Quality of life after laparoscopic totally extraperitoneal (TEP) inguinal hernia repair with fibrin glue versus tack mesh fixation
Ahmed Anwar, Waleed M. Ghareeb, Omar Yasser, Hamdy Shaban, Sameh T. Abu-Elela

TL;DR
This study compares quality of life and postoperative outcomes after hernia repair using fibrin glue versus tack fixation, finding better results with fibrin glue.
Contribution
The study introduces a comparison of fibrin glue and tack fixation in hernia repair focusing on quality of life and postoperative pain.
Findings
Fibrin glue group had shorter hospital stays and higher quality of life scores at 6 months.
No significant differences in postoperative complications like seroma or wound infection between the groups.
Operative time was longer for the tack group but not statistically significant.
Abstract
Mechanical methods are hypothesized to have postoperative pain and more seroma formation than non-mechanical methods due to tissue trauma. Therefore, the current prospective cohort study aimed to assess postoperative pain and quality-of-life (QoL) after fibrin glue versus tack mesh fixation. From July 2022 to December 2023, 80 patients sought TEP at the Suez Canal University Hospitals outpatient clinic. Participants were divided into two groups based on mesh fixation: the Fibrin glue group (FG) and the Tack group (TG). The purpose of this study was to compare the rate of post-operative complications, post-operative pain, length of hospital stays, and wound complications. In the meantime, the two groups QoL were compared using the SF-36 scoring questionnaire and the Caroline Comfort score (CCS). The patients in TG had higher operative time (84.5 ± 5.5 min) compared to patients in FG…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
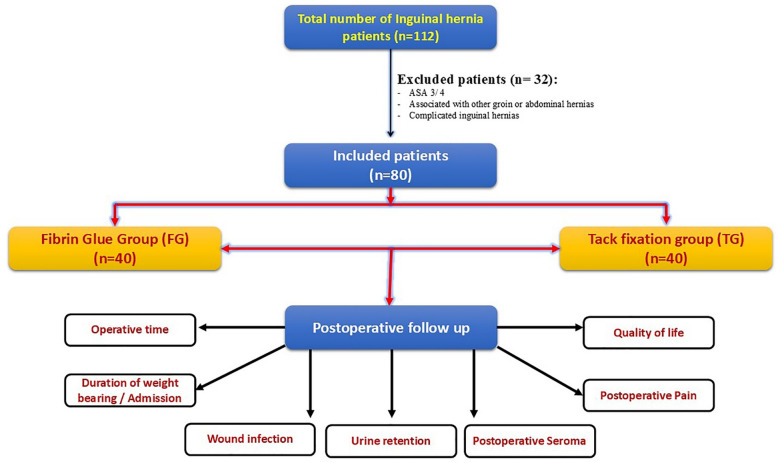 Figure 1
Figure 1- —Suez Canal University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHernia repair and management · Pelvic floor disorders treatments · Minimally Invasive Surgical Techniques
Introduction
Inguinal hernias are the most commonly presented abdominal hernias with approximately 20 million people operated on annually throughout the world. They are more commonly reported in young males, manual workers and in low socioeconomic population^1^. The advent of mesh was a breakthrough in the field of hernia surgery. A variety of meshes with variable physical and chemical properties are available for the repair of hernias^2^.Using prosthetic mesh materials, such as nonabsorbable polypropylene used in hernia repair have been known to cause physiological reactions causing pain and heaviness, whereas, recently used lightweight Prolene mesh has decreased pain and groin symptoms^3^. Furthermore, surgical techniques have evolved from open procedures to minimally invasive approaches and hernia repair has followed this same progression. Minimally invasive surgery has advantages of early postoperative recovery, lesser hospital stays, and early return to work. It is also associated with lesser postoperative pain due to smaller incisions with recurrence rates similar to open surgery^4^.A wide variety of mesh fixation techniques are available for laparoscopic hernia repair. These can be broadly divided into mechanical and nonmechanical methods^5^. Mechanical methods include sutures and tissue penetrating fixation devices like tackers. Nonmechanical techniques include self-gripping meshes and tissue adhesives (glues)^1^.
Mechanical methods are hypothesized to cause more postoperative pain and increased risk of seroma formation, hematoma formation, and osteitis pubis due to tissue trauma and also have increased risk of chronic pain due to nerve entrapment. On the other hand, nonmechanical methods do not have these disadvantages^6^.
Chronic pain following inguinal hernia repair has been reported in up to 53% of cases, with approximately 10% of patients experiencing worsened pain postoperatively. This burden is particularly notable in younger patients, those with severe preoperative pain, and in procedures involving heavyweight mesh and open techniques. While fibrin glue presents a promising solution, evidence evaluating its impact on postoperative quality of life remains limited^2,7,8^
Therefore, this study was designed to compare patient-reported outcomes following inguinal hernia repair using fibrin glue versus traditional tack mesh fixation, with a focus on postoperative pain and overall quality of life.
