Transformation and survival in patients with Waldenström macroglobulinemia: a population-based study
Yu Du, Xiaona Chang, Xiangxiang Li, Shugang Xing

TL;DR
This study finds that a small percentage of Waldenström macroglobulinemia patients transform to aggressive lymphoma, which significantly worsens survival.
Contribution
The study provides population-based insights into transformation risk and survival outcomes in Waldenström macroglobulinemia.
Findings
About 1.9% of patients transform to DLBCL within 10 years.
Transformation more than 24 months after diagnosis is linked to better survival.
Survival is worse for transformed DLBCL compared to de novo DLBCL.
Abstract
Waldenström’s macroglobulinemia (WM) is a rare hematologic neoplasm characterized by an indolent clinical course. However, a significant proportion of patients undergo histological transformation to aggressive diffuse large B-cell lymphoma (DLBCL). Long-term population-based data on the transformation and survival are scarce. Based on the Surveillance, Epidemiology, and End Results (SEER) database, we performed this study to estimate the risk of transformation and outcomes of patients with WM. 8191 patients with WM were retrieved from the SEER database. Competing risk methods were employed to evaluate the cumulative incidences and putative risk factors for transformation. Survival outcomes were analyzed using Kaplan-Meier and Cox proportional hazards regression. The cumulative incidence rates for transformation at 5 and 10 years were 1.0% (95% CI, 0.8%–1.3%) and 1.9% (95% CI,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
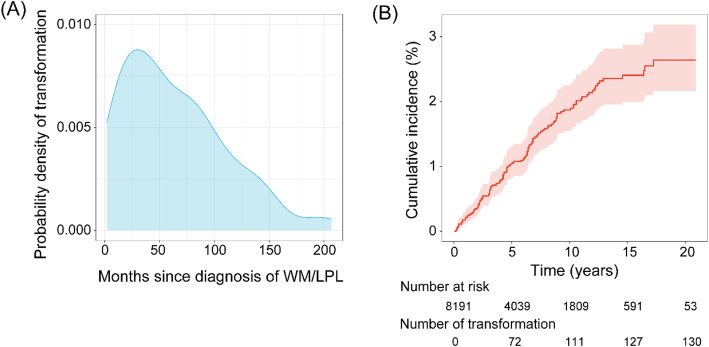 Figure 1
Figure 1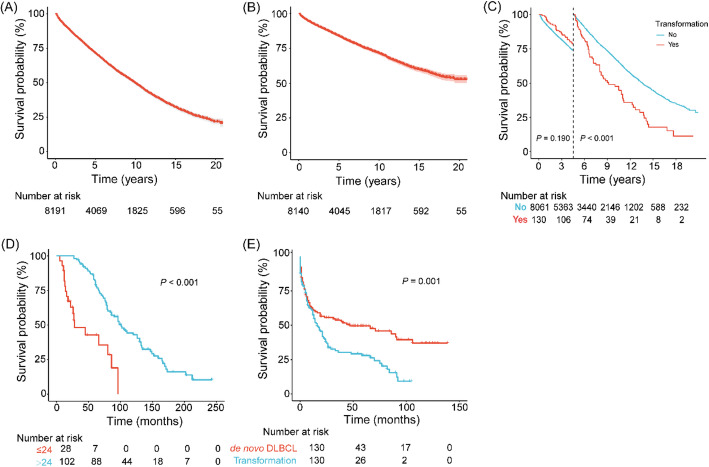 Figure 2
Figure 2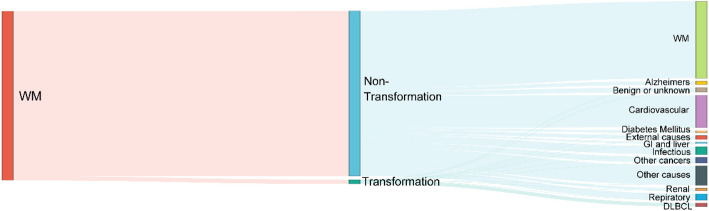 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Lymphocytic Leukemia Research · Chronic Myeloid Leukemia Treatments · Lymphoma Diagnosis and Treatment
Introduction
Lymphoplasmacytic lymphoma (LPL) represents an indolent yet incurable subtype of B-cell neoplasm, histopathologically distinguished by a heterogeneous proliferation of plasma cells, lymphoplasmacytoid cells, and small B lymphocytes. Waldenström macroglobulinemia (WM), a clinically significant subset of LPL, is defined by the concomitant presence of serum monoclonal immunoglobulin M (IgM) paraproteinemia and bone marrow infiltration by clonal lymphoplasmacytic cells, with approximately 95% of LPL cases meeting the diagnostic criteria for WM [1, 2]. Collectively, these entities constitute approximately 2% of all incident cases of non-Hodgkin lymphoma (NHL) at initial diagnosis, representing a relatively rare subset within the spectrum of lymphoid malignancies [3]. In light of the predominance of IgM-secreting LPL and given that WM represents the overwhelming majority of LPL cases, the nomenclature of WM will be adopted throughout this study to encompass both disease entities.
