Exploring patient preferences regarding the use of combination therapy with endothelin receptor antagonist (ERA) + phosphodiesterase-5 inhibitors (PDE5i)
Nicholas A. Kolaitis, Martha Kingman, Melisa Wilson, Gabriela Gomez Rendon, David Lopez, Carly J. Paoli, Mohammad Rahman, Ashley Martin, November McGarvey, Abraham Lee, Sana Mirza, Lana Melendres-Groves

TL;DR
This study explores how patients with pulmonary arterial hypertension prefer combination therapies, finding that a single tablet could reduce pill burden and improve adherence.
Contribution
The novel contribution is identifying patient preferences for a single tablet combination therapy in PAH management.
Findings
83.1% of patients believed single tablet combination therapy would reduce pill consumption.
Out-of-pocket costs and dosing regimen were top factors influencing therapy choice.
STCT could improve treatment initiation and adherence, but cost remains a significant barrier.
Abstract
To evaluate patient preferences for endothelin receptor antagonist (ERA) + phosphodiesterase-5 inhibitor (PDE5i) combination therapies in managing pulmonary arterial hypertension (PAH), including the potential benefits of a single tablet combination therapy (STCT) in reducing pill burden and improving adherence. An online survey was administered to 201 adult patients with PAH residing in the United States. Patients' preferences toward oral PAH therapies, including willingness to use double combination ERA+PDE5i therapy, were assessed using a discrete choice experiment (DCE). Respondents were predominantly White (86.1%) and female (88.6%), with a median age of 59 years. Most were not employed (56.2%), and 38.3% reported a disability. At the time of the survey, 36.8% were on triple therapy (PDE5i + ERA + prostacyclin), 17.9% on dual therapy (PDE5i + ERA), and the remaining on other or…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
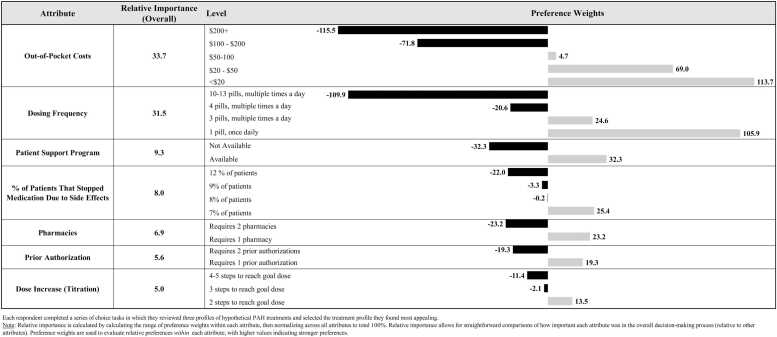 Figure 1
Figure 1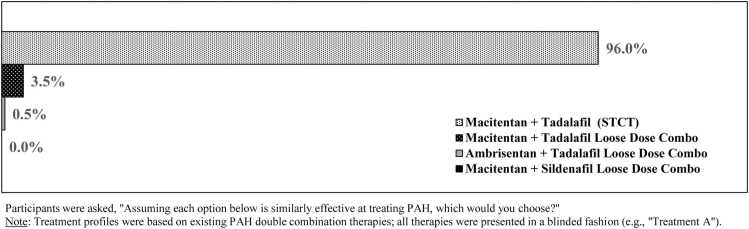 Figure 2
Figure 2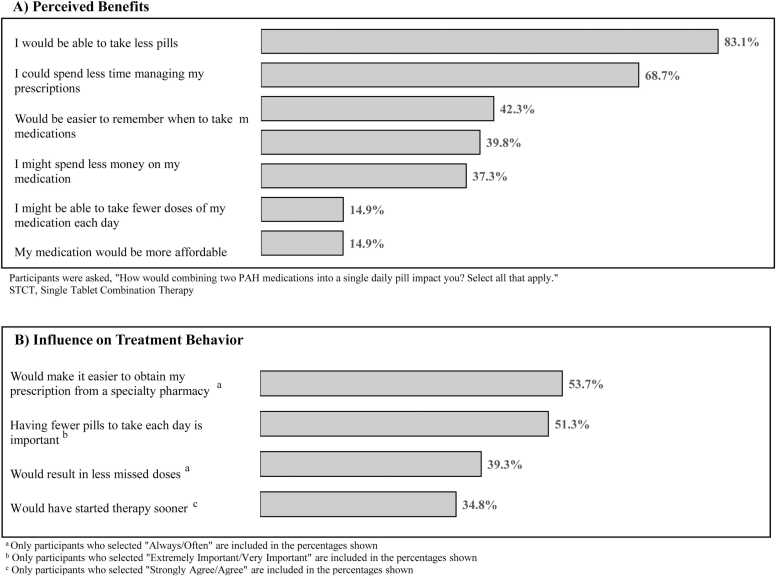 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBlood Pressure and Hypertension Studies · Pulmonary Hypertension Research and Treatments · Heart Failure Treatment and Management
Background
Pulmonary arterial hypertension (PAH) is a rare, progressive disease characterized by the proliferation and remodeling of the pulmonary vasculature.1 This pathological obstruction leads to elevated pulmonary vascular resistance and increased right ventricular afterload. As a result, the heart's capacity to function as a hemodynamic pump is impaired, reducing its ability to deliver sufficient oxygen to the body at the rate required for normal metabolizing tissue.2 Symptoms include chest pain, dyspnea, fatigue, and functional impairment, which worsen gradually. In addition to diminishing health-related quality of life, this physiological maladaptation of the heart eventually leads to right ventricular failure, high health care resource utilization, and premature death.2, 3, 4