Patients and methods
Study design and setting
This is a prospective cohort study on patients who were presenting with uncomplicated inguinal hernia and scheduled for laparoscopic total extraperitoneal (TEP) hernioplasty at Suez Canal University Hospitals in the period of July 2022 to December 2023. Ethical approval for the study was obtained from the Institutional Review Board of Suez Canal University, Faculty of Medicine (code #4846/2022). The study was registered at the www.clinicaltrial.gov under number: NCT06679504.
Selection criteria and outcome measurement
Male patients underwent laparoscopic TEP repair were divided into Fibrin glue fixation (group A) and Tack fixation (group B). Patients aged between 18 and 60 years old, with inguinal hernia (direct (medial) or indirect (lateral) classified as M3 or L3 depending on the European Hernia society (EHS) classification^9^ and did not undergo hernia repair surgery before were included. According to the guidelines published^10,11^, inguinal hernia repair without fixing the mesh is recommended in almost all hernia types except when defect is larger than 3 cm in medial (direct) hernia [M3 fixation is recommended] and lateral (indirect) hernia [L3 fixation is preferred]. Meanwhile, patients who were unfit for general anesthesia or with American Society of Anesthesiologists (ASA) grade 3 and above, associated with other groin or abdominal hernias, recurrent, or complicated inguinal hernias, were excluded (Fig. 1). In tack mesh fixation, non-absorbable two tackers (one at Cooper’s ligament and another at the medially at the anterior abdominal wall) were used in all patients included in this group.
Fig. 1. Flow chart depicting the inclusion and exclusion approaches for the current study participants. ASA: american society of anesthesiologists.
The main outcome of the present study was to compare quality of life after laparoscopic totally extra peritoneal inguinal hernia repair with fibrin glue versus tack mesh fixation using SF-36 scoring questionnaire^12^ and Carolinas Comfort Scale (CCS)^13^. Furthermore, the postoperative pain has been compared between both groups using the Visual Analogue Scale (VAS) for pain assessment. (0–10, with 0 indicating no pain and 10 indicating the worst possible pain)
Sample size calculation
The sample size was determined using an online sample size calculator (http://www.raosoft.com/samplesize.html). The proportion of postoperative usage of analgesics among patients operated with laparoscopic TEP and tack fixation vs. fibrin glue fixation was considered 36% and 16%, respectively. According to the previous calculations, 71 patients were required. After accounting for a 10% drop-out, the total required sample size was 80 patients divided upon 2 groups, with the margin of error set at 5% and confidence level of 95%. At the same visiting day at the outpatient clinic, one of the researchers assigned the included patients to one of the study groups in successive manners starting by tack mesh group at a rate of 1:1.
Statistical analysis
Categorical variables were expressed as frequencies and percentages, while continuous variables were expressed as mean ± standard deviation (SD). Categorical variables were compared using Chi-Square or Fisher’s exact test. Continuous variables were compared using Student t-tests or Mann-Whitney test, as appropriate. All statistical analyses were performed using IBM SPSS software (Version 25.0. Armonk, NY: IBM Corp.). A p-value < 0.05 was considered significant.
Results
Characteristics of patients
A total of 80 patients were included in the present study (Fibrin glue group = 40 patients and Tack fixation group = 40 patients). The mean age of patients underwent laparoscopic TEP repair with fibrin glue and tack mesh fixation was 48.95 ± 8.49 and 48.12 ± 11.06 years respectively (P = 0.96). Overall, all patients included were males while diabetes was the most common chronic illness among the studied patients without statistical significance between both groups (P = 0.2) (Table 1).
Table 1. Basic demographic data of the studied group (N = 80).Fibrin glue group (n = 40)Tack mesh fixation group (n = 40)P-valueAge (years), mean ± SD48.95 ± 8.4948.12 ± 11.060.96BMI (kg\m2)24.4 ± 2.325.1 ± 3.50.302ASA grade _n, (%)_III34(85%)6(15%)33(82.5%)7(17.5%)0.98Gender n, (%) male40 (100%)40(100%)1OccupationEmployeeManual Worker15(37.5%)25(62.6%)13(32.5%)27(67.5%)0.87Marital statusMarriedSingle21(52.5%)19(47.5%)25(62.5%)15(37.5%)0.69Smoking statusCurrent smokerNon/ex-smoker23(57.5%)17(42.5%)25(62.5%)15(37.5%)0.68Chronic illnessDMHTNIHD6(15%)5(10%)1(0.5%)3(7%)3(7%)0(0%)0.21Type of herniaDirect (M3)Indirect (L3)12(30%)28(70%)13(32.5%)27(67.5%)0.90Occurrence of herniaPrimary40(100%)40(100%)1* Statistical significance at P < 0.05. BMI: Body Mass Index; DM: Diabetes Mellitus; HTN: Hypertension; IHD: Ischemic Heart Disease; M3: medial/direct hernia with defect > 3 cm; L3: lateral/indirect hernia with defect > 3 cm.
