Reduced splenic volume and advanced age predict sepsis in patients with Howell–Jolly bodies: a retrospective cohort study
Kaori Uchino, Yuya Nakagami, Megumi Enomoto, Nozomi Shimizu, Kenichi Kondo, Takahiro Yamamoto, Yukie Sugita, Yuto Isaji, Sakura Saigusa, Yusuke Iida, Saki Shinohara, Tomohiro Horio, Satsuki Murakami, Shohei Mizuno, Kazuhiro Ikegame, Ichiro Hanamura, Akiyoshi Takami

TL;DR
This study finds that older age and smaller spleen size in patients with Howell-Jolly bodies increase the risk of sepsis.
Contribution
The study identifies reduced splenic volume and advanced age as independent predictors of sepsis in non-splenectomized patients with Howell-Jolly bodies.
Findings
Age ≥ 65 years and spleen volume < 34 mL independently predict sepsis in patients with Howell-Jolly bodies.
Computed tomography-based spleen volume measurements can help identify functional hyposplenism.
Older age also predicts any infection, while low spleen volume shows a trend toward significance.
Abstract
Functional hyposplenism, defined as impaired splenic function in the absence of splenectomy, increases susceptibility to life-threatening infections. Although Howell–Jolly bodies (HJBs) are well-established markers for this condition, the predictive value of spleen volume for infection risk remains unclear. We retrospectively analyzed 95 non-splenectomized patients with HJBs from 2014 to 2024. We measured spleen volume by computed tomography and compared results with ideal values. We evaluated the associations between splenic volume and infections using univariate and multivariate logistic regression analyses. The median patient age was 66 years (range, 16−95); 72% were male. The median spleen volume was 34 mL, lower than the ideal median of 210 mL. Forty-eight percent of patients experienced at least one infection. Univariate analysis identified age ≥ 65 years and spleen volume < 34 mL…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
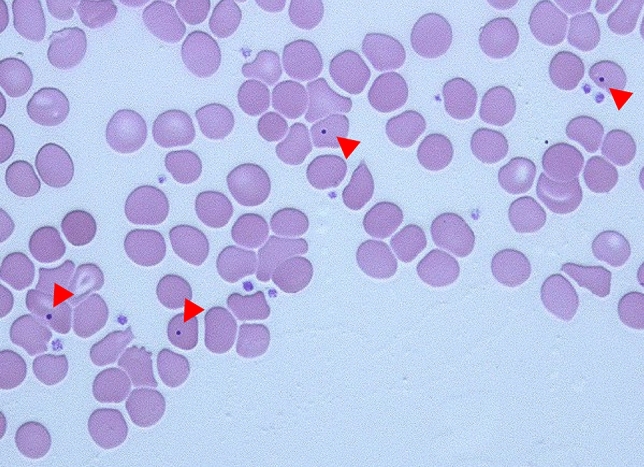 Figure 1
Figure 1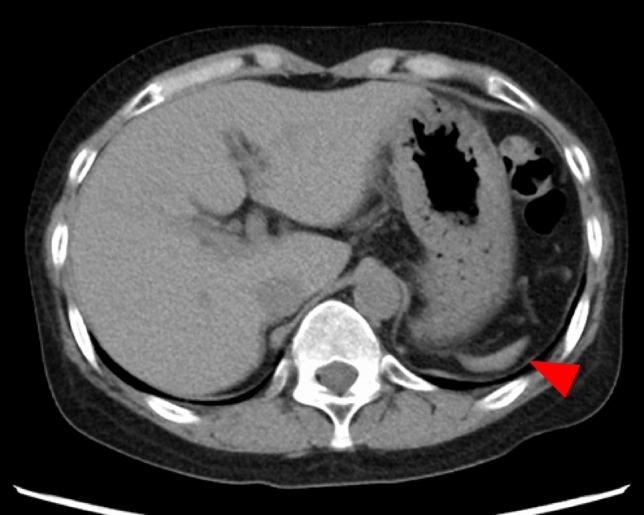 Figure 2
Figure 2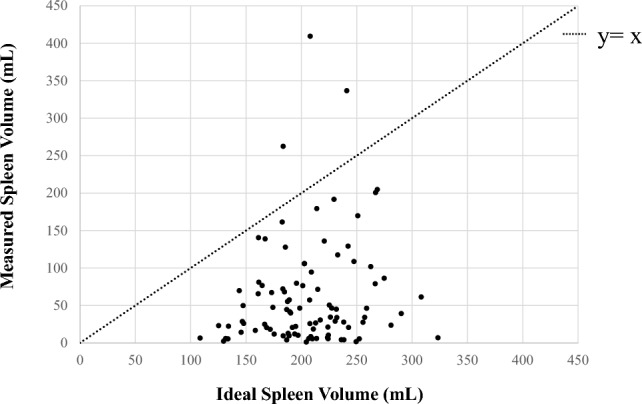 Figure 3
Figure 3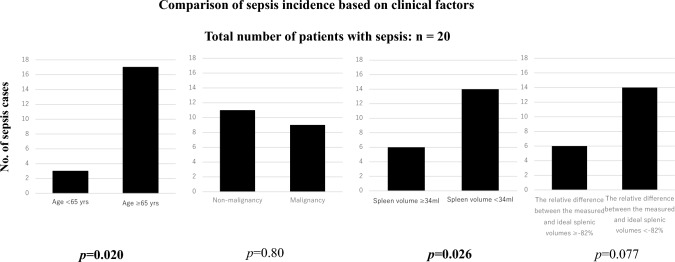 Figure 4
Figure 4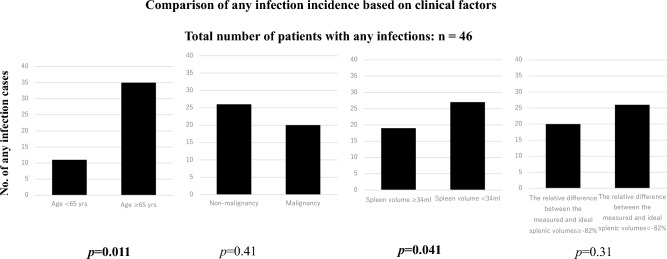 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal Trauma and Injuries · Pediatric Urology and Nephrology Studies · Autopsy Techniques and Outcomes
Introduction
Functional hyposplenism is characterized by impaired splenic function in individuals without prior splenectomy. This condition increases susceptibility to severe, occasionally fatal infections, especially by encapsulated bacteria such as Streptococcus pneumoniae, Haemophilus influenzae type b, and Neisseria meningitidis [1, 2]. Functional hyposplenism can result from diverse etiologies, including congenital abnormalities, gastrointestinal and autoimmune disorders, hematologic and non-hematologic malignancies, infections, and immunosuppressive therapies [3–6]. Moreover, aging, malignancy, and certain molecular-targeted therapies have emerged as contributing factors to functional hyposplenism.
