Affective disorders—developments of ICD-11 in comparison with ICD-10
Martin Härter, Frank Schneider

TL;DR
This paper compares ICD-11 updates for diagnosing affective disorders with ICD-10, highlighting structural and content changes.
Contribution
The paper provides a detailed comparison of diagnostic criteria for affective disorders between ICD-11 and ICD-10.
Findings
ICD-11 groups depressive symptoms into clusters and distinguishes partial from complete remission.
Bipolar disorder is now divided into type I and II, with manic episodes not being diagnosable independently.
Dysthymia is reclassified as a depressive disorder and cyclothymia as a bipolar disorder in ICD-11.
Abstract
With the introduction of the 11th revision of the World Health Organization (WHO) “International Statistical Classification of Diseases and Related Health Problems” (ICD-11), structural and content-related adjustments were made to the diagnostic guidelines for affective disorders, which are presented in this review article. The update has resulted in some changes to the diagnostic classification of affective disorders, based on the American Diagnostic and Statistical Manual of Mental Disorders 5 (DSM-5). The ICD-11 assigns depressive symptoms to so-called clusters, the main symptoms of depressed mood and joylessness can be accompanied by cognitive, behavioral or neurovegetative symptoms. In the case of remission of depressive episodes, the ICD-11 distinguishes between partial and complete remission. A persistent depressive disorder is present if the depressive episode lasts continuously…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
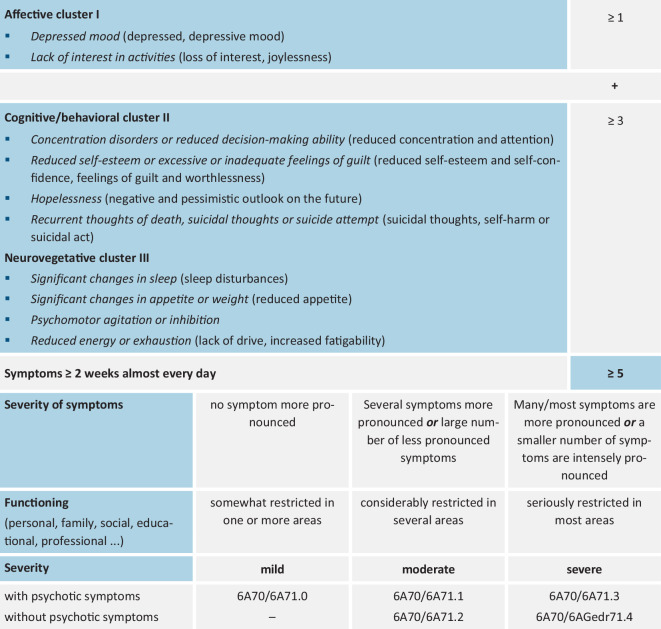 Figure 1
Figure 1 Figure 2
Figure 2- —Universitätsklinikum Düsseldorf. Anstalt öffentlichen Rechts (8911)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMental Health and Psychiatry · Personality Disorders and Psychopathology
Background
Affective disorders are a group of disorders whose main characteristics are a change in mood, usually in phases, toward the depressive or manic pole and a change in energy. Bipolar affective disorders, in which hypomanic or manic as well as depressive or mixed episodes with more or less symptom-free intervals occur, are to be distinguished from unipolar depressive courses.
The aim of this article is to provide a concise and clear presentation of the changes in the classification of affective disorders in the transition from the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) to ICD-11. On the one hand, the taxonomic classification of depressive and bipolar disorders is presented in tabular form, and on the other hand, specific information on the diagnosis of depressive disorders is given. For more detailed information, reference is made to the corresponding classification systems of the comprehensive disease categories including their specifics, available from the Federal Institute for Drugs and Medical Devices (BfArM)1^,^2.
Changes in the taxonomy of affective disorders in the transition from ICD-10 to ICD-11
The transition from ICD-10 to ICD-11 resulted in the following structural changes (see also [1–7]):
In addition to the classification into unipolar and bipolar courses, episodic affective disorders, i.e., manic (Chaps. F30–31) or depressive episodes (Chaps. F.32–33), were distinguished from chronic persistent affective disorders (dysthymia, cyclothymia) in ICD-10 (Chap. F.34). In addition, there were the residual categories “Other affective disorders” (Chap. F.38) and “Affective disorder not otherwise specified” (Chap. F.39).
The diagnosis of affective disorders remains categorical in principle in ICD-11, but the extent of operationalization (i.e., counting symptoms) has been reduced in favor of a clinical assessment with the central criteria of symptom severity and functional impairment. The concept of persistent affective disorders of ICD-10 is abandoned in ICD-11; dysthymia is assigned to depressive disorders and cyclothymia to bipolar disorders.