The US Food and Drug Administration (FDA) has authorized a range of treatments for PAH via 4 distinct pathways. Although upfront combination therapy is considered the standard of care in PAH management due to its superior clinical outcomes, monotherapy remains widely used despite extensive evidence supporting the benefits of combination treatments.5, 6, 7, 8 Indeed, the proceedings of the 7th World Symposium on Pulmonary Hypertension recommend that all newly diagnosed Group 1 patients with PAH be started on upfront combination therapy with a phosphodiesterase-5 inhibitor (PDE5i) and an endothelin receptor antagonist (ERA), given the improved observed outcomes.4 However, the complexity of PAH treatment regimens poses significant challenges. Patients often require medications with diverse routes of administration. PAH therapies can be oral, inhaled, continuous infusion, or via subcutaneous injection. These medications also require frequent dosing schedules in addition to other concurrent therapies to manage comorbidities. Over 80% of patients with PAH take 5 or more medications, contributing to polypharmacy and reduced adherence.9 A separate US claims study indicated that patients with PAH take a mean (standard deviation) of 11.8 (8.2) tablets per day.10
Recently, the FDA approved a single tablet combination therapy (STCT), which combines the PDE5i tadalafil and ERA macitentan in a once daily tablet.11 In other fields of medicine, STCTs are considered an effective strategy for enhancing the accessibility and adherence to treatment.12 STCT can also lead to better disease control in other cardiovascular diseases, such as hypertension, dyslipidemia, and diabetes.13, 14, 15, 16, 17, 18, 19
Although STCT in PAH is now available, the current scientific literature is largely missing the patients’ perspectives in the context of these emerging treatment options. We sought to identify the key drivers guiding the patients’ choice of PDE5i + ERA combination therapy, and to assess their receptivity to utilize a STCT formulation.
Methods
Study design
An online survey was administered to a US sample of patients with PAH to assess their beliefs and attitudes around the adoption of double combination ERA + PDE5i therapy for managing their PAH. The survey evaluated patients’ (1) demographics and health characteristics, (2) opinions regarding STCT, and (3) treatment attributes driving their decision to select ERA + PDE5i using a discrete choice experiment (DCE). All content was designed, evaluated, and pilot tested by a panel of 3 independent PAH practitioners to ensure content validity and real-world relevance. The study was reviewed and granted exemption by the Western Institutional Review Board-Copernicus Group. Participant recruitment and outreach activities were managed by the Pulmonary Hypertension Association Registry (PHAR).
