Intensity-modulated radiotherapy with carbon ion boost for high-risk sinonasal squamous cell carcinoma: clinical outcomes and the management of the node-negative neck
Lukas Bauer, Katharina Weusthof, Sebastian Regnery, Maximilian Deng, Philipp Schröter, Florian Stritzke, Nils Netzer, Henrik Franke, Kristin Uzun-Lang, Julius Moratin, Oliver Ristow, Rubens Thoelken, Semi B. Harrabi, Klaus Herfarth, Sebastian Adeberg, Jürgen Debus, Thomas Held

TL;DR
Combining intensity-modulated radiotherapy with a carbon ion boost improves local control and survival in high-risk sinonasal cancer with low toxicity.
Contribution
First clinical outcomes of combined IMRT and carbon ions for sinonasal SCC with insights on neck management.
Findings
OS and local progression-free survival at 12/24 months were 93.0%/89.3% and 88.4%/79.0%.
Grade III toxicity occurred in 9.3% of patients with no grade IV events observed.
Individualized neck treatment reduced radiation toxicity without compromising outcomes.
Abstract
•Carbon ion boost with IMRT shows high local control in sinonasal SCC.•Node-negative neck management remains variable in sinonasal SCC treatment.•Treatment shows low grade III toxicity with no grade IV events observed.•First clinical outcomes of combined IMRT and carbon ions for sinonasal SCC.•Study supports individualized neck treatment to reduce radiation toxicity. Carbon ion boost with IMRT shows high local control in sinonasal SCC. Node-negative neck management remains variable in sinonasal SCC treatment. Treatment shows low grade III toxicity with no grade IV events observed. First clinical outcomes of combined IMRT and carbon ions for sinonasal SCC. Study supports individualized neck treatment to reduce radiation toxicity. Local control of high-risk sinonasal squamous cell carcinoma (SCC) remains challenging and often involves significant morbidity. Management of the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
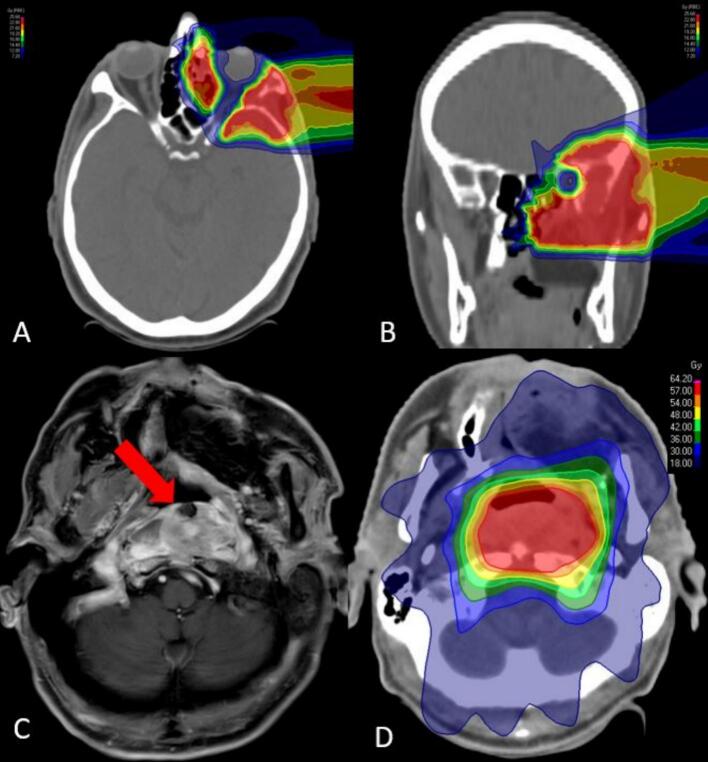 Figure 1
Figure 1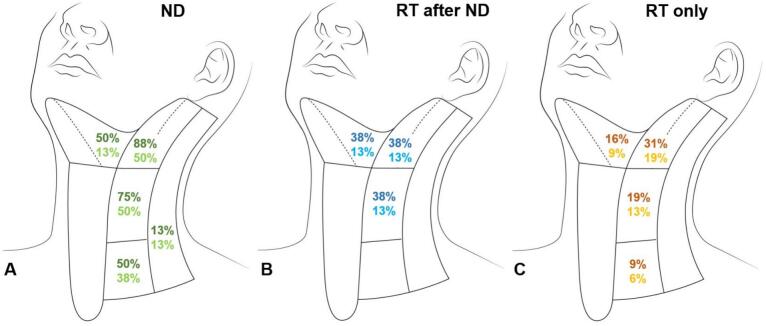 Figure 2
Figure 2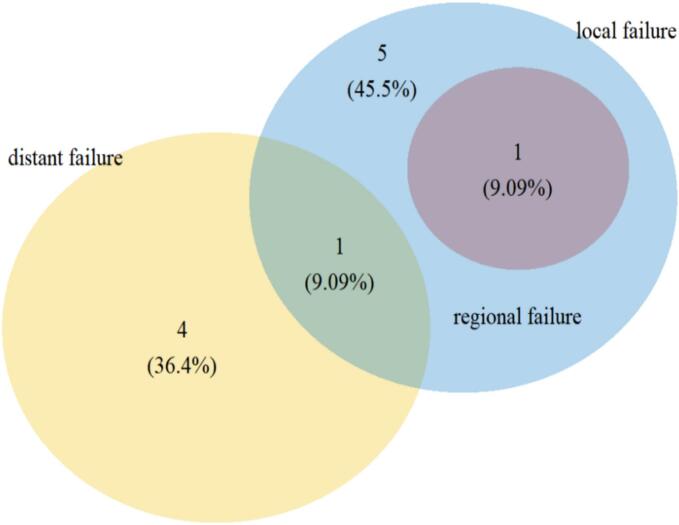 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHead and Neck Surgical Oncology · Head and Neck Cancer Studies · Sinusitis and nasal conditions
Introduction
Sinonasal cancer, comprised of a heterogenous group of different tumor entities, constitutes around 3 % of all head and neck cancers [1]. The most common histology (50–60 %) is squamous cell carcinoma (SCC) [2], which may show overlapping morphological and functional features with other histological subtypes, e.g. sinonasal undifferentiated carcinoma [3]. Due to the rarity of early symptoms, sinonasal cancer is often diagnosed at an advanced tumor stage, requiring a multidisciplinary treatment approach [4]. In general, local recurrence after surgery and postoperative radiotherapy (RT) occurs within five years post-treatment in around half of the patients [5]. However, the therapeutic options have improved noticeably within recent years, among others due to developments in imaging techniques, endoscopic or computer-assisted surgery and intensity-modulated radiotherapy (IMRT) [1]. Nonetheless, a tradeoff between optimal tumor control and