Postoperative changes of wrist-brachial index following arteriovenous fistula implantation correlate with steal syndrome, a prospective study
Navid Hajihoseini, Mohammadali Vakili, Alireza Aghili, Nazanin Musapour, Pezhman Kharazm

TL;DR
This study shows that changes in wrist-brachial index after AVF surgery can predict steal syndrome, including severe cases requiring treatment.
Contribution
The study demonstrates that immediate postoperative wrist-brachial index changes are a reliable predictor of steal syndrome after AVF implantation.
Findings
Immediate postoperative WBI changes significantly predict steal syndrome (P = .02) and severe cases (P = .03).
WBI changes correlated with hypertension and smoking but not other factors like age or diabetes.
23 patients had temporary steal syndrome, 16 had prolonged symptoms, and 3 required vascular reconstruction.
Abstract
Arteriovenous fistula (AVF) is the preferred vascular access for hemodialysis in end-stage renal disease. Steal syndrome, a complication causing limb ischemia, may follow AVF implantation. This study evaluated whether postoperative wrist-brachial index (WBI) changes predict steal syndrome, including severe cases requiring intervention. In a prospective study, patients undergoing first-time AVF implantation in 2022 were enrolled. WBI was measured preoperatively, immediately postoperatively, at 2 weeks, and at 3 months. Steal syndrome symptoms (pain, pallor, coldness, numbness, and paresthesia) were assessed at follow-ups. Data were analyzed using the Shapiro-Wilk, t test, and Mann-Whitney U tests (P < .05). Of 59 patients (31 men, 28 women; mean age, 56.9 ± 12.6 years), 23 (39%) had temporary steal syndrome, 16 (27.1%) had prolonged steal syndrome, and 3 (5.1%) required vascular…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
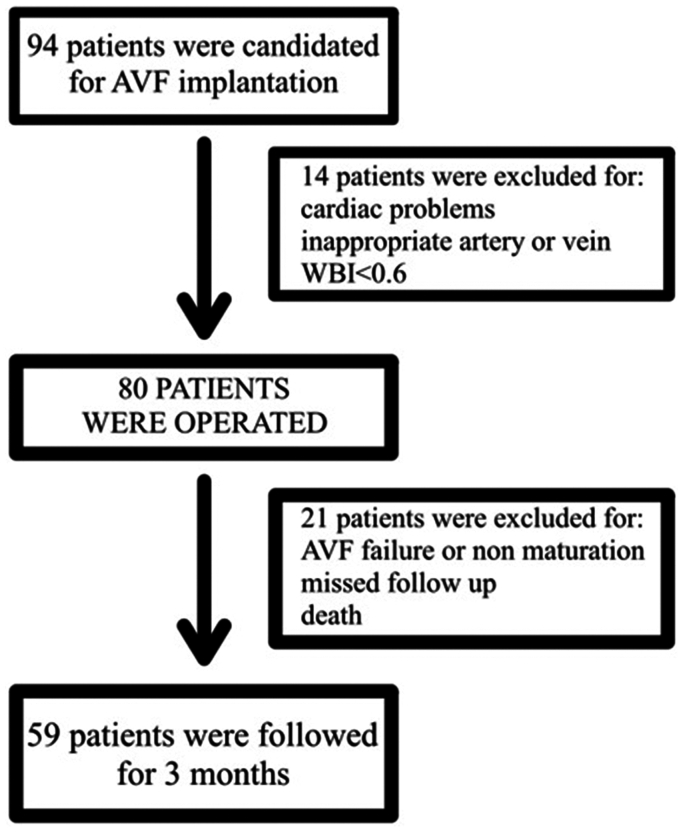 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Procedures and Complications · Central Venous Catheters and Hemodialysis · Peripheral Artery Disease Management
End-stage renal disease is defined as irreversible failure of kidneys function, which leads to death without renal replacement therapy.1 Renal replacement therapy includes renal transplant (as the most effective and best quality of life), hemodialysis, and peritoneal dialysis.2 Most end-stage renal disease patients are managed with hemodialysis. An effective hemodialysis is dependent on functional vascular access to provide sufficient flow to the hemodialysis machine.3 An arteriovenous fistula (AVF) is the preferred vascular access according to clinical guidelines.4 AVF creation involves anastomosing a superficial upper limb vein (eg, cephalic, basilic) to an adjacent artery, promoting vein dilation and arterialization for repeated punctures.5, 6, 7 Steal syndrome, a complication of AVF, results from arterial flow diversion to the venous system, causing limb ischemia.8 Although mild steal syndrome is common, severe ischemia threatening tissue loss occurs in 1% to 10% of patients.4^,^9 Severe cases may present with pain, pallor, pulselessness, or absent Doppler signals, requiring AVF closure.10^,^11 The determination