Comparing the postoperative outcome between fibrin glue vs. tack mesh fixation groups
The patients in tack mesh fixation group had higher operative time (84.5 ± 5.5 min) compared to patients in fibrin glue group (78.3 ± 6.4); however, there was no statistical significance (p = 0.21).
Furthermore, the fibrin glue group had statistically significant lower length of hospital stay (1.3 ± 0.3 days) compared to tack mesh group (1.8 ± 0.8 days) (p = 0.02) although the duration till initiation of weight bearing did not have statistical difference between both groups (2.28 ± 0.9 vs. 2.38 ± 1.3 days, respectively p = 0.09).
With following up patients for 30 days postoperative, Overall, there was no difference between both groups regarding the development of urinary retention, seroma or wound infection. (Table 2)
Table 2. Postoperative data of the studied group (N = 80).Fibrin glue group (n = 40)Tack mesh fixation group (n = 40)P-valueOperative time _(min)_78.3 ± 6.4[95%CI = 76.3–80.3]84.5 ± 5.5[95%CI = 82.8–86.2]0.21Duration till initiation of weight bearing _(days)_2.28 ± 0.9[95%CI = 2–2.6]2.38 ± 1.3[95%CI = 1.9–2.8]0.09Wound infection1(2.5%)2(5%)0.3Urinary retention3(7.5%)7(17.5%)0.09Seroma2(5%)3(7.5%)0.32Length of postoperative hospital stay (days)1.3 ± 0.3[95%CI = 1.2–1.4]1.8 ± 0.8[95%CI = 1.6–2.1] 0.02 ^*****^
- Statistical significance at P < 0.05.
With further follow up of the patients 6 months after surgery, for postoperative pain assessment, the patients in fibrin glue group had significantly lower visual analogue score (VAS) (1.48 ± 0.5) compared to patients in tack mesh fixation (5.7 ± 1.36) (p < 0.001). Furthermore, the fibrin glue group had a statistically significant higher overall quality of life score compared to tack mesh fixation group using both CCS and SF-36 questionnaire (P = 0.001 and 0.02; respectively) (Table 3).
Table 3. Postoperative pain and quality of life assessment (N = 80).Fibrin glue group (n = 40)Tack mesh fixation group (n = 40)P-valueVAS score1.48 ± 0.51[95%CI = 1.32–1.64]1.95 ± 0.82[95%CI = 1.69–2.2] 0.002 ^^ CCS score, Mean ± SD99 ± 7[95%CI = 96.8–101.2]105 ± 6[95%CI = 103.1–106.9] 0.001 ^^ SF-36 Questionnaire score (%), Mean ± SD79 ± 11[95%CI = 75.6–82.4]71 ± 17[95%CI = 65.7–76.3] 0.02 ^*****^
- Statistical significance at P < 0.05. CI: Confidence interval; VAS: Visual Analogue Scale; CCS: Caroline Comfort Score; SD: Standard deviation.
Discussion
The advent of laparoscopy brought new surgical approaches to inguinal hernia repair (IHR), and rigorous analysis comparing laparoscopic techniques to open has determined that the laparoscopic approach offers less postoperative pain, faster return to daily activities, and overall fewer complications^14^. Moreover, when compared to mechanical fixation procedures, fibrin glue mesh fixation has been linked to a reduced incidence of persistent postoperative inguinal discomfort and hematoma development after laparoscopic inguinal hernia repair, while retaining comparable recurrence rates^15,16^. This study aimed at decreasing morbidity and improving the quality of life of inguinal hernia patients through mesh fixation by fibrin glue instead of tack fixation. The present study participants were monitored for up to 30 days following surgery. The VAS, which measures pain, revealed a significant difference favoring the fibrin glue group (P = 0.002). As a result, the fibrin glue group outperformed the Tack mesh fixation group in terms of quality of life as measured by the CCS and SF-36 questionnaires (P = 0.001 and 0.02, respectively). Despite the fact that mesh hernioplasty has significantly decreased the likelihood of hernia recurrence, it is linked to the morbidity of chronic postoperative discomfort, which can significantly lower quality of life. Chronic discomfort after hernia repair has been attributed to a number of different etiologies.
