Multiple Pyogenic Arthritis Caused by Edwardsiella tarda Bacteremia: A Case Report and Literature Review
Ryuto Yokoyama, Kenya Yarimizu, Yu Onodera

TL;DR
A rare case of multiple pyogenic arthritis caused by Edwardsiella tarda bacteremia in an elderly man with multiple risk factors was successfully treated with intensive care.
Contribution
This is the first reported case of multiple pyogenic arthritis caused by Edwardsiella tarda bacteremia.
Findings
The patient developed multiple pyogenic arthritis and septic shock from Edwardsiella tarda bacteremia.
Intensive care, including antibiotics and surgical debridement, led to clinical improvement.
Early diagnosis and treatment are crucial for managing severe E. tarda infections in immunocompromised patients.
Abstract
Infection with Edwardsiella tarda, a Gram-negative rod found in freshwater and seawater, is typically associated with the ingestion of raw fish and commonly causes enteritis, liver abscess, cholangitis, and cholecystitis in humans. However, multiple pyogenic arthritis, which have not been previously reported, are considered exceedingly rare. Herein, we report a case of E. tarda bacteremia that resulted in multiple pyogenic arthritis and septic shock, which was successfully treated with intensive care. An 84-year-old man with a history of prostate cancer, diabetes mellitus, and chronic kidney disease was transferred to our hospital for swelling and pain in the left shoulder, following initial treatment for pyogenic arthritis of the left hip at a previous hospital. Imaging revealed the formation of abscesses in the shoulders and hips. He underwent emergent debridement of the left shoulder…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
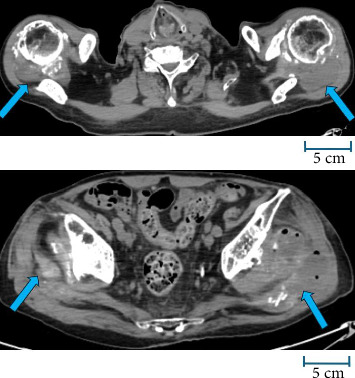 Figure 1
Figure 1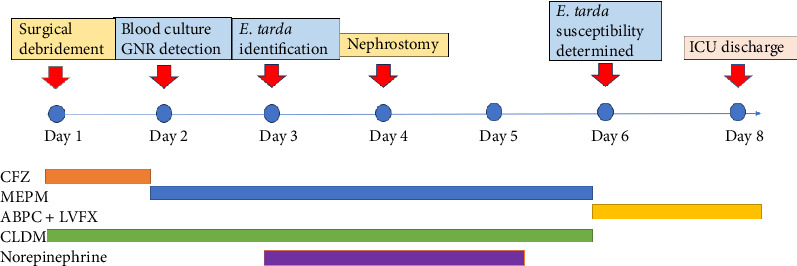 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAquaculture disease management and microbiota · Vibrio bacteria research studies · Biological Research and Disease Studies
1. Introduction
Edwardsiella tarda is a Gram-negative bacillus found in freshwater and seawater. Infection with E. tarda, typically associated with the ingestion of raw fish [1], most commonly causes enteritis, liver abscess, cholangitis, and cholecystitis in humans [2, 3]. The most common underlying disease leading to bacteremia is cancer, accounting for 65% of the cases; patients with immunosuppression, such as those with cancer, are highly likely to develop severe complications [3]. Although bacteremia itself is rare, the mortality rate can be as high as 40% [4]. Previous reports have described monoarticular septic arthritis caused by E. tarda, but polyarticular involvement has rarely been documented. The multiplicity of joint involvement in the present case may be attributed to sustained bacteremia and hematogenous dissemination, possibly facilitated by impaired host immunity. This case highlights the potential for E. tarda infection to cause disseminated musculoskeletal complications even in the absence of external trauma. Herein, we report a case of E. tarda bacteremia that resulted in multiple pyogenic arthritis and septic shock, which was successfully treated with intensive care.
2. Case Presentation
An 84-year-old man presented with the chief complaint of bilateral shoulder pain. His medical history included prostate cancer, diabetes mellitus, hypertension, chronic kidney disease, osteoarthritis of the hip, and left ureteral calculus. Additionally, the patient had been hospitalized 4 months prior to the current admission for terminal ileitis. He had been prescribed azilsartan/amlodipine, tramadol, empagliflozin, mecobalamin, limaprost, and loxoprofen. The patients had no known allergies.
Three days before admission, the patient fell at home and developed left hip pain. He was diagnosed with pyogenic arthritis of the left hip at another hospital and underwent femoral head resection and debridement with cefazolin therapy. The following day, the patient developed swelling and pain in the left shoulder, and approximately 100 mL of purulent fluid was aspirated.
Since the previous facility was unable to manage the condition, he was transferred to our tertiary care hospital.