WM is generally characterized by an indolent clinical phenotype, typically associated with prolonged overall survival [4]. However, a subset of patients may experience an aggressive disease course. Histological transformation (HT) to higher-grade lymphoproliferative disorders, along with the development of secondary malignancies, have been established as independent prognostic determinants significantly correlated with adverse clinical outcomes in patients with WM [5–8]. Despite significant improvements in overall survival rates achieved through the sequential incorporation of rituximab-based immunotherapy and Bruton tyrosine kinase (BTK) inhibitors into the therapeutic armamentarium for WM, the clinical management of patients experiencing high-grade histological transformation continues to pose substantial therapeutic challenges and remains an area of unmet medical need [9, 10]. A significant limitation of existing literature [5, 6, 11, 12] investigating histological transformation in WM stems from the predominant reliance on small, single-institution patient cohorts, which may not be representative of the broader patient population. This methodological constraint has potentially led to incomplete characterization of the natural history of transformation, including its true incidence, associated clinical course, and long-term prognostic implications in the general WM population.
Diffuse large B-cell lymphoma (DLBCL) represents the most frequent histopathological variant observed in high-grade transformation events among patients with WM [7, 13]. Consequently, the present study will specifically focus on evaluating the risk of histological transformation to DLBCL and its prognostic impact on survival outcomes in patients with WM, utilizing comprehensive, population-level data derived from the Surveillance, Epidemiology, and End Results (SEER) program, a nationally representative cancer registry in the United States.
Methods
Patient selection
The SEER database gathers cancer data, including information on demographics and clinical features from population-based cancer registries. In this study, patients who were newly diagnosed with WM from January 2000 to December 2020, and were ≥ 18 years old were identified in the SEER database according to the International Classification of Diseases for Oncology,* Third Revision* (ICD-O-3) of the World Health Organization morphology codes 9671/3 and 9761/3. Cases without positive microscopic confirmation or positive laboratory test results, unknown survival data, or WM not identified as the first cancer were excluded from the study. Transformation from WM to DLBCL was diagnosed according to histologic confirmation, and cases demonstrating transformation within 2 months of WM diagnosis were not included in this study. DLBCL were identified using morphology code 9680/3. After the above-mentioned exclusions, 8191 patients with WM were found; 130 of them had transformation, and 3643 of them had died by the time the follow-up ended. For all patients, age at diagnosis, sex, race and ethnicity, Ann Arbor stage, months from diagnosis to treatment, treatment strategy, survival time and outcomes at the last follow-up, cause of death, year of diagnosis, and the interval from WM diagnosis to transformation were obtained. Patients were considered to have received deferred treatment if the interval between diagnosis and initial treatment was more than 3 months.
Statistical analysis
Distributions of clinical and demographic characteristics were compared utilizing either Chi-squared or Fisher’s exact test according to transformation status.