Despite its clinical relevance, this condition is frequently underrecognized. Early detection is crucial for initiating preventive strategies, including appropriate vaccinations and prophylactic antibiotic administration [7, 8]. Under normal conditions, the spleen removes nuclear remnants from circulating erythrocytes without destroying the cells. When splenic function is impaired, Howell–Jolly bodies (HJBs)—basophilic nuclear inclusions—become detectable in peripheral blood smears [1, 3, 5–7, 9–11].
Previous findings [6] indicate that HJBs detection serves as a screening tool for suspected functional hyposplenism and that splenic volumes in these patients are frequently below ideal levels. However, whether reduced spleen volume directly contributes to an increased risk of infection or influences infection outcomes remain unclear. Therefore, this study aims to clarify the relationship between spleen volume and infection incidence in non-splenectomized patients with HJBs. We hypothesized that computed tomography (CT)-based assessment of spleen volume could aid in diagnosing functional hyposplenism and identifying the need for intensified preventive strategies in at-risk individuals.
Materials and methods
Following approval from the Institutional Review Board of Aichi Medical University School of Medicine (2023-239), patients with HJBs detected in peripheral blood smears via a standard optical microscope at Aichi Medical University Hospital from January 2014 to September 2024 were identified. HJBs were considered present when at least one red blood cell containing an HJB was identified in a single microscopic field at × 400 magnification. Patients aged ≤ 15 years or those lacking available computed tomography (CT) imaging were excluded. Retrospective data collection included underlying conditions, infections, and splenic volume measured on CT. Cases of sepsis, pneumonia, and urinary tract infections (UTIs) were included if confirmed via positive culture results and subsequently treated. Splenic volumes were quantified using CT imaging and analyzed with ZIOSTATION2 software (Ziosoft Inc., Tokyo, Japan). Ideal splenic volume was calculated using the following formula: 6.47 × body weight × age^−0.31^ (mL) [12]. The relative difference between measured and ideal splenic volumes was calculated as a percentage using the following formula: (the measured splenic volume -the ideal splenic volume)/the ideal splenic volume (%). Fisher’s exact test and logistic regression analysis were conducted to identify infection risk factors using the EZR software package for all analyses [13].