Participant population
Participants were sourced from PHAR, the largest active longitudinal registry in the United States that tracks patients with PAH who are new to care at a designated Pulmonary Hypertension Association Care Center.20 Registrants were emailed by PHAR staff alerting them to the availability of an optional research opportunity, and the first 201 who met eligibility criteria and completed the online survey were included in the analysis. No identifiable data were collected as part of the survey and the survey results were not linked back to the PHAR dataset.
Eligible participants were aged 18+, diagnosed with PAH, and had used at least 1 of the following PAH medications for 3 continuous months within the past year: Ambrisentan, Bosentan, Macitentan, Sildenafil, Tadalafil, Selexipag, Riociguat, Treprostinil, Epoprostenol, or Iloprost. Participants were ineligible if they self-reported any diagnosis of chronic thromboembolic pulmonary hypertension, interstitial lung disease, and/or diastolic heart failure. All participants were required to be able to speak, read, and understand English. Data were collected between August and September 2023.
Data collection
Participant demographics and health characteristics
Participant demographics (e.g., age, sex) and health characteristics (e.g., comorbidities, current treatments) were assessed via self-reported questionnaire items.
Treatment factors influencing ERA + PDE5i adoption
A DCE was conducted to evaluate which treatment factors were most important in determining patients’ willingness to adopt guideline–recommended double combination therapy. Each respondent completed a series of choice tasks in which they reviewed 3 profiles of hypothetical PAH treatments and selected the profile they found most appealing (Supplement S0.1). Each treatment profile presented a randomized combination of 7 different attributes, each with its own set of response options (“attribute levels”): (1) out-of-pocket costs, (2) dosing regimen, (3) percent of patients who discontinued medication due to side effects, (4) number of prior authorizations required, (5) number of pharmacies needed to visit, (6) number of dose increases (titration), and (7) patient support program (Supplement S0.2). One option/level for each of the 7 attributes was shown per profile, and the combinations of attributes were automatically selected based on an adaptive conjoint methodology.21 No 2 versions of the DCE were the same across respondents, minimizing the opportunity for bias.22 Key outcomes of the DCE included preference weights (or “part-worth utilities”), which were used to evaluate within-attribute treatment patterns, and relative importance estimates, which were used to evaluate between-attribute treatment patterns.
Perceptions of STCT for ERA + PDE5i adoption
After completion of the DCE, each respondent was shown 4 blinded ERA + PDE5i therapies and asked to select the 1 therapy they found most appealing (Supplement S0.3). Three of the blinded regimens were modeled off FDA-approved loose-tablet double combination therapies of ERA and PDE5i (macitentan-tadalafil, macitentan-sildenafil, and ambrisentan-tadalafil)6, 23, 24 and the fourth therapy was modeled off a STCT of macitentan-tadalafil.25 Each regimen displayed information on its dosing, discontinuation rates due to side effects, titration, number of pharmacies needed to visit, and number of prior authorizations required; these factors were selected from a panel of PAH practitioners as being relevant to treatment selection and important in determining the utility of STCT in this disease area. Due to individual differences in insurance coverage, an accurate out-of-pocket cost for each regimen could not be reliably presented; thus, we omitted cost as a feature in the blinded choice task. Separate questionnaire items further assessed respondents' attitudes and beliefs about STCT.