Using competing risk methods [14], the cumulative incidences of transformation were calculated, with death from any reason regarded to be the sole competing risk. The period to the first event was measured from the moment of WM diagnosis until the occurrence of transformation or mortality. Patients who had no events at the last follow-up were censored. The cumulative incidence curves of transformation were compared using Gray’s tests [15]. To assess the impact of various factors on transformation, the sub-distribution hazard ratio (SHR) along with their corresponding 95% confidence interval (CI) were calculated by fitting the Fine and Gray’s proportional sub-distribution hazard models [16]. The period from WM diagnosis until death is termed overall survival 1 (OS_1_), while the interval from disease transformation to death is defined as overall survival 2 (OS_2_). Disease-specific survival (DSS) was defined as the period between the initial diagnosis of WM and death attributable to WM. The Kaplan–Meier method was used to depict the OS and DSS curves, which were subsequently compared utilizing the log-rank tests. The impact of putative predictors on OS and DSS was assessed using univariate and multivariate Cox proportional hazard regression models.
A comparative study using case-matched analysis was carried out to evaluate the survival outcomes of patients whose DLBCL originated from a transformation of WM against those diagnosed with de novo DLBCL. Cases with DLBCL as the first malignancy were identified from the SEER database using the morphology code 9680/3. A 1:1 matching ratio was employed for patients with de novo DLBCL and those with transformation, based on age (± 2 years), sex, race, stage, B symptom presence, primary site, and year of diagnosis (± 2 years). The case-matched process was entirely random, disregarding factors such as the cause of death and survival status.
All statistical tests were two-sided, and differences with P < 0.05 were considered to be significant. The statistical analyses were conducted using STATA Release 16.0 (Stata-Corp LLC, College Station, TX, USA) and R version 4.2.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Characteristics of patients with WM
8191 patients diagnosed with LPL (3507 [42.8%])/WM (4684 [57.2%]) were included in this study (Table 1). At the time of diagnosis, the patients had a median age of 70 (range, 18–90 + years), with 63.5% being older than 65 years, and the male were a slight predominance (4830 [59.0%] male and 3361 [41.0%] female). Most of the patients were White (6796 [83.0%]). Excluding patients with an unknown stage, 86.1% of the patients were categorized as stage III/IV. A total of 312 (3.8%) patients had a deferred therapy. Chemotherapy was administered as a single modality in most patients (44.5%), followed by radiotherapy (1.4%), and a combined modality (0.8%). The remaining patients received no or unknown treatments (53.3%).
Table 1. Clinical characteristics of patients with WMVariable and CategoryTotalNon-transformationTransformation P No.%No.%No.%Total No. of patients8191100.0806198.41301.6Histology0.513LPL350742.8345598.5521.5WM468457.2460698.3781.7Age at diagnosis, years0.397≤ 65298636.5293498.3521.7> 65520563.5512798.5781.5Sex0.906Male483059.0475498.4761.6Female336141.0330798.4541.6Race and Ethnicity0.394NHW679683.0668798.41091.6NHB3734.636898.751.3NHAIAN220.32210000NHAPI4555.644497.6112.4Hispanic5456.754099.150.9Ann Arbor stage0.329Ⅰ2392.923799.220.8Ⅱ861.08497.722.3Ⅲ1201.511898.321.7Ⅳ188923.1185097.9392.1Unknown585771.5577298.5851.5Deferred therapy0.950Yes3123.830798.451.6No411250.2404598.4671.6Unknown376746.0370998.5581.5Treatment0.524^b^No treatment^a^436953.3430598.5641.50.344^c^CT only364744.5358498.3631.7RT only1121.411199.110.9CT + RT630.86196.823.2Year of diagnosis0.1132000–2010384747.0377798.2701.82011–2020434453.0428498.6601.4Abbreviations: CT, Chemotherapy; LPL, Lymphoplasmacytic lymphoma; NHAIAN, Non-Hispanic American Indian/Alaska Native; NHAPI, Non-Hispanic Asian or Pacific Islander; NHB, Non-Hispanic Black; NHW, Non-Hispanic White; RT, Radiotherapy; WM, Waldenström macroglobulinemia^a^The group with no treatment (no treatment, on active surveillance) included patients who had “unknown” chemotherapy or radiotherapy status. The Surveillance, Epidemiology and End Results database classifies chemotherapy (radiotherapy) data as “patients had chemotherapy (radiotherapy)” and “no/unknown”^b^No treatment, CT only, RT only, CT + RT^c^Any treatment vs. no treatment
Transformation to DLBCL
Histologically confirmed transformation to DLBCL was diagnosed in 130 (1.6%) patients. Most transformation events occurred within 10 years of WM diagnosis (85.4%, Fig. 1A). The median duration from the diagnosis of WM to its transformation was 54.5 months (range, 2–207 months). With 3552 deaths considered as a competing risk and 130 transformation events occurring after WM diagnosis, the cumulative incidence rates for transformation were 1.0% (95% CI, 0.8%–1.3%) at 5 years and 1.9% (95% CI, 1.5%–2.2%) at 10 years (Fig. 1B). The corresponding estimated annual incidence rate for transformation was 2.6 per 1000 patient-years (95% CI, 2.2–3.1 per 1000 patient-years) (Table S1).