Results
Patient characteristics
Overall, 95 patients with HJBs who had not undergone splenectomy were included in this study. A representative peripheral blood smear demonstrating the presence of HJBs is shown in Fig. 1. The median age was 66 years (range, 16–95), with 68 (72%) being male. The median spleen volume was 34 mL (range, 1.2–410 mL), while the median ideal spleen volume was 210 mL (range, 110–320 mL). A representative CT image of a patient with marked splenic atrophy (measured volume, 5.9 mL) is shown in Fig. 2. In most cases, the measured spleen volume was smaller than the ideal spleen volume, with a median relative difference of –82% (range, –99 to 97%) (Fig. 3).Fig. 1. Peripheral blood smear of a representative patient showing HJBs indicated by red arrows (Wright–Giemsa stain; total magnification, × 400). HJB Howell–Jolly bodyFig. 2Abdominal CT image of a representative patient demonstrating marked splenic atrophy (red arrow). The measured splenic volume was 5.9 mL. CT computed tomographyFig. 3Measured vs. ideal spleen volume. Scatter plot comparing measured spleen volumes and ideal spleen volumes in 95 patients. Each dot represents one patient. The dashed line (y = x) indicates equality between measured and ideal volumes. Most patients fall below the line, indicating reduced spleen volume relative to ideal
The most common underlying condition was cancer affecting 35 patients (37%), followed by alcoholic liver disease (12 patients, 13%), malignant hematological diseases (8 patients, 8.4%), post-hematopoietic stem cell transplantation (5 patients, 5.3%), and splenic ischemia (5 patients, 5.3%). Other conditions included inflammatory bowel disease, benign hematological diseases, abdominal aortic aneurysm (each in 3 patients, 3.2%), collagen diseases (2 patients, 2.1%), and various other conditions (19 patients, 20%) (Table 1). Table 1. Characteristics of patients with HJBs excluding splenectomized patientsVariableValueVariableValueNumber of cases95Underlying condition diseases, n (%)Patients age, years, median (range)66 (16–95) Cancer35 (37)Patient sex, n (%) Alcoholic liver diseases12 (13) Male68 (72) Malignant hematological diseases8 (8.4) Female27 (28) Post hematopoietic stem cell transplantation5 (5.3)Volume of spleen, ml, median (range)34 (1.2–410) Splenic ischemia5 (5.3)Volume of ideal spleen, ml, median (range)210 (110–320) Inflammatory bowel diseases3 (3.2)The relative difference between the measured and ideal splenic volumes, %, median (range)−82 (−99 to 97) Benign hematological diseases3 (3.2) Abdominal aortic aneurysm3 (3.2)Sepsis, n (%)20 (21) Collagen diseases2 (2.1)Pneumonia, n (%)24 (25) Others19 (20)Urinary tract infection, n (%)19 (20)At least one infection, n (%)46 (48)HJBs Howell–Jolly bodies
Infectious characteristics
During the study period, 20 patients (21%) developed sepsis, 24 (25%) had pneumonia, and 19 (20%) experienced UTIs. Overall, 46 patients (48%) developed at least one of these infections—pneumonia, UTI, or sepsis. Among all infections, Klebsiella pneumoniae—an encapsulated bacterium—was the most frequently identified pathogen (Tables 2, 3, and 4). Table 2. Causative pathogens of sepsisVariableValueVariableValueKlebsiella pneumoniae6Veillonella atypica1Escherichia coli3Pseudomonas aeruginosa1Streptococcus pneumoniae2Clostridium perfrigens1Methicillin-resistant coagulase negative Staphylococci2Streptococcus gallolyticus subsp. pasteurianus1Staphylococcus aureus2Staphylococcus lugdunensis1Klebsiella variicola1Enterobacter cloacae complex1Klebsiella earogenes1Enterococcus casseliflavus1Enterococcus faecium1Candida albicans1Elizabethkingia meningoseptica1The total number of infections and pathogens exceeds the number of patients, as some individuals experienced more than one type of infection and multiple pathogens were sometimes isolated from a single infectious episodeTable 3Causative pathogens of pneumoniaVariableValueVariableValueKlebsiella pneumoniae5Schizophyllum commune1Candida albicans4Cryptococcus neoformans1Pseudomonas aeruginosa3Enterococcus raffinosus1MRSA (methicillin-resistant Staphylococcus aureus)3Haemophilus influenzae1Enterococcus faecium2Serratia marcescens1Staphylococcus aureus2Nocardia cyriacigeorgica1Corynebacterium striatum3Klebsiella oxytoca1Escherichia coli2Acinetobacter baumannii complex1Moraxella catarrhalis2Proteus mirabilis1BLNAR (β-lactamase-negative ampicillin-resistant Haemophilus influenzae)2Enterococcus avium1MRCNS (Methicillin-resistant coagulase-negative staphylococci)2Enterococcus faecalis1Acinetobacter baumannii2Candida parapsilosis1Elizabethkingia meningoseptica1Candida lusitaniae1Stenotrophomonas maltophilia1Candida glabrata1Streptococcus agalactiae1The total number of infections and pathogens exceeds the number of patients, as some individuals experienced more than one type of infection and multiple pathogens were sometimes isolated from a single infectious episodeTable 4Causative pathogens of urinary tract infectionVariableValueEscherichia coli5Enterococcus faecalis5Candida albicans4Corynebacterium striatum4Klebsiella pneumoniae3MRSA (methicillin-resistant Staphylococcus aureus)2Proteus mirabilis2Pseudomonas aeruginosa1Veillonella parvula1Streptococcus anginosus1MRCNS (Methicillin-resistant coagulase-negative staphylococci)1Pseudomonas otitidis1Klebsiella oxytoca1Candida glabrata1Streptococcus agalactiae1The total number of infections and pathogens exceeds the number of patients, as some individuals experienced more than one type of infection and multiple pathogens were sometimes isolated from a single infectious episode
Results of statistical analysis
Univariate analysis revealed that patients ≥ 65 years were significantly more likely to develop sepsis than those < 65 years (p = 0.020). Additionally, a spleen volume < 34 mL was significantly associated with sepsis (p = 0.026). The relative difference between the measured and ideal splenic volumes (< −82%) showed a trend toward association with sepsis, although this was not statistically significant (p = 0.077) (Table 5, Fig. 4). Table 5. Infection incidence and clinical factors: univariate analysisVariableNon sepsisSepsis*p valueNon pneumoniaPneumoniap valueNon UTIUTIp valueNon infectionAt least one infectionp *valueAge < 65 yrs3330.0203060.153150.3025110.011Age ≥ 65 yrs4217411845142435History of no malignancy38110.8036130.824090.8023260.41History of malignancy379351136102620Spleen volume ≥ 34 ml4460.0264190.104460.07031190.041Spleen volume < 34 ml3114301532131827The relative difference between the measured and ideal splenic volumes ≥ −82%4160.07737100.484070.3027200.31 < −82%3414341436122226Bold indicate statistically significant differences (p 0.05)Fig. 4. Comparison of sepsis incidence based on clinical factors. Univariate analysis revealed that patients ≥ 65 years were significantly more likely to develop sepsis than those < 65 years (p = 0.020). A spleen volume < 34 mL was significantly associated with sepsis (p = 0.026). A relative difference between measured and ideal splenic volumes (< −82%) showed a trend toward association with sepsis but was not statistically significant (p = 0.077). This figure includes 20 patients who developed sepsis (n = 20)
Regarding other infection types, no clinical factors were significantly associated with pneumonia or UTIs. However, patients ≥ 65 years were significantly more likely to experience at least one infection (p = 0.011), and a spleen volume < 34 mL was also significantly associated with infection occurrence (p = 0.041) (Fig. 5).Fig. 5. Comparison of any infection incidence based on clinical factors. Univariate analysis revealed that patients ≥ 65 years were significantly more likely to experience at least one infection (p = 0.011). Spleen volume < 34 mL was also significantly associated with infection (p = 0.041). This figure includes 46 patients who experienced at least one infection (n = 46)
In the multivariate logistic regression analysis, age ≥ 65 years remained an independent risk factor for sepsis (odds ratio [OR], 4.0; 95% confidence interval [CI] 1.1–15; p = 0.039), as did spleen volume < 34 mL (OR, 3.0; 95% CI 1.0–8.9; p = 0.047).