Sample size
A general rule for estimating sample sizes for a traditional choice-based conjoint analysis is 26, 27 In this formula, n = number of respondents, t = number of choice tasks, a = number of alternatives (profiles) per task, and c = largest number of levels for any one attribute. Our design yields a formula result of 1,206 with a sample size of 201, indicating sufficient sample size to generate relatively precise preference weights. We further implemented an adaptive choice-based conjoint design as it collects more data per participant than a traditional DCE and allows for greater stabilization of estimates in designs with smaller sample sizes.28
Statistical analysis
Data were analyzed using SAS Studio 3.81 (for descriptive statistics) and Sawtooth Software Lighthouse Studio 9.15.9 (for the DCE analysis). Preference weights were generated for each attribute level via hierarchical Bayesian estimation.29 These preference weights allow one to understand preferences within each attribute (i.e., how one attribute level is valued relative to its alternatives): higher weights indicate greater preference (or odds of being selected) whereas lower weights indicate lower preference or aversion. Relative importance estimates were also generated for each attribute by calculating the difference between the highest and lowest preference weights for each attribute (i.e., the most preferred vs least preferred levels), dividing by the sum of all attributes’ ranges, and multiplying by 100 to convert into a percentage. In contrast with preference weights, which are used for understanding within-attribute patterns, relative importance scores enable one to directly compare between attributes—with the largest values reflecting the most important factors driving patient decision-making. Descriptive statistics were used to summarize the aggregate sample (N = 201). Frequency counts and percentages were provided for categorical variables, whereas means and standard deviations were provided for continuous or discrete variables.
Results
Participant characteristics
Respondents were predominantly White (86.1%) and female (88.6%). The majority were not employed (56.2%), with over one-third reporting a disability (38.3%) and one-third reporting a World Health Organization Functional Class (WHO FC) III-IV disease (31.4%). Most had health insurance: 71.1% were covered by public insurance (of which 55.7% were Medicare), and 56.2% were covered by private insurance (Table 1).Table 1. Patient CharacteristicsTable 1All respondents (N = 201)N/Mean%/SDAge Mean (SD)57.613.9 Median (range)59.021-85Sex, n (%) Male2311.4% Female17888.6% Prefer not to answer0Ethnicity, n (%) Non-Hispanic18391.0% Hispanic168.0% Prefer not to answer21.0%Race, n (%)a White17386.1% Black or African American105.0% American Indian or Alaska Native0 Asian63.0% Native Hawaiian or other Pacific Islander10.5% Middle Eastern or North African0 Two or more races52.5% Prefer not to answer63.0%US region, n (%) West5627.9% Midwest4622.9% Northeast2713.4% South7235.8%Education, n (%) Some high school, no diploma31.5% High school graduate or equivalent2010.0% Some college, no degree4522.4% Associate’s degree3014.9% Bachelor’s degree6632.8% Post-bachelor’s degree3718.4% Prefer not to answer0Employment, n (%) Employed full-time3517.4% Self-employed115.5% Employed part-time147.0% Manage family/household2110.5% Not employed and looking for work31.5% Not employed and not looking for work (e.g., student, retired)3316.4% Not employed and unable to work (e.g., disability)7738.3% Prefer not to answer73.5%Insurance, n (%) Select all that apply Public Insurance14371.1% Medicare11255.7% Medicaid2813.9% VA31.5% Private Insurance11356.2% Other insurance94.5%Access to support systems, n (%) Select all that apply Professional care provider8743.3% Family caregiver6431.8% Patient organization assistance program6331.3% Patient support program6130.4% Vouchers and/or discount cards that reduce the cost of medication3718.4% Other3316.4% Government disability assistance2411.9%Caregiver, n (%) Select all that apply Spouse/partner11858.7% Professional care provider4622.9% Child(ren)3316.4% Other2914.4% Extended family2813.9% Neighbor42.0%Abbreviation: SD, standard deviation; VA, veteran's affairs.aRace recoded to exclusive categories.
Over one-third of respondents had access to support systems, including PAH professional care providers (43.3%), family caregivers (31.8%), and/or received support from patient assistance/support programs (31.3%-30.4%). Over half received caregiving support from their spouse/partner (58.7%). Vouchers and/or discount cards were used by 18.4% to reduce the cost of their medication.