function preservation of organs at risk, e.g. the optic system, is frequently inevitable due to orbital or cranial nerve involvement. The biophysical properties of carbon ion RT (CIRT) enable both improved normal tissue sparing and dose escalation [6]. In addition, the increased relative biological effectiveness (RBE) and decreased oxygen dependence of CIRT are beneficial in radioresistant tumors [7,8]. Previous studies on CIRT of sinonasal cancer reported favorable local control and toxicity rates, compared to conventional RT for various tumor entities [[9], [10], [11]]. In a more recent publication from our center, the first prospective data on the toxicity and clinical outcomes of bimodal radiation therapy (CIRT + IMRT) for sinonasal malignancies were presented, specifically adenocarcinoma and squamous cell carcinoma, demonstrating a low incidence of acute toxicity alongside encouraging tumor control and survival rates [12]. However, clinical data on the effectiveness of CIRT for sinonasal SCC is scarce. In this context, carbon ion therapy offers distinct therapeutic advantages. Owing to their physical characteristics, carbon ions enable highly conformal dose distributions with sharp dose fall-off, which is particularly relevant in the anatomically complex paranasal sinus region where critical structures lie in close proximity. Beyond these physical benefits, carbon ions also exhibit increased relative biological effectiveness due to their higher linear energy transfer, resulting in increased cytotoxic efficacy even in more resistant histologies [[13], [14], [15]]. Also the management of the neck remains controversial in patients with sinonasal SCC, in particular for the node-negative-neck there is no established treatment standard [16]. The risk of nodal metastases in sinonasal SCC, primarily level Ib, IIa and VIIa, was reported to be around 7–22 % depending primarily on the tumor localization and T-stage [17]. Elective neck dissection can improve disease-specific survival in advanced stage maxillary sinus SCC [18] and is commonly recommended for T3–4 sinonasal cancer. Elective neck irradiation may reduce the rate of nodal recurrence in the cN0 situation [19] in advanced stage tumors. However, the question if a less radical approach with regard to the neck could be feasible to reduce toxicity in selected patients with advanced sinonasal SCC remains unclear. The aim of the current study was to investigate the treatment outcome, management of the neck and toxicity rates of IMRT with carbon ion boost in patients with sinonasal SCC.
Methods
Patient selection
After approval by the regional ethics committee (reference number S-421/2015, date of approval 18.06.2024), all patients with head and neck cancer treated by photon intensity-modulated radiotherapy (IMRT) with carbon ion boost at our institution were screened. All patients with squamous cell carcinoma (SCC) of the nasal cavity or paranasal sinuses treated between 2011 and 2019 were included. After exclusion of patients with incomplete clinical data or follow-up, a total of 43 patients were evaluated in the current study. A subgroup of 17 patients were treated within the IMRT-HIT-SNT phase II trial [12].