In ICD-11, the differentiation of depressive symptoms into three symptom clusters, a dimensional assessment of severity, and a greater degree of freedom for clinical professionals in the diagnosis of affective disorders are realized (see Fig. 1). In addition, the additional coding “with psychotic symptoms” also exists for moderate depressive episodes. In the case of currently remitted depressive episodes, ICD-11 also distinguishes between *partial *and complete remission.Fig. 1. Diagnostic guidelines (ICD-11): depressive disorder with single episode or recurrent depressive disorder (symptoms/criteria of ICD-10 in parentheses)
“Premenstrual dysphoric disorder” and “Mixed depressive disorder and anxiety disorder” are included as new categories.
After the first manifestation of a depressive episode, the majority of patients (55–65%) experience several depressive phases over the course of their lives (recurrent depressive disorder). The risk of relapse increases with each subsequent depressive episode. In addition, as the number of episodes increases and with increasing age, the intervals between depressive phases and recurrent depressive disorder become shorter (see taxonomy of recurrent depression; ICD-10 vs. CD-11, Table 1).Table 1. Taxonomy of depressive disorders in ICD-10 and ICD-11ICD-10ICD-11 (draft version)Affective disorders (F30–31)**Affective disorders (6A60.X–6A73.X)F32.—Depressive episode6A70 Single-episode depressive disorderF32.0 Mild depressive episode6A70.0 Single-episode depressive disorder, mildF32.1 Moderate depressive episode6A70.1 Single-episode depressive disorder, moderate, without psychotic symptoms6A70.2 Single-episode depressive disorder, moderate, with psychotic symptomsF32.2 Major depressive episode without psychotic symptoms6A70.3 Single-episode depressive disorder, severe, without psychotic symptomsF32.3 Depressive disorder, current major episode with psychotic symptoms6A70.4 Single-episode depressive disorder, severe, with psychotic symptomsF32.4 Depressive disorder, currently remitted6A70.6 Depressive disorder with single episode, currently in partial remission6A70.7 Depressive disorder with single episode, currently in full remissionF32.8 Other depressive episodesAtypical depression6A8Y Other specified affective disordersF32.9 Depressive episode, unspecified6A8Z Affective disorders, unspecifiedF33.—Recurrent depression6A71 Recurrent depressive disorderF33.0 Recurrent depressive disorder, currently mild episode6A71.0 Recurrent depressive disorder, current mild episodeF33.1 Recurrent depressive disorder, current moderate episode6A71.1 Recurrent depressive disorder, current moderate episode, without psychotic symptoms6A71.2 Recurrent depressive disorder, current moderate episode, with psychotic symptomsF33.3 Recurrent depressive disorder, current major episode without psychotic symptoms6A71.3 Recurrent depressive disorder, current severe episode, without psychotic symptomsF33.3 Recurrent depressive disorder, current major episode with psychotic symptoms6A71.4 Recurrent depressive disorder, current major episode, with psychotic symptomsF33.4 Recurrent depressive disorder, currently remitted6A71.6 Recurrent depressive disorder, currently in partial remission6A71.7 Recurrent depressive disorder, currently in full remissionF33.8 Other recurrent depressive disorder6A71.Y Other specified recurrent depressive disorderF33.9 Recurrent depressive disorder, unspecified6A71.Z Recurrent depressive disorder, unspecifiedF34.—Persistent affective disorders–F34.1 Dysthymia6A72 Dysthymic disorderF34.8 Other persistent affective disorders–F34.8 Persistent affective disorder, unspecified–New categories–F41.2 Anxiety and depressive disorder, mixed6A73 Mixed depressive and anxiety disorder–GA34.41 Premenstrual dysphoric disorder*ICD *International Statistical Classification of Diseases and Related Health Problems
In future, bipolar disorder will be divided into type I and type II. Manic episodes can still only be coded in the context of bipolar disorders and cannot be diagnosed as an independent, separate disorder (see Table 2).Table 2. Taxonomy of bipolar disorders in ICD-10 and ICD-11ICD-10ICD-11 (draft version)Affective disorders (F30–39)**Affective disorders (6A60.X–6A61.X)F30.—Manic episode6A60 Bipolar disorder type IF30.0 Hypomania6A60.2 (or 6A61.2) Bipolar disorder type I (or type II), current hypomanic episodeF30.1 Mania without psychotic symptoms6A60.0 Bipolar disorder type I, current manic episode, without psychotic symptomsF30.2 Mania with psychotic symptoms6A60.1 Bipolar disorder type I, current manic episode, with psychotic symptomsF30.8 Other manic episodes6A8Y Other specified affective disordersF30.9 Manic episode, unspecified6A8Z Affective disorders, unspecifiedF31.