On average, patients had been on their current PAH medication for 7.5 ± 6.1 years, which was typically double (17.9%) or triple (36.8%) therapy containing an ERA + PDE5i; the remainder were using monotherapy of ERA or PDE5i (26.4%) or soluble guanylate cyclase stimulators-based combination therapies (11%). Mean out-of-pocket costs averaged 20 per month (median, range = 0-1,100) (Table 2).Table 2. Patient Health and Treatment CharacteristicsTable 2All respondents (N = 201)N/Mean%/SDHealth conditions, n (%) Pulmonary arterial hypertension (WHO group 1)201100.0% Sleep apnea7939.3% Obesity4924.4% Depression4421.9% Thyroid disease3919.4% Anemia2813.9% Diabetes2010.0% Chronic kidney disease199.5% Systemic hypertension168.0% Cancer157.5% Chronic pain136.5% Chronic liver disease42.0% Peripheral vascular disease10.5%Current treatment, n (%) PDE5i (sildenafil or tadalafil) + ERA (bosentan, ambristan, or macitentan) + prostacyclin (selexipag, treprostinil, epoprostenol, or iloprost)7436.8% PDE5i (sildenafil or tadalafil) + ERA (bosentan, ambristan, or macitentan)3617.9% PDE5i alone (sildenafil or tadalafil)3115.4% ERA alone (bosentan, ambrisentan, or macitentan)2211.0% Other168.0% sGC (riociguat) + ERA (bosentan, ambrisentan, or macitentan) + prostacyclin (selexipag, treprostinil, epoprostenol, or iloprost)157.5% sGC (riociguat) + ERA (bosentan, ambrisentan, or macitentan)73.5%Current medication regimen duration, years Mean (SD)7.56.1 Median (range)6.30.25-37.1Time since diagnosis, yearsa Mean (SD)10.68 Median (range)91-38Time with provider, years Mean (SD)7.05.7 Median (range)60.08-28.8WHO functional class symptoms, n (%) Class I4220.9% Class II9647.7% Class III5828.9% Class IV52.5%Current regimen out-of-pocket cost, 5,000 and $7,000) were removed as being unlikely.
Treatment factors influencing ERA + PDE5i adoption
Relative importance estimates (S1.1) indicated that the most important factors (of those tested) influencing ERA + PDE5i adoption were lower out-of-pocket costs (33.7) and a simpler dosing regimen (31.5). Other factors such as patient support program (available vs not available = 9.3), discontinuation due to side effects (8.0), number of pharmacies required to obtain medications (1 vs 2 = 6.9), number of prior authorizations required (1 vs 2 = 5.6), and dose increase (titration) (5.0) were less important in determining treatment choices (Figure 1).Figure 1. Each respondent completed a series of choice tasks in which they reviewed 3 profiles of hypothetical PAH treatments and selected the treatment profile they found most appealing. Note: Relative importance is calculated by calculating the range of preference weights within each attribute, then normalizing across all attributes to total 100%. Relative importance allows for straightforward comparisons of how important each attribute was in the overall decision-making process (relative to other attributes). Preference weights are used to evaluate relative preferences within each attribute, with higher values indicating stronger preferences. PAH, pulmonary arterial hypertension.Figure 1
Individual preference weights (Figure 2) revealed that patients were most likely to select ERA + PDE5i treatment when out-of-pocket costs were under $20 (113.7), dosing regimen was 1 pill, once daily (105.9), patient support programs were available (32.3), discontinuation due to side effects was the least likely at 7% (25.4), the medications required 1 pharmacy (23.2), required 1 prior authorization (19.3), and only 2 steps were needed to reach goal dose (13.5) compared to 3 or 4 and 5 steps.Figure 2. Participants were asked, “Assuming each option below is similarly effective at treating PAH, which would you choose?” Note: Treatment profiles were based on existing PAH double combination therapies; all therapies were presented in a blinded fashion (e.g., “Treatment A”). PAH, pulmonary arterial hypertension; STCT, single tablet combination therapy.Figure 2
Further exploration confirmed that preferences for the lowest dosing regimen (single tablet therapy) and the lowest out-of-pocket cost (<$20) were maintained, despite patients’ current therapy (monotherapy vs double/triple therapy) or presumed financial status (inferred by their use of public only vs private/mixed insurance) (S1.3-S1.4).