Treatment planning
All patients were staged with CT of the neck and thorax and abdominal ultrasound. For precise delineation of the primary tumor and evaluation of the neck, a contrast-enhanced MRI of the neck was also performed.
Patients were immobilized in treatment position using thermoplastic head mask systems. The target volume delineation was conducted based on contrast-enhanced CT and MRI. The recommendations of the International Commission on Radiation Units and Measurements (ICRU) [20,21] were considered. Dose constraints of normal tissues were respected according to the Quantitative Analyses of Normal Tissue Effects in the Clinic [22].
The CTV boost included macroscopic tumor and/or the tumor bed with safety margins along typical pathways of spread. An isotropic margin of 3 mm was added for the PTV boost. The local effect model (LEM) I was applied for radiobiological modelling of the RBE of ions and calculation of the RBE-weighted dose [23,24]. An α/β value of 2 Gy was used for dose calculation with regard to the target and OAR [25,26]. The cumulative dose was specified by the equivalent dose in 2 Gy fractions (EQD2). The beam setup was individualized for each patient, optimized to mitigate range uncertainties caused by anatomical changes in the beam directions (e.g. mucosal swelling). CIRT was performed using active raster scanning technique. Daily orthogonal X-rays were used for image-guidance prior to irradiation followed by position correction. CIRT was applied with a single dose of 3 Gy (RBE) and 5–6 fractions per week. Most patients received the carbon ion boost at the beginning.
The CTV included the CTV boost and involved anatomical sites as well as the locoregional lymph nodes. A margin of 3 mm was added for the PTV. Further dose levels were added in the case of diagnosed lymph node metastases. Image-guidance for IMRT consisted of daily MV cone-beam CTs. If required, the treatment plan was adapted to anatomical and positional changes. RT was delivered with a 6 MV-linear accelerator using the step-and-shoot IMRT, Volumetric Intensity Modulated Arc Therapy (VMAT) or Tomotherapy® technique. RT was applied with a single dose of 2 Gy and 5 fractions per week. A patient case is shown in Fig. 1.Fig. 163-year-old male patient with a high-grade T4N0M0 squamous cell carcinoma of the paranasal sinuses. The patient received radiotherapy (RT) with 24 Gy (RBE) carbon ions (A + B) allowing for excellent preservation of the visual system followed by 50 Gy intensity-modulated RT (IMRT) after R0-resection. A local recurrence outside the clinical target volume of the carbon ion boost was diagnosed 21 months after RT (C). The patient received re-irradiation with a total dose of 60 Gy in 30 fractions IMRT (D).
Follow-up
Clinical follow-up was conducted with MRI or CT of the head and neck 6–8 weeks after RT, every 3 months within the first 2 years, every 6 months in the third year and thereafter every year post-treatment. CT thorax and abdominal sonography was performed once per year. Toxicity was recorded non-standardized by a radiation oncologist according to CTCAE v5.0 and analyzed retrospectively. Patients presented either to the ear, nose and throat specialist or the maxillofacial surgeon for clinical examination in regular intervals.
Statistical analysis
Statistical analysis was performed using R version 4.1.0 (https://www.r-project.org). Toxicity analysis was conducted using CTCAE v5.0. The mean number of toxicity events per patient was assessed based on the TAME method [27]. The mean number of grade III acute toxicity events per patient was compared between patients who underwent elective lymph node irradiation and those who did not, applying the Mann–Whitney U test. The median follow-up with regard to OS was determined using the inverse Kaplan-Meier method. OS, progression-free survival (PFS), local progression-free survival (L-PFS) and metastasis-free survival (MFS) were analyzed from the end of RT until death or tumor progression using the Kaplan-Meier method. Prognostic factors for OS were explored using the log-rank test. Multivariate analysis was inconclusive due to only few events during follow-up and therefore not evaluated.