In a recent meta-analysis, including 2312 patients from 18 randomized clinical trials (RCTs), Kitching et al. has reported that mesh fixation using fibrin glue has demonstrated superiority over tackers in minimizing postoperative pain and reducing the incidence of hematoma formation. These advantages contribute to faster recovery and earlier return to daily activities or work. Surgeons should consider these benefits during the informed consent process for laparoscopic inguinal and femoral hernia repair^17^. Several mechanisms have been proposed to explain the development of postoperative pain following tack mesh fixation. One avoidable cause of postoperative pain following tack mesh fixation is nerve entrapment during mesh placement, which can lead to neuropathic symptoms. Additionally, meshoma formation, a localized mesh-induced fibrosis, may incorporate adjacent nerves, contributing to persistent discomfort. It has also been hypothesized that mesh contraction over time may irritate surrounding nerve endings, exacerbating pain. In some patients, chronic inflammation triggered by the foreign body response to the mesh material further contributes to long-term discomfort and impaired quality of life^18,19^.
The severity of preoperative symptoms as assessed by the modified CCS is a strong predictor of reported postoperative complaints and is negatively correlated with the size of a direct defect, if one occurs. A CCS-based questionnaire specifically designed for hernias is being used for inguinal hernia repair in the preoperative and early postoperative stages for the first time, as far as we are aware. Of the 320 patients whose postoperative quality of life was assessed using the CCS comprehensive scoring technique, 55 and 38.1% were scored as “very satisfied” or “satisfied” at their initial visit, according to Berney et al. The patients’ satisfaction level rose even further at the second (6-week) visit, hitting 86.5 and 12.7%, respectively. The median and average scores for every group. Even though patients 50 years of age or younger had higher CCS scores than patients over 50, and the bilateral surgery group had higher CCS scores than the unilateral surgery group at both 2 and 6 weeks, the average and median scores in each group and at both time points were at least in the “satisfied” to “very satisfied” range^20^. This agrees with the results of a meta-analysis indicate a statistically significant reduction in chronic pain with the use of tissue glue fixation (OR 0.40; 95% CI 0.21–0.76; p = 0.005)^21^. Furthermore, findings were consistent with other studies, which demonstrated reduction in hypoesthesia in the tissue glue arm over the spiral tack arm (p = 0.045). However, another study did not show a difference in chronic pain in the ilioinguinal and genitofemoral areas using a VAS (p = 0.619)^22^.
Regarding operative data, we found that hospital stay, follow up time and duration till initiation of weigh bearing were shorter among fibrin glue group but with statistical insignificant differences (p > 0.05). When compared to the tacker group, the fibrin glue fixation group hospital stay lasted noticeably less. This can be explained by the fibrin glue group experiencing reduced discomfort and early patient mobilization. While the difference in weight-bearing initiation time did not reach statistical significance, this does not preclude its clinical relevance. Even modest improvements in early mobilization can impact patient comfort, rehabilitation speed, and discharge planning—especially in high-volume surgical settings. Therefore, interpreting outcomes should balance statistical metrics with practical, patient-centered implications.
Numerous trials comparing fibrin glue and tackers for mesh fixation revealed that the fibrin glue group required far less postoperative analgesics. Studies comparing fibrin glue fixation and sutures even in open hernia surgery showed that the fibrin glue group experienced less postoperative discomfort^23,24^.
Regarding the emergence of seroma or urine retention, there was no difference between the two groups, although it’s possible that the tackers produced more trauma than fibrin glue. A propensity score matched studies revealed no discernible difference between the fibrin glue and tacker groups in terms of postoperative problems such as hematoma, seroma, and urine retention According to some other researchers, however, the incidence of postoperative urinary retention was considerably higher in the tacker group than in the fibrin glue group, and it was connected with the quantity of tackers utilized^23,25,26^.
The current study identified some gaps in the body of knowledge on this subject, which may open the door for more research. More prospective randomized studies on the topic are required, ideally with controls for sex and age. It is necessary to examine if using varying amounts of fibrin glue causes any variations in long-term recurrence. Moreover, further researches comparing the absorbable tacker to other nonabsorbable fixing devices are also required.
Conclusion
Glue fixation may be effective in reducing the incidence of pain without increasing the risk of recurrence. Future research should consider both the effectiveness and cost-effectiveness of fixation techniques alongside the type of mesh and the size and location of the hernia defect.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bittner, R. et al. Guidelines for laparoscopic (TAPP) and endoscopic (TEP) treatment of inguinal hernia [International Endohernia Society (IEHS)]. Surgical endoscopy, 25(9): 2773–2843. (2011).10.1007/s 00464-011-1799-6PMC 316057521751060 · doi ↗ · pubmed ↗
- 2Patel, L.Y., Lapin, B., Gitelis, M.E., Brown, C., Linn, J.G., Haggerty, S., Denham, W., Butt, Z., Barrera, E., Joehl, R. and Carbray, J. Long-term patterns and predictors of pain following laparoscopic inguinal hernia repair: a patient-centered analysis. Surgical endoscopy, 31(5), 2109-2121.(2017).10.1007/s 00464-016-5207-027585467 · doi ↗ · pubmed ↗