Endoscopic immediate hemostasis strategy for palatal hematoma induced by linear endoscopic ultrasound
Ye Han, Sheng Wang, Siyu Sun

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
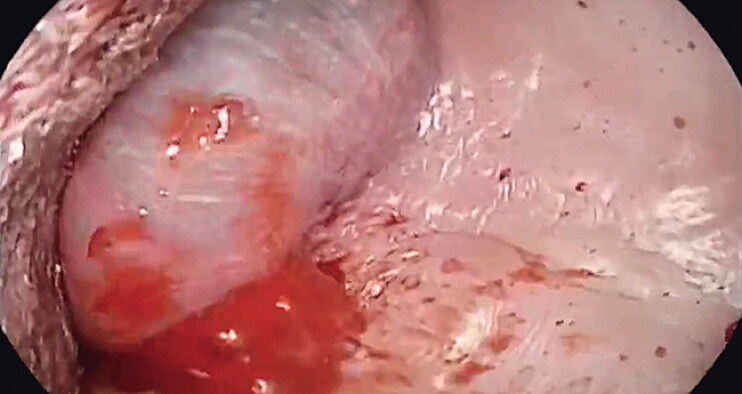 Fig. 1
Fig. 1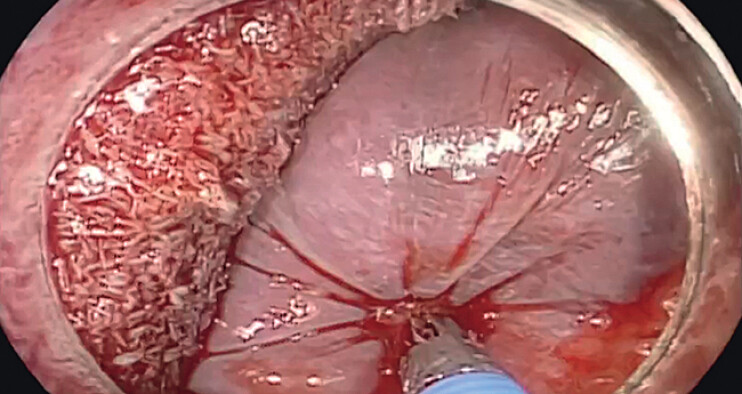 Fig. 2
Fig. 2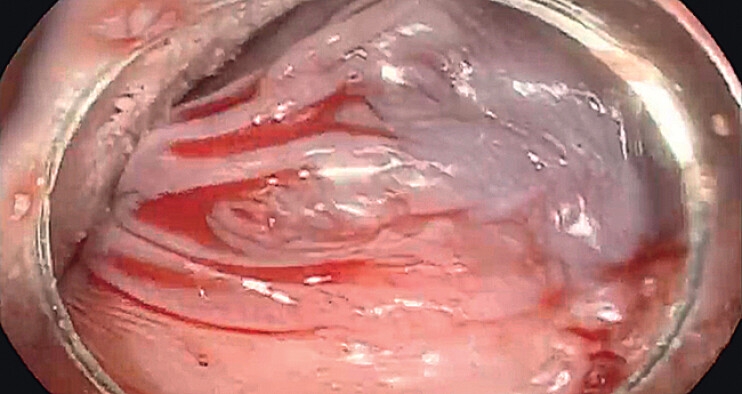 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOtolaryngology and Infectious Diseases · Nasal Surgery and Airway Studies · Hemophilia Treatment and Research
Linear echoendoscopes have the ultrasound transducer located at the tip, which make them more rigid than standard endoscopes. Although complications are rare 1 2 , endoscopic ultrasonography (EUS) carries inherent risks, particularly hemorrhage 3 . We report a rare case of a palatal hematoma during diagnostic EUS. The bleeding was subsequently controlled by using biopsy forceps under endoscopic vision.
A 61-year-old male was referred to our department for an EUS diagnosis under general anesthesia. During the examination, fresh blood was observed at the corner of the patientʼs mouth. The gastroscope was immediately replaced ( Video 1 ), and endoscopic visualization revealed hematoma formation with active bleeding in the upper palate ( Fig. 1 ). Under non-intubated general anesthesia, the patient was at risk of aspiration, and hemostasis was urgent. Under gastroscopy, fresh blood was rapidly aspirated from the mouth, and the bleeding point was accurately located. First, we used the gastroscope itself to compress the hematoma and reduce its tension. And then, the biopsy forceps was inserted to precisely clamp the bleeding vessel ( Fig. 2 ). After four rounds of biopsy forceps compression, each lasting 2–3 minutes, hemostasis was achieved ( Fig. 3 ). When the patient woke up, there was no bleeding in the mouth, and he had no discomfort when drinking water 2 hours later. The patient did not experience bleeding symptoms again during follow-up on the second day.
The video shows a palatal hematoma formation and bleeding during diagnostic EUS. The bleeding was subsequently controlled by using biopsy forceps under endoscopic vision.Video 1
Endoscopic visualization revealed hematoma formation with active bleeding in the upper palate.
The biopsy forceps was inserted to precisely clamp the bleeding vessel.
Bleeding clearly stopped after releasing the biopsy forceps, with no further expansion of the hematoma.
Standard treatments for oral bleeding include gauze packing, surgical suturing, and hemostatic sponges 4 , with no reported cases of endoscopic hemostasis. Conventional endoscopic hemostasis methods involve hemostatic clips and electrocoagulation, which cause significant postoperative discomfort and impair short-term quality of life. In our case, endoscopic hemostasis using biopsy forceps compression achieved immediate, effective, and precise hemostasis. No adverse events such as coughing or aspiration occurred. This treatment strategy has great clinical practicality, particularly during EUS procedures.
Endoscopy_UCTN_Code_CPL_1AH_2AC
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lakhtakia S Complications of diagnostic and therapeutic Endoscopic Ultrasound Best Pract Res Clin Gastroenterol 20163080782310.1016/j.bpg.2016.10.00827931638 · doi ↗ · pubmed ↗
- 2Mahajan G Bhasin D Telaprolu H Unusual complication of central venous catheter detected on contrast-enhanced EUS (with video)Endosc Ultrasound 20231229229336204802 10.4103/EUS-D-22-00018 PMC 10237611 · doi ↗ · pubmed ↗
- 3Ohno A Fujimori N Harada N Rescue technique for bleeding after placement of plastic stent in EUS-guided hepaticogastrostomy (with videos)Endosc Ultrasound 20231234734810.1097/eus.000000000000000637693113 PMC 10437201 · doi ↗ · pubmed ↗
- 4Sohn JB Lee H Han YS When do we need more than local compression to control intraoral haemorrhage?J Korean Assoc Oral Maxillofac Surg 20194534335031966979 10.5125/jkaoms.2019.45.6.343PMC 6955419 · doi ↗ · pubmed ↗