Results
Patient and treatment characteristics
The median age before RT was 64 years (range 19–83 years) and most patients were male (n = 28; 65.1 %). The median time of hospitalization during RT was 7 days (range 0–53 days). The median time from initial diagnosis to RT was 3.1 months (range 1.0–93.1 months). A percutaneous gastric feeding tube was required in one patient (2.3 %). A total of 4 patients (9.3 %) had previous or synchronous and 2 patients (4.7 %) metachronous secondary malignancies, primarily in the aerodigestive tract. The majority of patients had G2 (n = 17; 39.5 %) or G3 (n = 24; 55.8 %) tumors. Distant metastases were present in 2 patients (4.7 %) prior to RT. Further patient and treatment characteristics are shown in Table 1.Table 1. Patient and radiation treatment characteristics (n = 43 patients).Patients**%SexFemale1534.9Male2865.1Primary tumor localizationParanasal sinuses3274.4Nasal cavity1125.6T-stage prior to RTT1-2716.3T3716.3T42967.4Smoking≥10 pack years716.3<10 pack years12.3Never3581.4RT settingAdditive2046.5Definitive1841.9Adjuvant511.6ChemotherapyNeoadjuvant24.6Simultaneous CRT1841.9None2353.5Resection statusR0825.8R1619.4R2722.6RX1032.2Optimization strategy C12Single beam optimization37.0Intensity-modulated particle therapy4093.0C12 gantryyes1227.9no3172.1Median****Range**Age prior to RT [years]6419–83KPS prior to RT [%]9070–100BMI prior to RT [kg/m^2^]26.414.9–52.0BMI post RT [kg/m^2^]25.815.2–51.9Hospitalization during RT [days]70–53Total dose IMRT [Gy]50.050.0–60.0Total dose C12 boost [Gy RBE]24.012.0–24.0Cumulative total dose [Gy EQD2]80.075.0–80.0RT fractions3332–34Treatment time / fraction IMRT [min]5.12.7–8.2Treatment time / fraction C12 [min]8.04.0–17.0PTV [ccm]312.5111.5–845.9PTV C12 boost [cm^3^]166.041.2–503.0CTV [cm^3^]320.073.1–793.4CTV C12 boost [cm^3^]113.722.1–408.2GTV [cm^3^]49.54.2–214.0Beam number21–4Total number of C12 scan spots17,6894,956–47,999Maximum energy C12 [MeV/u]247.7182.0–297.8Abbreviations: Radiotherapy (RT), chemoradiotherapy (CRT), Karnofsky Performance Score (KPS), body mass index (BMI), intensity-modulated RT (IMRT), relative biological effectiveness (RBE), equivalent dose in 2 Gy fractions (EQD2), planning target volume (PTV), clinical target volume (CTV), gross tumor volume (GTV).
The most common treatment regimen was 24 Gy (RBE) carbon ion boost in 8 fractions followed by 50 Gy IMRT in 25 fractions, consistent with a cumulative dose of 80 Gy EQD2. Most patients received postoperative (n = 25; 58.1 %) compared to definitive RT (n = 18; 41.9 %). A total of 31 patients (72.1 %) received surgical treatment at some point. The median number of surgical treatments prior to RT was 1 (range 0–4). Most patients (n = 40; 93.0 %) had no clinical evidence of lymph node metastases prior to treatment. In this cohort, 8 patients (20.0 %) received a neck dissection, none had detected lymph node metastases. Only one patient with tumor infiltration of the nasopharynx had diagnosed lymph node metastases in level II–III bilaterally. There were 22 different treatment constellations for the cervical lymph nodes, which are summarized in Table 2/Fig. 2.Table 2. Clinical management of the cervical lymph nodes in patients with sinonasal SCC.**Pat.cN + levelsND levelspN + levelsRT levels****Node negative neck (n = 40)**Ipsilateral ND (n = 4)1NoneI-IIInoneI-III + RPipsilat.1Inonenonen.a.1I-IInonenonen.a.1II-IVnonenonen.a.Bilateral ND (n = 4)1II-VnoneI-III + RPbilat.1II-IVnoneI-III + RPipsilat.1I-IIInonenonen.a.1II-IVnonenonen.a.No ND (n = 32)12nonen.a.nonen.a.4nonen.a.I-IV + RPbilat.4nonen.a.II + RPbilat.1nonen.a.I-II + RPbilat.1nonen.a.II-III + RPbilat.1nonen.a.I-III + RPbilat.1nonen.a.II-IV + RPbilat.4nonen.a.II-III + RPipsilat.2nonen.a.I-IV + RPipsilat.1nonen.a.I-II + RPipsilat.1nonen.a.II + RPipsilat.**Node positive neck (n = 3)**Ipsilateral neck dissection1II ipsilat.I-III ipsilat.noneI-III + RPipsilat.Bilateral neck dissection1II-IV ipsilat.II-IVnoneI-IV + RPipsilat.No neck dissection1II-III bilat.nonen.a.II-IV + RPbilat.Abbreviations: Squamous cell carcinoma (SCC), neck dissection (ND), radiotherapy (RT), retropharyngeal (RP).Fig. 2A total of 40 patients (93 %) had a clinical node-negative neck. Shown are the rates of ipsilateral (dark color) and bilateral (light color) elective neck treatment for each lymph node level in patients with neck dissection (ND; n = 8; A) ± radiotherapy (RT) after ND (B) and without ND (n = 32; C). None of the patients with elective ND had lymph node metastases. A total of 12 patients (30 %) received no elective neck treatment. The extent of elective treatment was lower in the RT only group compared to both ND only and RT after ND. In all patients treated with RT, the retropharyngeal lymph nodes where included.