Fig. 1. Transformation in patients with Waldenström macroglobulinemia. (A) Probability density curve of transformation; (B) Cumulative incidence of transformation for the entire cohort with corresponding 95% confidence intervals
The results obtained from the univariate Fine and Gray’s proportional subdistribution hazards models for transformation were presented in Table 2. However, this investigation did not identify any statistically significant clinical or demographic factors demonstrating a substantial association with the risk of histological transformation in the studied cohort (Figure S1).
Table 2. Univariate analyses for risk factors of transformation, DSS, and OS_1_Variable and categoryTransformationDSSOS_1_SHR (95% CI) P HR (95% CI) P HR (95% CI) P Transformation (time dependent)Yes v NoNANA4.37 (3.49–5.46)< 0.001Age at diagnosis> 65 v ≤ 65 years0.93 (0.65–1.31)0.6612.40 (2.15–2.67)< 0.0013.28 (3.03–3.55)< 0.001SexFemale v Male1.01 (0.71–1.43)0.9590.83 (0.75–0.91)< 0.0010.84 (0.78–0.90)< 0.001Race and EthnicityHispanic Ref.
Ref.
Ref. NHW1.65 (0.67–4.04)0.2800.98 (0.81–1.20)0.8740.87 (0.76–0.99)0.038NHB1.32 (0.38–4.55)0.6700.86 (0.64–1.16)0.3190.84 (0.69–1.03)0.089NHAIANNANA1.74 (0.85–3.57)0.1310.96 (0.51–1.81)0.906NHAPI2.61 (0.91–7.50)0.0750.98 (0.74–1.29)0.8760.87 (0.72–1.05)0.136Ann Arbor stageⅠ-Ⅱ Ref.
Ref.
Ref. Ⅲ-Ⅳ1.72 (0.61–4.81)0.3031.22 (0.96–1.55)0.1101.19 (1.02–1.39)0.027Missing1.64 (0.60–4.49)0.3371.23 (0.97–1.55)0.0871.04 (0.89–1.20)0.650Deferred therapyYes Ref.
Ref.
