Traumatic pancreatic injury successfully bridged through a giant pancreatic pseudocyst
Tomohisa Iwai, Masaki Nishimura, Megumi Tsukamoto, Yusuke Ozaki, Shigeru Iwase, Shin Maeda

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
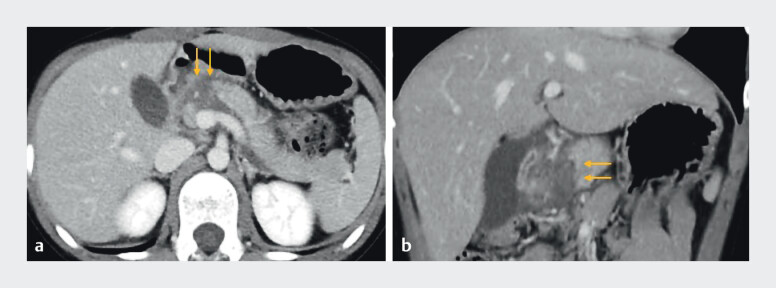 Fig. 1
Fig. 1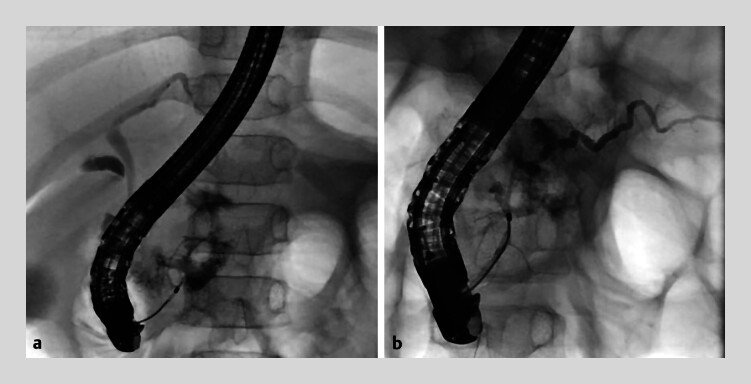 Fig. 2
Fig. 2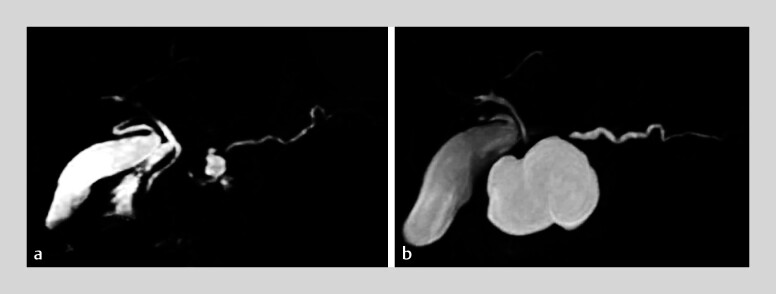 Fig. 3
Fig. 3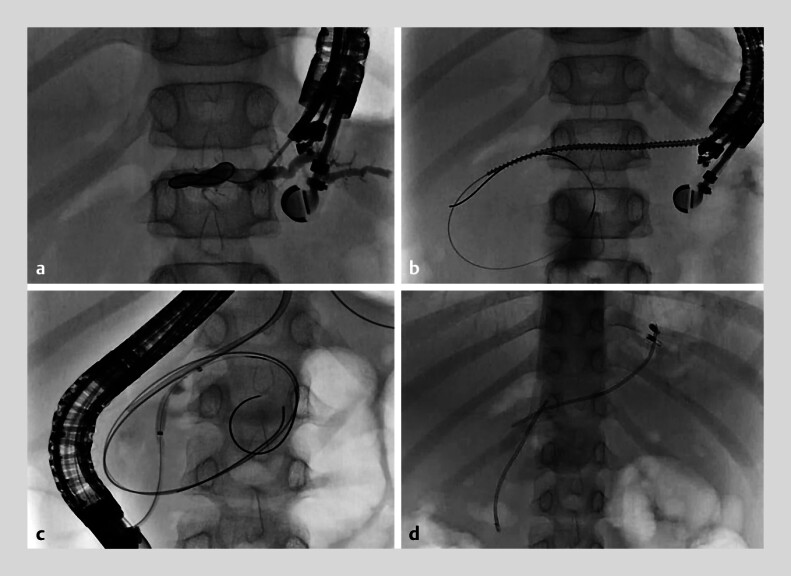 Fig. 4
Fig. 4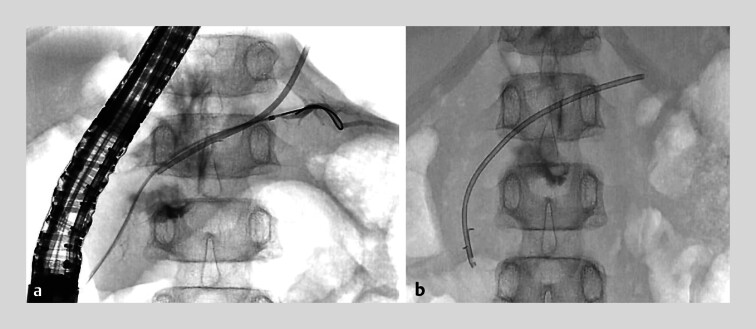 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal Trauma and Injuries · Trauma and Emergency Care Studies · Trauma Management and Diagnosis
Pancreatic injury is a rare form of abdominal trauma and usually requires surgery for deep damage with axial deviation 1 2 . Recently, endoscopic pancreatic stenting for the disconnected pancreatic duct syndrome (DPDS) has been attempted as a minimally invasive treatment 3 4 5 , but difficult situations are often encountered. Here, we present a case of successful rendezvous stenting through a giant pancreatic pseudocyst ( Video 1 ). A 9-year-old boy fell off his bicycle and had handlebar trauma. He had a duodenal perforation and severe damage to the pancreas, resulting in DPDS ( Fig. 1 ). He first underwent mesh repair surgery for duodenal perforation, and endoscopic treatment for DPDS was unsuccessful on two attempts ( Fig. 2 ). Two weeks later, MRCP revealed a small pseudocyst, and conservative management was chosen. The patient developed postprandial abdominal pain and maintained on total parenteral nutrition (TPN) for 2 months. He was transferred to our hospital 2 months after the injury, still on TPN. MRCP performed at our hospital revealed that the pancreatic pseudocyst had enlarged to 45 mm ( Fig. 3 ). Because single-session bridging was considered impossible, two stents were placed in the pseudocyst – one via the transpapillary route and one via EUS-guided pancreatic duct drainage – to establish two points of communication between the pseudocyst and the main pancreatic duct ( Fig. 4 ). In the second session, after balloon dilation of the distal connecting part of the pancreatic duct, a guidewire inserted from the papilla of Vater was advanced across the pseudocyst into the pancreatic duct of the tail, and a transpapillary pancreatic stent was successfully placed through the pseudocyst ( Fig. 5 ). To the best of our knowledge, this is the first report of successful stent bridging through a giant pancreatic pseudocyst caused by trauma.