Treatment outcome
The median follow-up with regard to OS after RT was 25.1 months (range 2.0–100.0 months).
The one- and two-year PFS was 79.1 % and 75.5 %, respectively (supplementary figure 1). Most patients with disease progression after RT developed local failure (n = 7; 63.6 %) and 4 of these local relapses (36.4 %) occurred within the carbon ion boost CTV. Regional failure occurred in one patient who also developed simultaneous local failure. The pattern of failure is shown in Fig. 3.Fig. 3. Venn diagram showing the pattern of local, regional and distant failure for all patients with progressive disease after radiotherapy (n = 11; 25.6 %), analyzed regarding the site of first failure only. Most patients developed local failure (n = 7; 63.6 %), the majority within the clinical target volume of the carbon ion boost (n = 4; 36.4 %). Only one patient developed regional failure.
The OS, L-PFS and MFS after 12/24 months were 93.0 %/89.3 %, 88.4 %/79.0 %, and 86.0 %/86.0 % (supplementary figure 2–4). The total hospitalization days were the only prognostic factor associated with decreased OS (p = 0.012; supplementary figure 5). Further factors, among others CRT vs. RT, postoperative vs. definitive RT or the Karnofsky Performance Score had no significant impact on OS.
Acute and late toxicity
Radiotherapy was discontinued in one patient (2.3 %) due to newly diagnosed brain metastases during treatment. All other patients could complete RT without interruptions. The cumulative rate of acute grade III toxicity was 9.3 % (n = 4). Acute grade III toxicity events included oral mucositis, radiation dermatitis and weight loss. The mean number of acute grade I and II toxicity events per patient was 1.7 (95 %-confidence interval [CI] 1.2–2.1) and 3.1 (95 %-CI 2.5–3.8). The most common grade I–II acute toxicities were oral mucositis (n = 28; 65.1 %), dysphagia (n = 25; 58.1 %) and radiation dermatitis (n = 22; 51.2 %). The mean number of grade III acute toxicity events per patient was higher if elective lymph node irradiation was performed (0.24 vs. 0.03; p = 0.181).
The cumulative rate of late grade III toxicity was 4.7 % (n = 2). Late grade III toxicities included dysphagia and hearing impairment. The mean number of late grade I and II toxicity was 1.7 (95 %-CI 1.3–2.1) and 0.7 (95 %-CI 0.4–0.9). The most common grade I–II late toxicities were dry mouth (n = 18; 41.9 %), dysgeusia (n = 16; 37.2 %) and lymph edema (n = 13; 30.2 %). No grade IV acute or late toxicity was reported. Further details on the mean number and total counts of acute and late toxicity events are summarized in Table 3a, Table 3b.Table 3aMean number of CTCAE v5.0 toxicity events and overall toxicity per patient (n = 43).Mean95 %-CIPatients**%Acute short-term toxicityCTC grade I1.71.2–2.112.3CTC grade II3.12.5–3.83888.4CTC grade III0.10–0.249.3Late toxicity**CTC grade I1.71.3–2.11637.2CTC grade II0.70.4–0.91739.5CTC grade III0.10–0.124.7Abbreviations: Common Terminology Criteria of Adverse Events (CTCAE), confidence interval (CI); Comment: If a patient had more than one toxicity event, only the highest toxicity grade was counted once in the total count category.Table 3bMost common CTCAE v5.0 grade I-III acute short-term and late toxicities (n = 43).**Acute toxicityLate toxicity****° I****° II****° III****° I****° II****° III**Oral mucositis4 (9.3 %)24 (55.8 %)3 (7.0 %)3 (7.0 %)00Dysphagia7 (16.3 %)18 (41.9 %)04 (9.3 %)1 (2.3 %)1 (2.3 %)Radiation dermatitis11 (25.6 %)11 (25.6 %)1 (2.3 %)4 (9.3 %)00Dry mouth5 (11.6 %)4 (9.3 %)016 (37.2 %)2 (4.7 %)0Dysgeusia1 (2.3 %)10 (23.3 %)013 (30.2 %)3 (7.0 %)0Fatigue6 (14.0 %)6 (14.0 %)09 (20.9 %)00Mucosal infection010 (23.3 %)0000Lymph edema2 (4.7 %)3 (7.0 %)07 (16.3 %)6 (14.0 %)0Weight loss5 (11.6 %)6 (14.0 %)1 (2.3 %)1 (2.3 %)4 (9.3 %)0Dry eye2 (4.7 %)7 (16.3 %)0000Nausea2 (4.7 %)7 (16.3 %)0000Dehydration2 (4.7 %)7 (16.3 %)0000Hearing impariment3 (7.0 %)3 (7.0 %)04 (9.3 %)3 (7.0 %)1 (2.3 %)Conjunctivitis3 (7.0 %)4 (9.3 %)01 (2.3 %)2 (4.7 %)0Trismus2 (4.7 %)2 (4.7 %)04 (9.3 %)1 (2.3 %)0Optic nerve disorder1 (2.3 %)002 (4.7 %)2 (4.7 %)0Abbreviations: Common Terminology Criteria of Adverse Events (CTCAE), Comment: Acute toxicity that continued in the late phase was counted as both acute and late toxicity.
