity for unrelated R1 side-chain cephalosporins. All 58 subjects had negative ST results to unrelated R1 side-chain cephalosporins. Seven subjects underwent an OPC with an unrelated cephalosporin, and all were tolerated.
Finally, we looked for examples of cross-/co-reactivity to penicillins or broad BL reactivity, excluding R1 side-chain–related penicillins (ie, aminopenicillins with aminocephalosporins). We compared patients with and without preexisting PALs. Of the 9 subjects with a preexisting PAL, 1 had a positive ST result to a penicillin (intradermal test cefazolin 7 mm, ampicillin 5 mm) and was not challenged; the other 8 subjects in fact tolerated a penicillin OPC and were delabelled. Thus, most (7 of 8 tested [87.5%]) of the subjects with confirmed CALs had their preexisting PAL removed. However, of the 49 subjects without any preexisting PAL, 5 subjects (10.2%) had positive ST results to penicillin(s), including 1 subject who demonstrated broad BL ST reactivity to cephalosporins and penicillins (Table III). All 5 subjects had a history of anaphylaxis to cefazolin. One cefazolin-allergic patient with a positive ampicillin ST result in fact tolerated a penicillin VK OPC; the other 4 were not challenged. To date, 27 of the 44 subjects with negative penicillin ST results have undergone a penicillin OPC and, as expected, all were tolerated.Table IIIPositive ST/IDT results demonstrating non-R1 side-chain BL cross-/co-reactivity among subjects with confirmed index cephalosporin allergies, and no preexisting penicillin allergySubjectIndex culprit drug (index reaction)Preexisting PALPositive ST/IDT resultsOPC1Cefazolin (grade 4 reaction; <1 y earlier)NilCefazolin +++, benzylpenicillin ++, ampicillin +++Not performed2Cefazolin (grade 4 reaction; timing unknown)NilCefazolin ++, benpenzylpenicillin +, amoxicillin ++, ampicillin +Not performed3Cefazolin (grade 4 reaction 1-5 y earlier)NilCefazolin +++, ampicillin +++Tolerated penicillin VK4Cefazolin (grade 4 reaction; >5 y earlier)NilCefazolin +++, amoxicillin +++Not performed5Cefazolin (grade 3 reaction; <1 y earlier)NilCefazolin,∗ MDM ++, PPL +, benpenzylpenicillin ++, amoxicillin +, ampicillin +, cefalexin +, ceftriaxone +, cefepime +Not performedThe ST result was considered positive if the wheal diameter was at least 3 mm larger than that achieved with the negative control with surrounding erythema (flare). The IDT result was considered positive if the wheal diameter was at least 3 mm greater, and erythema was at least 5 mm greater, than that achieved with the control wheal (saline bleb). Wheal size summarized as 3 mm +, 4-7 mm ++, ≥ 8 mm +++.IDT, Intradermal test; MDM, minor determinant mixture; PPL, penicilloyl polylysine.∗Cefazolin IDT performed in anesthetics drug allergy clinic, documented clear positive; however, wheal/flare size not documented.
In the remaining cohort, another 18 (8.5%) subjects were confirmed allergic to an R1-related antibiotic (aminopenicillins in 17 of 18) where a true index CAL was clinically suspected but not definitively confirmed. Thirty (14.2%) subjects were proven nonallergic to the index cephalosporin by OPC. Seventeen of these 30 subjects had PALs; however, none were confirmed by testing.
There were 14 subjects who reported multiple CALs (5 involving R1-related cephalosporins, 9 involving R1-unrelated cephalosporins) and all 14 also reported PALs. One CAL was confirmed (cefazolin ST+), and another subject had positive ST result to multiple BLs, suggesting a possible BL ring allergy. Eight of the 14 subjects underwent a penicillin OPC, of which 3 (37.5%) subjects reacted—none of whom had confirmed CALs.
This study presents a real-world analysis of test outcomes in cephalosporin- allergic subjects. We found that 27% of patients had their cephalosporin allergy confirmed, and that a history of anaphylaxis during the index reaction and an intravenous culprit drug were statistically significant predictors of a positive index or R1-related cephalosporin ST result. This finding is consistent with previous literature.8^,^13
Our major finding is that subjects with a confirmed cephalosporin allergy may demonstrate cross-reactivity within the R1 side-chain groups, but there was no evidence of broader cephalosporin group cross-reactivity.7^,^14 This finding reinforces the clinical relevance of the R1 side-chain model in cephalosporin allergy. The R1 side-chain model was similarly relevant to subjects with preexisting PALs, including examples where aminopenicillin/aminocephalosporin R1 side-chain cross-reactivity was confirmed, but a broader penicillin allergy was refuted.
It is well established that around 90% of patients with PALs (without CALs) can be delabelled after drug allergy assessment.15^,^16 Similarly, in our study, most subjects with preexisting PALs in fact tolerated a penicillin challenge, regardless of whether they had a true CAL. A notable exception was the higher penicillin OPC reaction rate in the 14 subjects with 3 or more BL allergy labels: 1 demonstrated broad BL ST positivity, and 3 of 8 reacted to a penicillin OPC. This finding suggests that clinicians should exercise more caution in assessing patients with multiple BL allergy labels, such as by avoiding direct challenges, without preceding skin tests.