Blinded choice of PAH therapies
When asked to select among blinded regimens mimicking the real-world characteristics of loose-dose ERA + PDE5i therapies, in addition to a hypothetical STCT, most respondents selected a profile resembling a STCT of macitentan-tadalafil (96.0%) (Figure 3).Figure 3(A) Participants were asked, “How would combining two PAH medications into a single daily pill impact you? Select all that apply.” (B) (a) Only participants who selected “Always/Often” are included in the percentages shown. (b) Only participants who selected “Extremely Important/Very Important” are included in the percentages shown. (c) Only participants who selected “Strongly Agree/Agree” are included in the percentages shown. STCT, single tablet combination therapy.Figure 3
Perceptions of STCT of ERA + PDE5i
Most respondents noted that STCT would allow them to take fewer pills per day (83.1%) and reduce time spent managing prescriptions (68.7%). Over one-third identified benefits to adherence (42.3%), cost (39.8%), and reduced pill burden (37.3%). Few expected their medications to be more affordable (14.9%) or associated STCT with increased treatment quality or confidence in physician-recommended medications (14.9%) (Figure 3A).
Likert scales indicated mixed evidence for whether an STCT would prove useful for compliance (Always/Often = 39.3%; Rarely/Never = 39.3%) and/or initiation of combination therapy (Strongly Agree/Agree = 34.8%; Disagree/Strongly Disagree = 30.8%). However, preferences for reduced pill burden (Always/Often = 51.3%) and easier prescription access (Always/Often = 53.7%) were upheld, consistent with the DCE and other self-report items (Figure 3B). The complete results can be found in the Appendix (S1.2a-c).
Discussion
This study examined the factors influencing patients with PAH’s decision-making regarding PDE5i + ERA therapy and their interest in STCT. Results of the DCE showed that patients were most receptive to combination therapies when offered with the lowest cost and least frequent dosing (i.e., lower pill burden). Cost slightly outweighed the convenience of single tablet dosing, aligning with findings from other chronic diseases such as diabetes and hypertension, where high out-of-pocket expenses reduce adherence.30 Participants were willing to trade off other benefits to reduce pill burden, which was 3 times as important as factors such as avoiding side effects or accessing support programs. Given that many participants had long-standing PAH and were already on combination therapy, concerns about side effects were minimal and factors such as titration and prior authorizations played a minor role in decision-making.
Most participants saw STCT as a promising solution for improving adherence by simplifying treatment regimens—a factor that is especially important in a population observed to take as many as 12 pills per day.12 This result is consistent with prior studies in other disease states showing that complex medication regimens contribute to reduced adherence and increased burden,33, 34, 35, 39 whereas simplified regimens—including STCT regimens12, 13, 14, 15, 16, 17, 18, 19—can lead to better disease control13, 14, 15, 16, 17, 18, 19 and lower health care resource utilization.36, 39 Our participants recognized this potential benefit, showing a strong preference for STCT in the DCE (when hypothetical treatment profiles were presented), as well as in the blinded choice task (when real-world treatment profiles were presented). In the latter case, 96% preferred a treatment simulating a STCT over multipill, “loose dose” alternatives (<4%).
Medication cost was a decisive factor, regardless of insurance type, with both publicly and privately insured patients favoring lower out-of-pocket expenses (S1.3). This is not surprising as most participants in this study had financial challenges such as unemployment and reliance on public insurance, which likely shaped their treatment preferences. Interestingly, while some participants additionally reported using vouchers or manufacturer support programs to manage costs, these programs were found largely unimportant to determining patient decision-making in the DCE. These findings highlight the need for clinicians to incorporate cost discussions into shared decision-making and to increase awareness of support programs that can help bridge financial barriers.
Although participants in this study strongly preferred simplified regimens such as STCT, they also prioritized minimizing out-of-pocket costs—2 preferences that are often at odds with one another. STCT typically comes at a higher price point due to their formulation complexity and branded status, presenting a financial barrier for patients who are already economically vulnerable. To reconcile this tension, strategies are needed to make STCT more affordable and accessible. These include expanded eligibility and awareness of manufacturer-sponsored copay and voucher programs, greater insurer coverage of STCT on preferred drug formularies, and value-based pricing models that account for long-term cost savings from improved adherence and reduced health care utilization. Additionally, policy efforts aimed at reducing cost-sharing burdens—particularly for publicly insured individuals—could help ensure that financial constraints do not prevent patients from choosing the therapies most likely to support sustained treatment success.