Discussion
The current study reports first clinical results of IMRT with carbon ion boost in patients with high-risk sinonasal SCC. Radiotherapy yielded promising early tumor control rates and was associated with favorable toxicity. Treatment decisions with regard to the management of node-negative-neck were challenging and highly individualized.
The reported results raise the question whether dose escalation using IMRT with carbon ion boost could improve local control in high-risk sinonasal SCC. Our findings indicate better local control compared to historical cohorts, where local recurrence rates after surgery and postoperative RT approached 50 % at five years [28]. The only prospective study on CIRT for sinonasal cancers reported 2-year OS and L-PFS rates of 79.4 % and 61.8 %, respectively [12]. Our study seems to be in line with these results, showing 2-year OS and L-PFS of 89.3 % and 79.0 % after a carbon ion boost, suggesting that this strategy leads to favorable outcomes compared to historical cohorts.
A major challenge in the treatment of sinonasal squamous cell carcinoma (SCC) remains the high rate of local failure, which persists even with the integration of a carbon ion boost. In our series, more than one-third of local recurrences occurred within the carbon ion boost volume, underscoring that while CIRT achieves excellent dose conformity and biological effectiveness, there is still considerable room for improvement in local control. By contrast, nodal failures were infrequent, regardless of the heterogeneous management strategies applied, suggesting that the primary barrier to long-term disease control in this setting continues to lie within the local tumor compartment.
It is important to recognize that CIRT is a relatively young technique and remains under continuous technical and biological refinement. One potential strategy for further optimization is the underlying radiobiological modeling of the relative biological effectiveness (RBE). In our cohort, dose prescription was based on the Local Effect Model I (LEM I). However, other models are in clinical use, including the modified microdosimetric kinetic model (mMKM) and the MKM-derived Japanese biological model (NIRS-MKM), each of which results in different RBE-weighted dose distributions. Recent developments in treatment planning allow for mixed- or multi-RBE optimization, where distinct RBE models can be applied to different regions of interest [29]. Such strategies may enable a more accurate biological dose calculation, particularly in the context of heterogeneous tumor volumes or advanced-stage disease, where dose–effect relationships may differ substantially. These ongoing refinements highlight that current clinical outcomes with CIRT should be interpreted within the framework of evolving radiobiological models. In particular, given that the majority of patients in our cohort presented with locally advanced SCC, further research is warranted to determine whether such subgroups − especially those with larger tumor volumes or higher-stage disease − derive a specific benefit from this approach. Whether the proposed carbon ion boost regimen is the most appropriate approach to improve local control, compared with definitive hypofractionated CIRT, cannot be determined from this study, as only indirect comparisons with previously published data are possible. Prospective randomized studies are needed to clarify this question and to establish evidence-based treatment standards.
In addition, our results provide further clinical evidence that biophysical benefits of CIRT might translate into reduced toxicity rates compared to conventional RT in patients with sinonasal cancer. Despite precision advantages of IMRT [30] and complication reduction by endoscopic surgery [31], a benefit-risk-tradeoff between tumor control and organ function preservation is often required. In particular elderly patients are at risk for increased toxicity [32]. Historic series provide important context for toxicity outcomes. Suh et al. reported a markedly lower incidence of acute grade 3 mucositis with IMRT (16 %) compared to 3D-RT (37 %) [33]. In a pooled analysis of available studies, Zhang et al. observed slightly higher rates of acute grade 3–4 toxicity following CIRT (>30 %) relative to IMRT (24 %) [9]. Across treatment modalities, late toxicity was consistently reported in the range of 10–13 %. On the contrary, favorable toxicity rates of IMRT with carbon ion boost were previously reported for various sinonasal tumors, among others adenoid cystic carcinoma, adenocarcinoma and malignant melanoma [10,34,35]. The rate of grade III toxicity ranged between 0–40 %. In line with these studies, the rate of acute and late grade III toxicity was 9.3 % and 4.7 % in the current analysis. Considering the high-risk tumor characteristics, the mean number of grade I–II acute and late toxicity events per patient of 4.8 and 2.4 was acceptable. Nevertheless, the ability to ascertain whether the addition of a carbon ion boost confers a clinically meaningful reduction in toxicity compared with IMRT remains limited, owing to the retrospective design and the non-standardized nature of toxicity assessment in our study. Although non-significant, there was a trend towards fewer grade III toxicity events in patients without RT of the lymph nodes. Evaluated in prospective clinical trials, improved toxicity rates through reduced volumes of lymph node RT were previously reported [36]. However, any approach to reduce toxicity based on a less intense treatment of the neck should consider the potentially increased risk for regional recurrence. In the case of positive lymph nodes, there is a significant adverse effect on local control, distant spread and OS [17,37].