—Bipolar affective disorder**6A60 Bipolar disorder type IF31.0 Bipolar affective disorder, current hypomanic episode6A60.2 (or 6A61.2) Bipolar disorder type I (or type II), current hypomanic episodeF31.1 Bipolar affective disorder, current manic episode without psychotic symptoms6A60.0 Bipolar disorder type I, current manic episode, without psychotic symptomF31.2 Bipolar affective disorder, current manic episode with psychotic symptoms6A60.1 Bipolar disorder type I, current manic episode, with psychotic symptomsF31.3 Bipolar affective disorder, current mild or moderate depressive episode6A60.3 Bipolar disorder type I, current mild depressive episode6A60.4 Bipolar disorder type I, current moderate depressive episode, without psychotic symptomsF31.4 Bipolar affective disorder, current major depressive episode without psychotic symptoms6A60.6 Bipolar disorder type I, current major depressive episode, without psychotic symptomsF31.5 Bipolar affective disorder, current major depressive episode with psychotic symptoms6A60.7 Bipolar disorder type I, current major depressive episode, with psychotic symptomsF31.6 Bipolar affective disorder, current mixed episode6A60.9 Bipolar disorder type I, current mixed episode, without psychotic symptoms6A60.A Bipolar disorder type I, current mixed episode, with psychotic symptomsF31.7 Bipolar affective disorder, currently remitted6A60.F Bipolar disorder type I, currently in full remissionF31.8 Other bipolar affective disorder6A60.Y Other specified bipolar disorder type IF31.9 Bipolar affective disorder, unspecified6A60.Z Bipolar disorder type I, unspecified*–*6A61 Bipolar disorder type II–6A61.0 Bipolar disorder type II, current hypomanic episode–6A61.1 Bipolar disorder type II, current mild depressive episode–6A61.2 Bipolar disorder type II, current moderate depressive episode, without psychotic symptoms–etc.F34.—Persistent affective disorders–F34.0 Cyclothymia6A62 Cyclothymic disorderF34.8 Other persistent affective disorders–F34.9 Persistent affective disorder, unspecified–*ICD *International Statistical Classification of Diseases and Related Health Problems, etc. Continue coding as for bipolar disorder type I to 6A61.Z bipolar disorder type II, unspecified
To capture inter-individual differences, depressive or manic episodes can be additionally coded with so-called qualifiers (6A80*) (analogous to the “specifiers” of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition [DSM-5]), e.g., with regard to accompanying anxiety syndromes, a chronic course, a seasonal pattern, or in relation to the peripartum period [4]. In the ICD-11, it is possible to code further clinical manifestations in addition to the affective core diagnosis of “depression” or “bipolar disorder”, e.g., “with marked anxiety symptoms” (6A80.0); “with panic attacks” (6A80.1); “with persistent symptoms,” i.e., at least 2 years (= possibility of coding chronic depression that goes beyond dysthymia; 6A80.2); “with melancholia” (6A80.3, which was coded as “somatic syndrome” in ICD-10); “with seasonal onset” (6A80.4); or “with rapid cycling” (6A80.5).
Diagnosis of depressive episodes
To diagnose a depressive episode, at least five symptoms must be present (four were sufficient in ICD-10), at least one of which must be from the affective cluster. The classification of episode severity (mild, moderate, severe) is—unlike in the ICD-10—not based on the sum of the symptoms, but also takes into account their intensity and the degree of functional impairment in addition to the number of symptoms. The grouping of depression symptoms is intended to illustrate the wide clinical range of symptoms and increases clarity. Cluster I contains the two so-called entry-level symptoms. This no longer includes the less specific symptom “lack of energy, increased fatigability,” which now belongs to Cluster III as “reduced energy or exhaustion.”
Concluding remarks
It is to be hoped that the new ICD-11 will be met with widespread acceptance once it has been introduced into healthcare in Germany. Although the coding will be more differentiated and, if necessary, more detailed, this also corresponds to the general efforts to achieve even greater personalization with regard to the treatment strategies to be used. The greater emphasis on the dimensionality of disorders, e.g., with regard to functional impairment and severity, can contribute to the fact that, in addition to the clinical reduction of symptoms, the improvement of functional limitations and quality of life in particular will become more important as therapeutic goals.
Practical conclusion
- In the case of transient depressive moods, which are very common in the general population, it makes sense to differentiate them from depressive disorders by assessing the severity of symptoms and functional limitations.
- The grouping or clustering of depressive symptoms is useful due to the clinical breadth of the symptomatology and it increases clarity.
- The addition of persistent or chronic depression was overdue and was already frequently used in everyday clinical practice.
- The addition of the “qualifiers” to the classification makes clinical sense, as numerous symptoms such as anxiety, panic, persistence, seasonal pattern, or melancholy are common and useful for treatment planning.
- The abandonment of the coding of individual manic episodes is logical, as the separation was not well documented in the context of family, therapy, and follow-up studies.
- The independent coding of bipolar disorder type 2 is welcome, since study findings support this view and the prognosis and response to treatment are usually more favorable.
- The resolution of the persistent affective disorders and the classification in the respective chapters of depressive and bipolar disorders is particularly helpful because of the similar treatment strategies; in addition, clinical courses with transitions are often found in these subcategories.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization (WHO) (2019) International classification of diseases, eleventh revision (ICD-11). https://icd.who.int/browse 11 (Licensed under Creative Commons Attribution-No Derivatives 3.0 IGO licence (CC BY-ND 3.0 IGO))