On arrival, his Japan Coma Scale score was 2, Glasgow Coma Scale score was E4V4M6, respiratory rate was 18 breaths/min, heart rate was 86 bpm, blood pressure was 115/61 mmHg, temperature was 37.5°C, and peripheral oxygen saturation was 96% (room air). Physical examination revealed bilateral shoulder swelling and pain with a limited range of motion in the left shoulder.
Laboratory testing results showed elevated C-reactive protein, procalcitonin, blood urea nitrogen, creatinine, and D-dimer and decreased levels of hemoglobin, platelets, and calcium (Table 1). Positive blood cultures for E. tarda were obtained in two of two sets (Table 2). Computed tomography revealed abscesses in both shoulders and hips (Figure 1).
Following admission, debridement of the left shoulder was performed, and the patient was admitted to the intensive care unit (ICU) for a local gentamicin infusion. On hospital Day 2, Gram-negative rods were identified in blood cultures, prompting an antibiotic change to meropenem. On Day 3, the organism was confirmed to be E. tarda, and the patient was diagnosed with multiple pyogenic arthritis due to E. tarda bacteremia. Circulatory instability developed on the same day, with the systolic blood pressure dropping to 50 mmHg, necessitating norepinephrine administration. Echocardiography performed on Day 4 revealed no evidence of infective endocarditis. On Day 4, oliguria developed, and a bedside ultrasound examination by a urology specialist revealed left hydronephrosis (Grade 3). Left percutaneous nephrostomy was performed due to suspected ureteral obstruction caused by a left ureteral stone. There was no evidence of urinary tract infection. The hemodynamic status stabilized on Day 5. On Day 6, antimicrobial susceptibility to E. tarda was confirmed. Consequently, the antimicrobial therapy was modified to ampicillin and levofloxacin, which were empirically selected based on the clinical judgment of the multidisciplinary team at that time. On Day 8, the patient was discharged from the ICU. Repeated blood cultures on Day 6 yielded negative results (Figure 2).
3. Discussion
In the present case, the patient was considered to have developed multiple pyogenic arthritides as a result of E. tarda bacteremia. A PubMed search using the terms “Edwardsiella tarda” [MeSH] OR “Edwardsiella tarda” [tiab] yielded 345 articles published in the past 5 years. Most of the existing reports describe hepatobiliary infections as the primary manifestation of E. tarda infection [5–7]. In contrast, musculoskeletal infections are rarely reported, although a few recent cases of vertebral osteomyelitis have been documented [8]. While rare manifestations of E. tarda bacteremia, such as necrotizing fasciitis, meningitis, intra-abdominal abscess, empyema, and infective endocarditis, have been described [9–13], to our knowledge, there have been no reports of multiple pyogenic arthritis. Thus, this case represents a significant contribution to the accumulation of knowledge regarding E. tarda bacteremia. The incidence of E. tarda bacteremia has been reported to be 0.004% (38/9368), which is extremely low [3]. Among the diseases caused by E. tarda bacteremia, hepatobiliary infections account for 84.8% (32/38). Malignancy was the most common underlying condition, present in 65.8% (25/38) of the cases, 23.7% (9/38) of which progressed to sepsis. The all-cause mortality rate was 8.6% (3/35) at 30 days and 25.8% (8/31) at 90 days. A separate study involving 182,668 sets of blood cultures also demonstrated similar findings, with hepatobiliary infections being the predominant clinical presentation and malignancy the most frequent comorbidity [14]. In the present case, the patient had a history of malignancy and diabetes mellitus, suggesting a potentially increased susceptibility to E. tarda bacteremia.
We reviewed 12 reported cases of septic shock caused by E. tarda infection over the past 15 years (Table 3). The most common underlying disease was liver abscess (33.3%, 4/12), followed by soft tissue infections or necrotizing fasciitis (25.0%, 3/12), and biliary tract infections (16.6%, 2/12). The mortality rate was 33.3% (4/12), with necrotizing fasciitis accounting for 50% (2/4) of the fatal cases. Carbapenem antibiotics were selected as the initial antimicrobial therapy in 83.3% (10/12) of the cases, and source control by drainage was performed in 66.6% (8/12). These findings suggest that the mortality rate in patients who develop septic shock may be higher than that in patients with bacteremia alone. Among the four fatal cases, only one patient—who underwent surgical debridement—survived, while drainage was not performed in the remaining three, who had pneumonia or soft tissue infections. Comparing the drainage group and nondrainage group, the survival rate was 87.5% (7/8) in the drainage group and 25.0% (1/4) in the nondrainage group. Fisher's exact test showed a tendency toward higher survival in the drainage group, but no significant difference was observed (p = 0.0667). The hazard ratio for survival was 3.50 (95% CI: 0.63–19.5), and the odds ratio was 21.0 (95% CI: 0.96–456.7). Although statistical significance was not demonstrated, there is potential for improved survival rates. These observations underscore the crucial role of source control in managing septic shock. In the present case, early surgical debridement was performed for pyogenic arthritis, and early diagnosis and timely surgical intervention are likely to have contributed to the patient's survival.