The unexpected finding in this study was the penicillin ST reactivity observed in 5 (10.2%) of the confirmed cefazolin-allergic subjects. We note, however, that there were no examples of penicillin allergy demonstrated by OPC in the cephalosporin-allergic patients without PALs. Four of the 5 cefazolin and penicillin ST-positive subjects did not undergo a follow-up penicillin challenge due to safety concerns and lack of clinical indication. Our findings are similar to those of previous reports, including a meta-analysis reporting that 3.7% to 4.4% of cefazolin-allergic patients have positive ST results to penicillins.7^,^8^,^17 However, a recent study highlighted instances of false-positive penicillin ST results in cefazolin-allergic patients, reporting that 5 of 68 (7.3%) subjects with positive cefazolin ST results also had positive penicillin ST results, but in fact went on to tolerate a penicillin challenge.18 The ST results in our cohort of cefazolin-allergic patients demonstrated significant wheal and flare, with multiple positive ST results in 3 cases, making false-positive results less likely. Ultimately, without follow-up penicillin challenges, it is not possible to determine whether these penicillin ST results represent false positives, true cross-reactivity, or cosensitization to penicillins.
The limitations of this study are the retrospective data collection, incomplete testing and inconclusive test outcomes in a number of cases, limited number of subjects with confirmed allergies to noncefazolin cephalosporins, and lack of confirmatory challenges in subjects with positive ST results. We acknowledge that some of the intradermal skin test concentrations used in this study differ from those used in some other centers; however, ST concentrations used were contemporary to guidelines available at the time this study commenced. Repeat testing to assess for resensitization following negative drug allergy workup was not performed, given lack of global consensus for this approach, and resource constraints.10^,^19
Conclusion
Cross-reactivity between cephalosporins, and penicillins, is mainly explained by R1 side-chain similarity, with infrequent examples of broad BL cross-reactivity. However, some positive penicillin ST results do not clearly follow these patterns, and the presence or absence of a PAL does not reliably predict penicillin test results in cephalosporin-allergic patients. Future research investigating the safety of supervised graded penicillin challenges in cephalosporin-allergic patients is needed.Clinical implicationsCross-reactivity between cephalosporins, and penicillins, is mainly explained by R1 side-chain similarity, but some positive ST results do not follow this pattern. The presence of a preexisting PAL is not a good predictor of penicillin skin test or OPC outcomes in cephalosporin-allergic patients.
Disclosure statement
Disclosure of potential conflict of interest: The authors declare that they have no relevant conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Blumenthal K.G.Wolfson A.R.Li Y.Seguin C.M.Phadke N.A.Banerji A.Allergic reactions captured by voluntary reporting J Patient Saf 172021 e 1595 e 16043072054610.1097/PTS.0000000000000568 PMC 6669104 · doi ↗ · pubmed ↗
- 2Dhopeshwarkar N.Sheikh A.Doan R.Topaz M.Bates D.W.Blumenthal K.G.Drug-induced anaphylaxis documented in electronic health records J Allergy Clin Immunol Pract 720191031112996968610.1016/j.jaip.2018.06.010PMC 6311439 · doi ↗ · pubmed ↗
- 3Van Boeckel T.P.Gandra S.Ashok A.Caudron Q.Grenfell B.T.Levin S.A.Global antibiotic consumption 2000 to 2010: an analysis of national pharmaceutical sales data Lancet Infect Dis 1420147427502502243510.1016/S 1473-3099(14)70780-7 · doi ↗ · pubmed ↗
- 4Dutra K.J.Lazenby G.B.Goje O.Soper D.E.Cefazolin as the mainstay for antibiotic prophylaxis in patients with a penicillin allergy in obstetrics and gynecology Am J Obstet Gynecol 23120244304363852760710.1016/j.ajog.2024.03.019 · doi ↗ · pubmed ↗
- 5Toh T.S.Foo S.Y.Loh W.Chong K.W.En Goh A.Hee H.I.Perioperative anaphylaxis: a five-year review in a tertiary paediatric hospital Anaesth Intensive Care 49202144513347238510.1177/0310057 X 20964470 · doi ↗ · pubmed ↗
- 6Romano A.Valluzzi R.L.Caruso C.Maggioletti M.Quaratino D.Gaeta F.Cross-reactivity and tolerability of cephalosporins in patients with Ig E-mediated hypersensitivity to penicillins J Allergy Clin Immunol Pract 62018166216722940844010.1016/j.jaip.2018.01.020 · doi ↗ · pubmed ↗
- 7Stone C.A.Jr.Trubiano J.A.Phillips E.J.Testing strategies and predictors for evaluating immediate and delayed reactions to cephalosporins J Allergy Clin Immunol Pract 92021435444.e 133282291810.1016/j.jaip.2020.07.056PMC 7855229 · doi ↗ · pubmed ↗
- 8Touati N.Cardoso B.Delpuech M.Bazire R.El Kara N.Ouali D.Cephalosporin hypersensitivity: descriptive analysis, cross-reactivity, and risk factors J Allergy Clin Immunol Pract 9202119942000.e 53338559010.1016/j.jaip.2020.11.063 · doi ↗ · pubmed ↗