Ref. No1.01 (0.41–2.52)0.9761.41 (1.09–1.83)0.0091.30 (1.08–1.56)0.005Unknown0.92 (0.37–2.31)0.8640.96 (0.74–1.25)0.7631.11 (0.93–1.33)0.259Treatment^a^Yes v No/Unknown1.15 (0.82–1.63)0.4181.51 (1.37–1.66)< 0.0011.14 (1.07–1.22)< 0.001Abbreviations: CI, Confidence interval; DSS, Disease-specific survival; HR, Hazard ratio; NA, Not available; NHAIAN, Non-Hispanic American Indian/Alaska Native; NHAPI, Non-Hispanic Asian or Pacific Islander; NHB, Non-Hispanic Black; NHW, Non-Hispanic White; OS, Overall survival; SHR, Subdistribution hazard ratio; WM, Waldenström macroglobulinemia^a^Patients who have undergone at least one treatment regimen are compared to those who have received no treatment or whose treatment status is unknown
Survival and effect of transformation on OS
There were 3643 deaths during the 50,867 patient-years of follow-up (mortality rate, 71.6 per 1000 patient-years). The median OS_1_ was 119 months (95% CI, 115–123 months), whereas median DSS was not reached. The 5- and 10-year OS_1_ rates were 71.2% (95% CI, 70.2%–72.3%) and 49.5% (95% CI, 48.2%–50.9%), respectively (Fig. 2A). The 5- and 10-year DSS rates were 83.8% (95% CI, 82.9%–84.7%) and 71.4% (95% CI, 70.1%–72.8%), respectively (Fig. 2B).
Fig. 2. Kaplan–Meier curves for survival in patients with Waldenström macroglobulinemia. (A) OS_1_; (B) DSS; (C) OS_1_ for patients with and without transformation; (D) OS_1_ for patients with early and late transformation; (E) OS_2_ for patients with de novo DLBCL and those with DLBCL transformed from WM. DLBCL, diffuse large-B cell lymphoma; DSS, disease-specific survival; OS, overall survival
Patients exhibiting transformation demonstrated a significantly shorter OS_1_ compared to those without transformation (10-year rate, 37.3% [95% CI, 29.2%–47.6%] v 49.8% [95% CI, 48.5%–51.2%], respectively; P < 0.001; Fig. 2C). Furthermore, patients whose transformation occurred more than 24 months after the initial diagnosis of WM exhibited a longer OS_1_ compared to those whose transformation took place within 24 months (5-year OS_1_ rates, 81.9% [95% CI, 74.7%–89.9%] v 42.7% [95% CI, 26.4%–69.2%], respectively; P < 0.001; Fig. 2D). The multivariate Cox proportional hazards regression indicated that time-dependent transformation was an independent predictor of decreased OS_1_ (HR, 4.21 [95% CI, 3.36–5.26], P < 0.001). As shown in Table 3, multivariate analyses incorporating significant individual variables also revealed that aged >65 years and males demonstrated statistically significant predictors of shorter DSS and OS_1_ (Figure S2 and S3). In this study, treatment might be associated with poorer DSS and OS_1_, most likely due to the fact that patients who underwent treatment initially presented with more aggressive disease and those without treatment were asymptomatic or minimally symptomatic [17].
Table 3. Multivariate analyses for risk factors of DSS and OS_1_ in patients with WMVariable and categoryDSSOS_1_HR (95% CI) P HR (95% CI) P Transformation (time dependent)Yes v NoNA4.21 (3.36–5.26)< 0.001Age at diagnosis> 65 v ≤ 65 years1.06 (1.05–1.06)< 0.0013.40 (3.14–3.68)< 0.001SexFemale v Male0.78 (0.71–0.86)< 0.0010.80 (0.75–0.86)< 0.001Race and EthnicityHispanicNHW0.82 (0.72–0.94)0.003NHB1.06 (0.87–1.28)0.592NHAIAN1.09 (0.58–2.05)0.786NHAPI0.82 (0.68–0.99)0.043Ann Arbor stageⅠ-ⅡⅢ-Ⅳ1.16 (0.99–1.36)0.062Missing1.02 (0.88–1.19)0.797Deferred therapyYesNo1.43 (1.10–1.85)0.0071.28 (1.06–1.53)0.008Unknown1.25 (0.94–1.67)0.1261.11 (0.91–1.36)0.311TreatmentYes v No/Unknown1.59 (1.37–1.86)< 0.0011.13 (1.01–1.25)0.029Abbreviations: CI, Confidence interval; DSS, Disease-specific survival; HR, Hazard ratio; NA, Not available; NHAIAN, Non-Hispanic American Indian/Alaska Native; NHAPI, Non-Hispanic Asian or Pacific Islander; NHB, Non-Hispanic Black; NHW, Non-Hispanic White; OS, Overall survival; WM, Waldenström macroglobulinemia
Characteristics of the 130 patients with DLBCL transformed from WM were summarized in Table 4. With a median age of 74 years (range, 48–90 + years), 21 of 77 (27.3%) patients exhibited B symptoms at transformation. 33 of 62 patients (53.2%) had stage Ⅲ to Ⅳ disease, and extranodal involvement was present in 41.5%. The most frequent site of extranodal involvement were bone marrow (9.2%), central nervous system (8.5%), gastrointestinal tract (6.2%), lungs (3.8%), and skin (3.8%).