of a single reliable test to predict the steal syndrome after AVF implantation has been the subject of several studies.3^,^12, 13, 14 The wrist-brachial index (WBI), defined as the ratio of wrist to brachial artery pressure, is a noninvasive predictor of arterial insufficiency.15^,^16 The WBI is normally about 1, and a preoperative WBI of <0.6 contraindicates AVF creation.17^,^18 Yet, steal syndrome, including severe cases, can occur in limbs with a normal WBI.19 Postoperative WBI changes may better predict ischemia.12^,^20 This study investigated the correlation between postoperative WBI changes and steal syndrome, including severe ischemia requiring intervention, in AVF patients.
Methods
This prospective study enrolled 94 patients scheduled for first-time AVF implantation using the brachial artery and superficial veins (cephalic, basilic, or median cubital) in 2022. Only patients with first-time AVF implantation using the brachial artery were included. All patients were excluded from distal AVF implantation because of inappropriate distal vessels. According to the guidelines, our preference is always to place distal fistulas when feasible. Exclusion criteria included unsuitable vessels, left ventricular ejection fraction of <30%, inadequate superficial veins (requiring arteriovenous grafts), or preoperative WBI of <0.6. Preoperative assessments included echocardiography, color Doppler ultrasound examination, and Allen's test to confirm intact palmar arch and normal radial/ulnar arteries. Initial WBI screenings were performed in the clinic before surgery. Patients with a WBI less than 0.6 were excluded for that limb. Values of ≥0.6 qualified for surgery, but these were not recorded in detail and thus could not be correlated with postoperative results. None were <0.6 preoperatively. The WBI was calculated as the ratio of wrist pressure to the highest brachial artery pressure from both arms, measured with validated digital sphygmomanometers. Patients with brachial pressure differences of >20 mm Hg also were excluded, reducing the cohort to 80 patients. The WBI was measured preoperatively, immediately postoperatively, at 2 weeks, and at 3 months. AVF functionality was confirmed intraoperatively by thrill or bruit. Patients were assessed for steal syndrome symptoms (pain, pallor, coldness, numbness, and paresthesia) at each follow-up using a standardized checklist. Temporary steal syndrome was defined as symptoms resolving within 3 months, prolonged steal syndrome as symptoms persisting beyond 3 months, and severe steal syndrome as limb-threatening ischemia requiring surgical intervention.
Patients with AVF failure or immature fistulas were excluded to standardize the cohort. These patients were immediately referred for alternative access, and further WBI measurements were not feasible. Patients who were not able to be followed were also excluded, resulting in 59 patients (Fig). Data were analyzed using SPSS 18 with Shapiro-Wilk, t test, and Mann-Whitney U tests (P < .05). The study was approved by the university's ethics committee.FigEnrolment flowchart. AVF, arteriovenous fistula; WBI, wrist-brachial index.