Limitations
The results of this study must be considered within the context of its limitations. Participants were a convenience sample of English-speaking US patients enrolled in the PHAR registry, which may limit generalizability to nonregistry populations and non-US settings. The sample was skewed toward White, insured women, and thus may not reflect the treatment priorities of uninsured and/or underinsured patients, especially those of minority groups that disproportionately experience issues with health care affordability and insurance access.37, 38 Over half of participants were not employed at the time of study, and this may reflect a sampling bias wherein unemployed adults are more likely to participate in online surveys. As a prevalent population, these patients had lived with their disease for some time, likely adjusting to their condition, which could result in different responses compared to those at the start of their treatment journey. While these sampling limitations may result in certain patients being omitted from the survey, the results nevertheless reflect valid preferences collected among WHO group 1 patients with PAH residing in the United States.
As with any DCE, the study results are bound by the attributes and levels included. To minimize respondent burden, fewer than 10 attributes were tested, and some important factors—such as clinical outcomes—were omitted. While the results observed here are valid within the choices provided to respondents, it is possible that decision-making would differ had respondents been shown a different selection of attributes and levels. Likewise, the blinded choice task—which omitted the cost of each regimen but included features such as dosing, discontinuation rates, and prior authorizations—may have yielded different results had a different combination of regimen characteristics been presented. Lastly, there is always some risk of inaccuracy in self-reported surveys; however, the structured nature of the DCE reduces the opportunity for distortions in memory by eliminating the need for open-ended recall, and the remaining questionnaire items represent low-stakes situations that are unlikely to evoke bad-faith answers.
Conclusions
Uptake of guideline–recommended upfront double therapy remains low in both the United States and globally, with monotherapy still commonly used in practice.8, 32 The results of this study suggest that dosing regimen (i.e., pill burden) is a critical factor influencing treatment selection among adults with PAH, and that STCT represents a way for patients to simplify their regimens and improve adherence. Whether STCT is effective in increasing adoption of guideline-recommended therapy and optimizing patient outcomes will ultimately depend on its affordability, as many patients face financial limitations and are strongly motivated to select the lowest-cost therapeutic option. While the upfront costs of combination therapy (including STCT) are likely to be offset in the long-term as a function of better disease management,3, 31 near-term solutions for reducing out-of-pocket costs are needed to ensure STCT remains an option available to patients.
Author contributions
Gabriela Gomez Rendon: Conceptualization, Methodology, Writing - review and editing. David Lopez: Conceptualization, Methodology, Writing - review and editing. Carly J. Paoli: Conceptualization, Methodology, Writing - review and editing. Mohammad Rahman: Methodology, Writing - review and editing. Abraham Lee: Data curation, Software, Formal analysis; November McGarvey: Conceptualization, Methodology, Supervision. Sana Mirza: Data curation, Formal analysis, Writing – original draft. Ashley Martin: Conceptualization, Methodology, Formal analysis, Writing – original draft. Nicholas A. Kolaitis: Conceptualization, Methodology, Writing - review and editing. Lana Melendres-Groves: Conceptualization, Methodology, Writing - review and editing. Melisa Wilson: Conceptualization, Methodology, Writing - review and editing. Martha Kingman: Conceptualization, Methodology, Writing - review and editing.
Funding
This study was sponsored by Johnson & Johnson Innovative Medicine, Titusville, NJ.