Traumatic pancreatic injury successfully bridged through a giant pancreatic pseudocyst.Video 1
Computed tomography revealed disconnected pancreatic duct syndrome secondary to handlebar trauma (arrow). a Axial image. b Coronal image.
Fluoroscopic images of endoscopic retrograde cholangiography. Endoscopic pancreatic duct stenting was not achieved after two attempts. a First attempt, day 1 post-injury. b Second attempt, day 20 post-injury.
Magnetic resonance cholangiopancreatography demonstrated a pancreatic pseudocyst at the site of the trauma. a A small pancreatic pseudocyst was formed shortly after the injury. ( b ) The pseudocyst enlarged to 45 mm by the time the patient was transferred to our hospital.
Fluoroscopic images during pancreatic stenting in the first session. a EUS-guided pancreatic duct drainage was performed from the distal pancreatic duct. b The stricture was dilated using a drill dilator. c From the papillary side, the stricture was dilated with a balloon dilator. d Two pancreatic stents were placed in the pancreatic pseudocyst.
Fluoroscopic images of endoscopic retrograde cholangiography during the second session. a A guidewire was successfully advanced into the distal pancreatic duct through the shrunk pancreatic pseudocyst. b Transpapillary bridging with a single stent was achieved, and the transgastric stent was removed.
Endoscopy_UCTN_Code_TTT_1AS_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ho V Patel N Bokhari F Management of adult pancreatic injuries: A practice management guideline from the Eastern Association for the Surgery of Trauma J Trauma Acute Care Surg 20178218519927787438 10.1097/TA.0000000000001300 · doi ↗ · pubmed ↗
- 2Pavlidis E Psarras K Symeonidis N Indications for the surgical management of pancreatic trauma: An update World J Gastrointest Surg 20222753854310.4240/wjgs.v 14.i 6.538PMC 925824235979422 · doi ↗ · pubmed ↗
- 3Ito Y Kenmochi T Irino T Endoscopic management of pancreatic duct injury by endoscopic stent placement: a case report and literature review World J Emerg Surg 201272110.1186/1749-7922-7-2122788538 PMC 3422996 · doi ↗ · pubmed ↗
- 4Ishii K Itoi T Tsuchiya TEUS-guided pancreatic duct rendezvous in a child with traumatic pancreatic duct disruption Gastrointest Endosc 20148051952025127948 10.1016/j.gie.2014.06.044 · doi ↗ · pubmed ↗
- 5Karpuzcu H Erdoğan C The clinical efficacy and safety of ERCP in traumatic pancreatic injuries: a systematic review and meta-analysis World J Emerg Surg 2025205210.1186/s 13017-025-00631-540533798 PMC 12178067 · doi ↗ · pubmed ↗