Results
Of 59 patients (31 men, 28 women; mean age, 56.9 ± 12.6 years), 36 (61%) had diabetes, 33 (55.9%) had hypertension, 16 (27.1%) were smokers, and 33 (55.9%) had other comorbidities (eg, coronary disease, hypothyroidism). Forty-two patients (71.2%) had prior hemodialysis via catheters (mean duration, 35.7 ± 12.6 months). The mean preoperative WBI was 0.95 ± 0.11, decreasing to 0.74 ± 0.19 immediately postoperatively, 0.73 ± 0.17 at 2 weeks, and 0.69 ± 0.19 at 3 months (Table I). WBI changes (ΔWBI = [(Current WBI – Preoperative WBI)/Preoperative WBI] × 100) averaged 22.1%, 23.1%, and 27.4% at early, 2-week, and 3-month intervals, respectively (Table II).Table IWrist-brachial index (WBI) measures in different time intervalsThe lowestThe mostAverageStandard deviationWBI before operation0.711.170.950.11WBI immediately after the procedure0.261.200.740.19WBI 2 weeks after surgery0.31.070.730.17WBI 3 months after surgery0.261.330.690.19Table IIWrist-brachial index (WBI) changes in different time intervalsReduction (percent)No reduction (percent)TotalWBI changes Immediately55 (93.22%)4 (6.77%)59 (100%)WBI changes after 2 weeks53 (89.83%)6 (10.16%)59 (100%)WBI changes after 3 months56 (94.91%)3 (5.08%)59 (100%)
Steal syndrome occurred in 23 patients (39%) at 2 weeks (temporary), 16 (27.1%) at 3 months (prolonged), and 3 (5.1%) with severe ischemia requiring surgical intervention (Table III). Seven patients developed new steal syndrome symptoms at 3 months. Patients were classified into four groups based on the occurrence of steal syndrome. This classification is defined in relation to WBI changes in each group in Table IV. Immediate postoperative WBI changes had significant association with steal syndrome incidence (P = .02). Changes in the WBI after 2 weeks and 3 months also correlated with steal syndrome, but these correlations were not meaningful (P = .14 and .11, respectively) (Tables IV and V).Table IIIThe incidence of the different types of steal syndromeNo.PercentTemporary steal syndrome2339Prolonged steal syndrome1627.1Severe steal syndrome35.1Table IVPatients' classification according to the type of steal syndromeGroupNo.PercentAverage ΔWBI (percent)After surgeryAfter 2 weeksAfter 3 months1No steal2949.216.6622.6826.882Only temporary steal1423.733.9821.1232.943Only prolonged steal711.918.7425.6927.144Temporary and prolonged steal915.363.1227.7135.92Total59100WBI, wrist-brachial index.Table VThe association between wrist-brachial index (WBI) changes in different time intervals with the incidence of steal syndromeΔWBIAverage incidence of steal syndromeStandard deviationP-valueImmediately after surgery26.87%22.44%0.02Two weeks after surgery25.37%12.37%0.14Three months after surgery33.9716.630.11
In the severe ischemia subgroup (n = 3), the mean WBI changes were 64.05% (range, 62.23–65.6%) immediately postoperatively, 28.91% (range, 28.19–29.32%) at 2 weeks, and 36.02% (range, 35.23–36.43%) at 3 months. Immediate postoperative WBI changes were significantly associated with severe ischemia (P = .03), but not at 2 weeks (P = .41) or 3 months (P = .38).
By comparing the P values in two other periods and considering the increase in WBI changes over time, it can be concluded that the P values (.14 to .11) are changing toward the reduction and significance of the association. WBI changes correlated significantly with hypertension (P = .01 immediate, P = .02 at 3 months) and smoking (P = .03 at 3 months), but not with age, sex, dialysis duration, diabetes, or body mass index (Tables VI and VII).Table VIThe association between wrist-brachial index (WBI) changes in different time intervals with quantitative variationsΔWBIP value (correlation coefficient)Immediately after surgeryP value (correlation coefficient)Two weeks after surgeryP value (correlation coefficient)Three months after surgeryAge.53 (−0.08).85 (−0.02).79 (0.03)Dialysis duration.50 (0.08).51 (−0.08).81 (0.03)BMI.20 (−0.16).84 (−0.02).45 (−1.0)Table VIIThe association between wrist-brachial index (WBI) changes in different time intervals with qualitative variationsVariationP valueEarly WBI changesP value2 weeks WBI changesP value3 months WBI changesSex.11.10.07Smoking.98.98.03Hypertension.01.79.02Diabetes.31.03.98
Discussion
Steal syndrome complicates AVF implantation, with severe cases requiring intervention in <10% of patients.4 In this study, 50.8% of patients experienced steal syndrome, but only 5.1% had severe ischemia, consistent with prior reports.9 A preoperative WBI of <0.6 contraindicates AVF creation,13 yet steal syndrome, including severe cases, can occur in limbs with normal WBI, necessitating postoperative predictors.17 Early postoperative changes in the WBI are attributed to flow diversion from the arterial system to the venous system through the fistula and resultant decrease in wrist pressure. Therefore, ischemic symptoms are common in the early postoperative period secondary to a decrease in distal arterial perfusion.21^,^22 In our study, 23 patients (39%) experienced ischemic symptoms in the early postoperative period.