The management of the neck was highly individualized in the current study with a total of 22 different treatment constellations. Although patients could benefit from a personalized approach in general, evidence-based treatment algorithms are required. Most patients in our study had cN0 status (n = 40; 93.0 %) and only one patient (2.3 %) with tumor extension to the nasopharynx initially had diagnosed lymph node metastases. In patients with maxillary sinus SCC and initial cN0 status (81–94 % % of the patients), the rate of regional recurrence was reported between 3–30 % without elective lymph node irradiation [37]. The regional control was excellent in the current study since only one patient developed combined local and nodal failure. However, most patients (n = 30; 69.8 %) received elective neck treatment, 25 patients (58.1 %) either neck dissection or RT and 5 patients (n = 11.6 %) both. Elective neck treatment with RT was generally less extensive than with ND ± RT. Although prophylactic treatment of the node-negative-neck remains controversial [28], it is generally recommended in locally advanced sinonasal SCC (T3–4 stage) due to the risk of nodal involvement [18]. Tumor localization in the maxillary sinus and extension to the oral cavity or nasopharynx are further risk factors for nodal spread [17]. For selected patients with N0 status and low risk for nodal involvement, deescalation of the lymph node treatment could be beneficial. The most obvious possible measure is to treat advanced stage node-negative sinonasal SCC with either elective neck dissection or nodal irradiation but not both. The reported rates or regional recurrence after neck dissection without additional lymph node RT were reported around 5–15 % [38,39]. Selective neck dissection may be feasible to detect occult lymph node metastases in sinonasal SCC [40], but does not improve neck control [38]. The rate of neck recurrence after elective nodal irradiation without prior neck dissection was reported around 0–5 % [19,41,42]. Further possible deescalation strategies include the reduction of irradiated lymph node volume based on a certain threshold of nodal involvement for each level [43]. Besides rarely involved lymph node levels (e.g. IV–V) in node-negative tumors, irradiation of the contralateral neck can be omitted in well-lateralized tumors without contralateral neck involvement. However, data to support this treatment algorithm in sinonasal SCC is scarce, based on retrospective studies and inhomogeneous, e.g. with regard to diagnostic workup. Furthermore, physiological lymph node drainage routes are often individual and complex and can be influenced among others by surgery or tumor extension [44]. Therefore, risk-adapted neck irradiation guided by lymph node scintigraphy could enhance consistency, e.g. with regard to the controversial levels VIIa and IX. Also, photoacoustic molecular imaging shows potential to detect occult metastatic lymph nodes in patients with head and neck cancer [45]. Further clinical evidence using modern imaging, radiation techniques and patient reported outcomes is required to improve evidence-based treatment algorithms of the node-negative-neck in sinonasal SCC.
Limitations
The current study had several limitations. First, the toxicity was recorded non-standardized for most of the patients. Second, further long-term follow-up is required to evaluate treatment outcome. Third, the treatment regimens with regard to the management of the neck were rather heterogeneous. Despite these limitations, the current study reported encouraging results, thereby adding valuable evidence to the recent developments in the radiation treatment of high-risk sinonasal SCC.
Conclusions
In the current study, first clinical results of IMRT with carbon ion boost in patients with high-risk sinonasal SCC showed encouraging early local tumor control and OS. The management of the node-negative-neck was highly individualized. Toxicity rates were encouraging and could be further reduced by a less radical treatment approach of the cervical lymph nodes in selected patients.
Funding support
T.H., M.D. and F.S. are funded by the Physician-Scientist Program of Heidelberg University, Faculty of Medicine.