E. tarda has been suggested to exist in a state of asymptomatic infection [15]. In general, patients with cancer are at an increased risk for asymptomatic infection or reactivation of pathogens, such as Mycobacterium tuberculosis and other bacteria [16, 17]. In the present case, reactivation from a latent E. tarda infection might have occurred. The patient had been hospitalized 4 months prior to the current admission for terminal ileitis. At that time, although C-reactive protein levels were markedly elevated (25 mg/dL), the clinical symptoms and imaging findings of enteritis were mild, and the patient was treated with a 5-day course of intravenous cefazolin before being discharged. Given the patient's history of prostate cancer and diabetes mellitus, he was likely in an immunocompromised state. Although stool culture was not performed in this case, E. tarda has been reported to be isolated from 0% to 0.8% of clinical stool specimens [18]. Although persistent colonization is uncommon, these findings suggest that E. tarda may be transiently carried in the intestinal tract. Therefore, the possibility remains that E. tarda persisted as a subclinical infection due to insufficient antimicrobial therapy. In immunocompromised individuals, such as those with malignancy or diabetes, E. tarda should be considered a potential pathogen in cases of enteritis, and an adequate duration of antimicrobial therapy may be warranted.
4. Conclusions
Multiple pyogenic arthritis caused by E. tarda bacteremia is extremely rare and scarcely reported, yet it has the potential for rapid clinical deterioration. Our patient had multiple risk factors, including cancer, diabetes, and hypertension, which might have predisposed him to a severe disease course. Early diagnosis, appropriate antibiotic therapy, surgical debridement, and intensive care are crucial for patient survival. Additionally, early transfer to a tertiary center can also improve outcomes. Even rare infections, such as E. tarda, should be considered in the differential diagnosis of immunocompromised patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Leung K. Y. Siame B. A. Tenkink B. J. Noort R. J. Mok Yu-K. Edwardsiella tarda–Virulence Mechanisms of an Emerging Gastroenteritis Pathogen Microbes and Infection 2012141263410.1016/j.micinf.2011.08.0052-s 2.0-8435516168421924375 · doi ↗ · pubmed ↗
- 2Hirai Y. Asahata-Tago S. Ainoda Y. Fujita T. Kikuchi K. Edwardsiella tarda Bacteremia. a Rare but Fatal Water- and Foodborne Infection: Review of the Literature and Clinical Cases From a Single Centre The Canadian Journal of Infectious Diseases & Medical Microbiology 201526631331810.1155/2015/7026152-s 2.0-8495277448526744588 PMC 4692300 · doi ↗ · pubmed ↗
- 3Hasegawa K. Kenya M. Suzuki K. Ogawa Y. Characteristics and Prognosis of Patients With Edwardsiella tarda Bacteremia at a Single Institution, Japan, 2005–2022 Annals of Clinical Microbiology and Antimicrobials 2022211 p. 5610.1186/s 12941-022-00548-w PMC 973064736476326 · doi ↗ · pubmed ↗
- 4Wang I.-K. Kuo H.-L. Chen Y.-M. Extraintestinal Manifestations of Edwardsiella tarda Infection International Journal of Clinical Practice 200559891792110.1111/j.1742-1241.2005.00527.x 2-s 2.0-3364465738816033613 · doi ↗ · pubmed ↗
- 5Hasegawa M. Sanmoto Y. Recurrent Cholangitis and Bacteraemia due to Edwardsiella Tarda: A Case Report Oxford Medical Case Reports 202420241 p. omad 14810.1093/omcr/omad 148PMC 1082331738292162 · doi ↗ · pubmed ↗
- 6Hara C. Tanaka T. Nishiwada S. Kirihataya Y. Yoshimura A. Acute Cholecystitis with Sepsis due to Edwardsiella Tarda: A Case Report Surg Case Rep 202391 p. 18410.1186/s 40792-023-01763-z PMC 1059369337872407 · doi ↗ · pubmed ↗
- 7Tominaga R. Kashiura M. Hatano H. Moriya T. Emphysematous Liver Abscess With Edwardsiella tarda Infection ID Cases 202229 p. e 0154310.1016/j.idcr.2022.e 01543 PMC 923461235769544 · doi ↗ · pubmed ↗
- 8Tsuchiya K. Okano I. Miyamoto Y. Thoracic Spondylitis Associated With Sepsis and Neurological Deficit Caused by Edwardsiella Tarda: A Case Report Spine Surg Relat Res 20237654755010.22603/ssrr.2023-001738084220 PMC 10710892 · doi ↗ · pubmed ↗