The significant association with severe ischemia (P = .03) underscores the predictive value of early WBI changes. Over time, distal arterial vasodilation reduces peripheral vascular resistance, increasing limb flow despite a lower WBI.23^,^24 This adaptation explains why late WBI changes (2 weeks: P = .41; 3 months: P = .38) were less predictive of steal syndrome.
Hypertension and smoking correlated with WBI changes, likely owing to their effects on vascular compliance.24 The lack of association with diabetes, age, or body mass index suggests hemodynamic factors primarily drive WBI changes.
Limitations
The sample size (n = 59) and small severe ischemia subgroup (n = 3) limit statistical power for subgroup analyses. The absence of a validated steal syndrome questionnaire may introduce subjectivity. Future studies with larger cohorts should explore longitudinal WBI trends and additional predictors, such as arterial diameter ratios.22
Conclusions
Although a preoperative WBI of ≥0.6 remains the minimum threshold for AVF creation, significant immediate postoperative WBI reductions are a serious risk factor for steal syndrome and should prompt close follow-up, especially when combined with hypertension or smoking. Immediate postoperative WBI changes reliably predict steal syndrome, including severe cases requiring intervention, after AVF implantation. Patients with significant early WBI reductions, particularly >60%, require close monitoring to detect and manage ischemic complications promptly.
Funding
None.
Disclosures
None.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abbasi M.A.Chertow G.M.Hall Y.N.End-stage renal disease BMJ Clin Evid 201020102002 PMC 321782021418665 · pubmed ↗
- 2Caskey F.J.Kramer A.Elliott R.F.Global variation in renal replacement therapy for end-stage renal disease Nephrol Dial Transplant 262011260426102124513110.1093/ndt/gfq 781 · doi ↗ · pubmed ↗
- 3Miller P.E.Tolwani A.Luscy C.P.Predictors of adequacy of arteriovenous fistulas in hemodialysis patients Kidney Int 5619992752801041170310.1046/j.1523-1755.1999.00515.x · doi ↗ · pubmed ↗
- 4Lok C.E.Huber T.S.Lee T.KDOQI clinical practice guideline for vascular access: 2019 update Am J Kidney Dis 752020 S 1S 1643277822310.1053/j.ajkd.2019.12.001 · doi ↗ · pubmed ↗
- 5Albayrak R.Yuksel S.Colbay M.Hemodynamic changes in the cephalic vein of patients with hemodialysis arteriovenous fistula J Clin Ultrasound 3520071331371727403510.1002/jcu.20307 · doi ↗ · pubmed ↗
- 6Georgakarakos E.I.Kapoulas K.C.Georgiadis G.S.Tsangaris A.S.Nikolopoulos E.S.Lazarides M.K.An overview of the hemodynamic aspects of the blood flow in the venous outflow tract of the arteriovenous fistula J Vasc Access 1320122712782226658310.5301/jva.5000037 · doi ↗ · pubmed ↗
- 7Chandra A.Mix D.Varble N.Hemodynamic study of arteriovenous fistulas for hemodialysis access Vascular 21201354622310482510.1258/vasc.2011.201204 · doi ↗ · pubmed ↗
- 8Wixon C.L.Hughes J.D.Mills J.L.Understanding strategies for the treatment of ischemic steal syndrome after hemodialysis access 1J Am Coll Surg 19120003013101098990410.1016/s 1072-7515(00)00335-5 · doi ↗ · pubmed ↗