CRediT authorship contribution statement
Lukas Bauer: Data curation, Investigation, Validation, Methodology, Visualization, Writing – original draft, Writing – review & editing. Katharina Weusthof: Data curation, Investigation, Validation, Methodology, Writing – review & editing. Sebastian Regnery: Data curation, Investigation, Validation, Methodology, Writing – review & editing. Maximilian Deng: Data curation, Investigation, Validation, Methodology, Writing – review & editing. Philipp Schröter: Data curation, Investigation, Validation, Methodology, Writing – review & editing. Florian Stritzke: Data curation, Investigation, Validation, Methodology, Writing – review & editing. Nils Netzer: Data curation, Investigation, Validation, Methodology, Writing – review & editing. Henrik Franke: Data curation, Investigation, Validation, Methodology, Writing – review & editing. Kristin Uzun-Lang: Data curation, Investigation, Validation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. Julius Moratin: Data curation, Investigation, Validation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. Oliver Ristow: Data curation, Investigation, Validation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. Rubens Thoelken: Data curation, Investigation, Validation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. Semi B. Harrabi: Data curation, Investigation, Validation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. Klaus Herfarth: Data curation, Investigation, Validation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. Sebastian Adeberg: Data curation, Investigation, Validation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. Jürgen Debus: Data curation, Investigation, Validation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. Thomas Held: Data curation, Investigation, Validation, Methodology, Visualization, Writing – original draft, Project administration, Supervision.
Declaration of competing interest
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: J.D. reports grants from CRI The Clinical Research Institute, grants from View Ray Inc., grants from Accuray International, grants from Accuray Incorporated, grants from RaySearch Laboratories AB, grants from Vision RT limited, grants from Merck Serono GmbH, grants from Astellas Pharma GmbH, grants from Astra Zeneca GmbH, grants from Siemens Healthcare GmbH, grants from Solution Akademie GmbH, grants from Eromed PLC Surrey Research Park, grants from Quintiles GmbH, grants from Pharmaceutical Research Associates GmbH, grants from Boehringer Ingelheim Pharma GmbH Co, grants from PTW-Frieburg Dr. Pychlau GmbH, grants from Nanobiotix A.a., outside the submitted work. The other authors declare no conflict of interest. S.A. reports grants from Novocure Inc., Accuray International Sàrl, Merck Sharp&Dohme, Sanofi-Aventis GmbH and Merk Serono GmbH outside the submitted work.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Llorente J.L.López F.Suárez C.Hermsen M.A.Sinonasal carcinoma: clinical, pathological, genetic and therapeutic advances Nat Rev Clin Oncol 11201446047210.1038/nrclinonc.2014.9724935016 · doi ↗ · pubmed ↗
- 2Turner J.H.Reh D.D.Incidence and survival in patients with sinonasal cancer: a historical analysis of population‐based data Head Neck 34201287788510.1002/hed.2183022127982 · doi ↗ · pubmed ↗
- 3De Cecco L.Serafini M.S.Facco C.Granata R.Orlandi E.Fallai C.A functional gene expression analysis in epithelial sinonasal cancer: biology and clinical relevance behind three histological subtypes Oral Oncol 9020199410110.1016/j.oraloncology.2019.02.00330846184 · doi ↗ · pubmed ↗
- 4Guntinas-Lichius O.Kreppel M.P.Stuetzer H.Semrau R.Eckel H.E.Mueller R.P.Single modality and multimodality treatment of nasal and paranasal sinuses cancer: a single institution experience of 229 patients Eur J Surg Oncol (EJSO)33200722222810.1016/j.ejso.2006.10.03317127030 · doi ↗ · pubmed ↗
- 5Blanco A.I.Chao K.S.C.Ozyigit G.Adli M.Thorstad W.L.Simpson J.R.Carcinoma of paranasal sinuses: long-term outcomes with radiotherapy Int J Radiat Oncol *Biol *Phys 592004515810.1016/j.ijrobp.2003.09.10115093898 · doi ↗ · pubmed ↗
- 6Schulz-Ertner D.Karger C.P.Feuerhake A.Nikoghosyan A.Combs S.E.Jäkel O.Effectiveness of carbon ion radiotherapy in the treatment of skull-base chordomas Int J Radiat Oncol *Biol *Phys 68200744945710.1016/j.ijrobp.2006.12.05917363188 · doi ↗ · pubmed ↗
- 7Mattke M.Vogt;K.Bougatf N.Welzel T.Oelmann-Avendano J.Hauswald H.High control rates of proton‐ and carbon‐ion–beam treatment with intensity‐modulated active raster scanning in 101 patients with skull base chondrosarcoma at the Heidelberg Ion Beam Therapy Center Cancer 12420182036204410.1002/cncr.3129829469932 · doi ↗ · pubmed ↗
- 8Uhl M.Mattke M.Welzel T.Oelmann J.Habl G.Jensen A.D.High control rate in patients with chondrosarcoma of the skull base after carbon ion therapy: first report of long‐term results Cancer 12020141579158510.1002/cncr.2860624500784 · doi ↗ · pubmed ↗