Declaration of Competing Interest
Nicholas A. Kolaitis reports administrative support, article publishing charges, statistical analysis, and writing assistance were provided by Janssen Pharmaceuticals Inc. Gabriela Gomez Rendon reports a relationship with Johnson & Johnson Innovative Medicine that includes employment and equity or stocks. David Lopez reports a relationship with Johnson & Johnson Innovative Medicine that includes employment and equity or stocks. Martha Kingman reports a relationship with Johnson & Johnson Innovative Medicine that includes consulting or advisory. Carly J. Paoli reports a relationship with Janssen Pharmaceuticals Inc that includes employment and equity or stocks. Mohammad Rahman reports a relationship with Janssen Pharmaceuticals Inc that includes employment and equity or stocks. Ashley Martin reports a relationship with BluePath Solutions Inc that includes employment. November McGarvey reports a relationship with BluePath Solutions Inc that includes employment. Abraham Lee reports a relationship with BluePath Solutions Inc that includes employment. Sana Mirza reports a relationship with BluePath Solutions Inc that includes employment. Nicholas Kolaitis reports a relationship with Johnson & Johnson Innovative Medicine that includes consulting or advisory. Johnson & Johnson Innovative Medicine reports a relationship with Melisa Wilson that includes consulting or advisory. Lana Melendez-Groves reports a relationship with Johnson & Johnson Innovative Medicine that includes consulting or advisory. G. Gomez, D. Lopez, C.J. Paoli, M. Rahman: Employees of Johnson & Johnson Innovative Medicine and hold stock in J&J. A. Lee, and N. McGarvey: Were employees of BluePath Solutions (BPS) at time of research but are no longer employed by BPS. N.A. Kolaitis: Has received financial support from J&J, Liquidia, United Therapeutics, Bayer. M. Wilson: Has received financial support from J&J, Merck, Bayer, United Therapeutics. M. Kingman: Has received financial support from Aerami, Merck, J&J, Liquidia, Gossamer. L. Melendres: Has received financial support from J&J, United Therapeutic, Bayer, Merck. The other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lan N.S.H.Massam B.D.Kulkarni S.S.Lang C.C.Pulmonary arterial hypertension: pathophysiology and treatment Diseases 620183810.3390/diseases 602003829772649 PMC 6023499 · doi ↗ · pubmed ↗
- 2Humbert M.Kovacs G.Hoeper M.M.2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: developed by the task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS). Endorsed by the International Society for Heart and Lung Transplantation (ISHLT) and the European Reference Network on rare respiratory diseases (ERN-LUNG)Eur Heart J 4320223618373110.1093/eurheartj/ehac 23736017548 · doi ↗ · pubmed ↗
- 3Pizzicato L.N.Nadipelli V.R.Governor S.Real-world treatment patterns, healthcare resource utilization, and cost among adults with pulmonary arterial hypertension in the United States Pulm Circ 122022 e 1209010.1002/pul 2.12090 PMC 924878635795495 · doi ↗ · pubmed ↗
- 4Chin K.M.Gaine S.P.Gerges C.Treatment algorithm for pulmonary arterial hypertension Eur Respir J 642024240132510.1183/13993003.01325-2024 PMC 1152534939209476 · doi ↗ · pubmed ↗
- 5Moutchia J.Mc Clelland R.L.Al-Naamani N.Pulmonary arterial hypertension treatment: an individual participant data network meta-analysis Eur Heart J 4520241937195210.1093/eurheartj/ehae 04938416633 PMC 11143388 · doi ↗ · pubmed ↗
- 6Sitbon O.Cottin V.Canuet M.Initial combination therapy of macitentan and tadalafil in pulmonary arterial hypertension Eur Respir J 562020200067310.1183/13993003.00673-2020 PMC 746997132350101 · doi ↗ · pubmed ↗
- 7Muller A.Escribano-Subias P.Fernandes C.C.Real-world management of patients with pulmonary arterial hypertension: insights from EXPOSURE Advances in Therapy 4120241103111910.1007/s 12325-023-02730-838216826 PMC 10879368 · doi ↗ · pubmed ↗
- 8Hoeper M.M.Pausch C.Grünig E.Temporal trends in pulmonary arterial hypertension: results from the COMPERA registry Eur Respir J 592022 Jun 210202410.1183/13993003.02024-2021 PMC 916039234675047 · doi ↗ · pubmed ↗