Table 4. Characteristics of patients with DLBCL transformed from WMCharacteristics N %Age (median, range), years74 (48–90+)Sex (M/F)76/5458.5/41.5RaceWhite11487.7Black53.8Other118.5SiteExtranodal5441.5Nodal7658.5StageⅠ1914.6Ⅱ107.7Ⅲ64.6Ⅳ2720.8Unknown6852.3B symptomYes2116.2No5643.1Unknown5340.8Primary siteGastrointestinal tract86.2Lung53.8Skin53.8CNS118.5Bone marrow129.2Lymph node7658.5Other1310.0SurvivalAlive3930.0Dead9170.0Abbreviations: CNS, Central nervous system; DLBCL, Diffuse large B-cell lymphoma; F, Female; M, Male; WM, Waldenström macroglobulinemia
Among the 130 patients who underwent transformation, 39 survived and 91 died at the time of the last follow-up. The median OS_2_ was 16 months (95% CI, 12–23 months), and the OS_2_ rates were 37.8% (95% CI, 29.8%–47.9%) and 28.0% (95% CI, 20.5%–38.1%) at 2 years and 5 years, respectively (Fig. 2E). Comparative survival analysis revealed significantly inferior survival outcomes in patients with WM-transformed DLBCL when compared to matched cases of de novo DLBCL with comparable clinicopathological characteristics (5-year OS_2_ rates, 28.0% [95% CI, 20.5%–38.1%] v 49.5% [95% CI, 41.2%–59.4%], respectively; P = 0.001; Fig. 2E).
Causes of death
During the study period, there were 3,643 deaths. The causes of death were illustrated in Fig. 3. Of these, 1,654 (45.4%) were attributed to WM, and 190 (5.2%) to secondary malignancies. Other leading causes of death included cardiovascular diseases (698, 19.2%), followed by infectious (166, 4.6%) and respiratory diseases (137, 3.8%). Of the 91 deaths among patients experiencing transformation, 74 (81.3%) were attributed to DLBCL.
Fig. 3. Sankey diagram shows the proportion of causes of death. DLBCL, diffuse large-B cell lymphoma; GI, Gastrointestinal; WM, Waldenström macroglobulinemia
Discussion.
As far as we know, this study based on population is the largest to investigate transformation in patients diagnosed with WM. Data from 8191 patients were examined, with a median follow-up of 107 months, during which 130 histologically confirmed transformations were diagnosed. The cumulative incidence rates for transformation were 1.0% at 5 years and 1.9% at 10 years. Compared with patients who did not experience transformation, transformation resulted in a significantly higher mortality rate. Additionally, we found that the OS was shorter for individuals with DLBCL transformed from WM than for those with de novo DLBCL.
In the present study, the cumulative incidence rates of transformation at 5-year and 10-year were 1.0% and 1.9%, respectively. A retrospective single-center study involving 1466 patients reported a cumulative incidence of transformation of 1.0% at 5 years and 2.4% at 10 years, similar to our results [5]. However, in another retrospective analysis by Zanwar et al. [18], the 5- and 10-year cumulative incidence rates of transformation was 2.4% and 4.7%, respectively, which were higher than those in our study. This observation may be attributed to the fact that the development of aggressive non-Hodgkin lymphoma (NHL) subtypes concurrent with WM was classified and analyzed as histological transformation events within the framework of this investigation.