Age ≥ 65 years was also significantly associated with the development of at least one infection (OR, 3.1; 95% CI 1.3–7.6; p = 0.013). Spleen volume < 34 mL showed a trend toward association but did not reach statistical significance (OR, 2.2; 95% CI 0.96–5.3; p = 0.064) (Table 6). Table 6. Sepsis incidence and clinical factors: multiple logistic regression modelVariableSepsisOR95% CI*p valueAge (< 65 vs. ≥ 65 yrs)4.01.1–150.039Spleen volume (< 34 vs. ≥ 34 ml)3.01.0–8.90.047At least one infectionOR95% CIp *valueAge (< 65 vs. ≥ 65 yrs)3.11.3–7.60.013Spleen volume (< 34 vs. ≥ 34 ml)2.20.96–5.30.064Bold indicate statistically significant differences (p 0.05)
Discussion
In this study, infection risk in non-splenectomized patients exhibiting HJBs was investigated, revealing that older age (≥ 65 years) and reduced splenic volume (< 34 mL) independently increased susceptibility to sepsis. Although a significantly smaller actual-to-ideal splenic volume ratio (≤ 82%) showed a trend toward sepsis risk, this difference was not statistically significant. These findings suggest that a spleen volume threshold of 34 mL may be clinically meaningful for identifying patients at higher risk of severe infections, particularly sepsis. Moreover, older age emerged as a robust predictor of infection. This highlights the potential value of targeted prophylactic measures—such as vaccinations and antibiotic therapy—in patients with suspected functional hyposplenism.
The precise mechanisms underlying splenic atrophy in functional hyposplenism remain poorly understood. Picardi et al*.*[14] hypothesized that immune-mediated processes similar to those causing pancreatic atrophy in diabetes may underlie progressive splenic shrinkage. Supporting this immunological perspective, the study shows that patients with autoimmune pancreatitis initially presented with splenomegaly, which later progressed to splenic atrophy after steroid treatment [15]. The proposed mechanism involves the expansion of autoreactive lymphocytes that deplete naive lymphocyte populations, ultimately reducing spleen volume. Similarly, experimental studies in murine models show that persistent antigen presentation can induce splenic atrophy [16]. Consistent with these observations, a case of prolonged chronic graft-versus-host disease (GVHD) is associated with ongoing splenic atrophy [5], further supporting an immune-mediated etiology. Although these findings strongly suggest an immunological basis, further research is warranted to elucidate the precise biological pathways involved.
HJBs are well-recognized markers of impaired splenic function under standard light microscopy [3–6]. Although HJBs’ sensitivity and specificity may be lower than those of more specialized tests—such as radioisotope scanning, flow cytometry for IgM^+^ CD27^+^ B cells, or pitted erythrocyte counts [6, 17–20]—their simplicity and low cost make them a practical screening method across diverse clinical settings. Patients with detectable HJBs could undergo additional confirmatory testing or closer clinical monitoring, especially if imaging also reveals reduced splenic volume. Integrating HJBs detection with imaging findings enhances the ability of clinicians to identify individuals at risk for functional hyposplenism.
CT–based measurement of the splenic volume provides greater precision than traditional single-dimensional assessments (e.g., measuring the splenic long axis) [12, 15]. Although splenomegaly is commonly reported in radiologic assessment, splenic atrophy is often overlooked or underreported [21]. Although indices such as the spleen index are used to evaluate splenomegaly, statistical reports on splenic atrophy remain limited, and no clear criteria have been established [22]. Whereas Picardi et al. [14] identified a two-dimensional splenic index using ultrasound, our CT-derived volumetric cut-off provides a three-dimensional, operator-independent assessment that can be applied to routine abdominal CT scans, thereby enhancing the clinical utility of imaging-based evaluation for functional hyposplenism. Nevertheless, reduced splenic volume alone does not definitively diagnose functional hyposplenism. Radioisotope-based assays and specialized immunological tests remain the gold standard for confirming true splenic dysfunction [23, 24]. However, these modalities are expensive, require specialized equipment, and may not be readily available in all healthcare settings. Consequently, CT-based spleen volume measurements serve as an accessible and relatively accurate indicator of potential functional hyposplenism—especially when interpreted alongside HJB status [5, 6].