The development of reliable predictive biomarkers for identifying patients with WM at elevated risk of histological transformation represents a critical unmet need in clinical practice; however, current evidence remains limited due to insufficient cohort sizes and lack of comprehensive molecular profiling in existing studies. In a study by Zanwar et al. [18], multivariate analysis showed that the sole independent predictor of transformation was MYD88^WT^ status. Another study also observed that patients with the MYD88^WT^ genotype were at an increased risk of transformation (HR, 19.8) [11]. According to Leleu et al. [19], purine analogs have been linked to a higher risk of transformation and emergence of myelodysplasia or acute myeloid leukemia. Conversely, no differences in transformation were found in a study comparing fludarabine and chlorambucil [20]. Consistent with our findings, the investigation conducted by Lin et al. [7] similarly failed to identify statistically significant clinical or molecular predictors associated with the risk of histological transformation in their study cohort, further highlighting the methodological challenges and knowledge gaps in this area of research. The current investigation was limited by insufficient documentation of clinicopathological characteristics in the WM cohort, which precluded comprehensive risk stratification and multivariate analysis of potential transformation predictors. These methodological constraints underscore the necessity for future large-scale, prospective studies incorporating detailed molecular profiling and standardized clinical data collection to elucidate the complex interplay of factors associated with histological transformation risk.
In accordance with previous reports, OS_1_ was worse for patients with WM who experience transformation than for those who did not. Castillo et al. [5] reported a much shorter median OS_1_ in patients with transformation than in those without transformation (8.7 vs. 16 years). With transformation as a time-dependent covariate, patients who experienced transformation exhibited a significantly higher risk (HR, 5.075) for death than those who did not experience transformation in a study by Zanwar et al. [18]. Additionally, we found that individuals with transformation occurring >24 months after WM diagnosis had higher OS rates than those with transformation occurring within 24 months. Similar findings were also reported in high-grade transformations of follicular lymphoma [21, 22] and marginal zone lymphoma [23, 24].
Using a case-control matching method, we observed that patients with de novo DLBCL had higher OS_2_ rates compared to those with DLBCL transformed from WM. Similar finding was reported by Castillo et al. [8]. Possible explanations for this finding include differences in disease biology and treatment regimens [25]. Another factor to consider is that most clinical trials designed for WM or de novo DLBCL do not include individuals with transformations.
In our study, we found that patients with DLBCL transformed from WM presented with a high rate of extranodal disease (41.5%), and the bone marrow (9.2%) was the main site, followed by central nervous system (CNS) (8.5%), gastrointestinal tract (6.2%), lungs (3.8%), and skin (3.8%). The finding was consistent with what Durot et al. reported [6]. Previous studies have demonstrated a correlation between the MYD88 L265P mutation and extranodal involvement in patients with de novo DLBCL [26–28]. And, a hallmark of WM is MYD88 L265P mutation [29], which may facilitate the localization of tumor cells to extranodal sites in transformed WM.
Advantages of the current study comprise its population-based design and use of SEER data spanning a 21-year period. However, we acknowledge that some limitations should be addressed. First, the study design precluded a central pathology review, which may have led to potential misclassifications. Second, the absence of detailed individual-level treatment data impeded our ability to elucidate the relationship between treatment and transformation. Finally, it is possible that in a small percentage of cases, the DLBCL component did not arise from a real histological transformation, but rather developed de novo.
In conclusion, the 10-year cumulative incidence rate for transformation to DLBCL in patients with WM was 1.9%. A significantly higher risk of death was linked to transformation to DLBCL, and the results appeared to be worse than those in the general population when DLBCL developed de novo. Despite comprehensive analysis, this study did not identify statistically significant risk factors associated with histological transformation. These findings underscore the critical need for future investigations incorporating advanced molecular profiling and larger, multicenter cohorts to establish reliable predictive biomarkers for transformation susceptibility, elucidate the underlying molecular mechanisms driving transformation, and develop targeted therapeutic strategies to improve clinical outcomes and survival rates in this high-risk patient population.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1