The spleen plays a multifaceted role in immune defense, contributing to antigen presentation, antibody production, phagocytosis, and opsonization of blood-borne pathogens [1]. A previous study [25] shows that functional hyposplenism increases the risk of infection, particularly sepsis. However, quantifying this risk relative to that of splenectomized patients remains challenging, given limited comparative data [26]. In splenectomized individuals, the risk of overwhelming post-splenectomy infection (OPSI) is > 50 times that of the general population, with S. pneumoniae as the predominant causative pathogen (50–90% of cases), followed by H. influenzae type b and N. meningitidis [27]. Functional hyposplenism may confer similar susceptibility; however, direct comparative evidence is lacking [26]. The microorganisms most commonly responsible for OPSI include Streptococcus pneumoniae, Haemophilus influenzae type b, and N. meningitidis, with less frequently reports on Klebsiella pneumoniae and Salmonella typhi, among others [7]. Therefore, a similar distribution of pathogens was expected in our cohort of patients with functional hyposplenism. However, Klebsiella pneumoniae emerged as the most frequently detected organism. This unexpected predominance may reflect the widespread use of effective vaccines against Streptococcus pneumoniae, Haemophilus influenzae type b, and N. meningitides, but no commercially available vaccine currently exists for Klebsiella pneumoniae.
Given this vulnerability, clinical guidelines have increasingly shifted to treating patients with functional hyposplenism similar to those who have undergone splenectomy. In particular, the latest British guidelines17, which reference our single-center research on HJBs detection [6], emphasize that both splenectomized and functionally hyposplenic patients require vaccination against S. pneumoniae, H. influenzae type b, and N. meningitidis. Moreover, lifelong prophylactic antibiotics therapy is recommended for individuals at high risk of pneumococcal infection—especially young children (< 16 years), older adults (> 50 years), patients with poor serological responses, or those with a history of invasive pneumococcal disease. Other high-risk populations include patients with hematological malignancies—particularly those undergoing splenic irradiation, experiencing GVHD, or long-term immunosuppression—as well as those in the early postoperative period following post-splenectomy (within 1–3 years). These recommendations highlight the significance of accurately identifying patients with potential splenic dysfunction, whether anatomical or functional.
Our findings support this approach. Through the establishment of a specific spleen volume threshold (< 34 mL) associated with increased sepsis risk and identifying older age as an additional key predictor, we contribute further details to the existing evidence base. These findings may help clinicians in personalizing preventive strategies, including timely vaccination and antibiotic prophylaxis. Nonetheless, larger prospective studies are warranted to determine the optimal frequency and methodology for monitoring splenic volume. They are also needed to refine prophylactic approaches (e.g., duration of antibiotic use) and to directly compare outcomes between patients with functional hyposplenism and those who have undergone splenectomy.
Despite these findings, this study has some limitations. First, the single-center, retrospective design may limit generalizability, and reliance on culture-positive cases may underestimate the incidence of infection. Second, incomplete data on vaccination status and antibiotic prophylaxis hindered a thorough evaluation of their protective effects. Third, since many patients underwent CT imaging after an infectious event, time-dependent sepsis risks could not be calculated. Finally, although HJB detection is a practical screening tool for splenic dysfunction, its diagnostic accuracy is inferior to that of more specialized methods. Larger prospective studies—particularly those incorporating etiologically stratified cohorts—are required to determine whether specific patient subgroups exhibit distinct infection profiles or require more intensive prophylaxis. A lack of microbiological data meant that subgroup analyses of causative organisms by age or spleen volume could not be conducted in this study. Future studies with larger sample sizes are needed to explore whether specific pathogens are more prevalent in specific subgroups of patients. While CT-based spleen volumetric measurement provides precise splenic function assessment, repeated imaging poses cost and resource challenges. Therefore, further research into alternative or targeted screening protocols may help balance the feasibility and clinical benefits.
Older age (≥ 65 years) and reduced splenic volume (< 34 mL) independently predict sepsis risk in non-splenectomized patients with HJBs. These findings underscore the need to carefully evaluate splenic volume alongside HJBs detection to identify and manage functional hyposplenism. Future prospective investigations should aim to refine prophylactic strategies, establish optimal screening intervals, deepen understanding of the underlying mechanisms, and ultimately improve outcomes in this at-risk population.