The Endoscopic Versus Open Approach for Anterior Skull Base Tumors: A Systematic Review of Comparative Outcomes and a Framework for Surgical Selection
Ubaid Ullah Mian, Alishba Hameed, Touba Azeem, Sajjad Ullah, Muhammad Idris Khan, Hammad Iftikhar, Umar Farooq, Meer Wais, Jibran Ikram

TL;DR
This review compares endoscopic and open surgical approaches for anterior skull base tumors, finding that endoscopic methods offer better outcomes for certain tumors while open approaches are better for more complex cases.
Contribution
The paper provides a systematic review and a decision-making framework for selecting between endoscopic and open approaches for anterior skull base tumors.
Findings
Endoscopic endonasal approach (EEA) is linked to better quality of life and less morbidity for midline tumors.
Open approaches are preferred for tumors with lateral extension, large size, or complex vascular involvement.
EEA and open approaches have distinct complication profiles, such as CSF leakage and meningitis.
Abstract
Anterior skull base tumors (ASBTs) pose significant surgical challenges due to their proximity to critical neurovascular structures. Surgical management has evolved with the adoption of both endoscopic and open approaches. This systematic review synthesizes evidence comparing these approaches in terms of complications, outcomes, and indications. We conducted a systematic review following the PRISMA guidelines, analyzing studies published between 1981 and 2022. A total of 1200 articles were initially identified from databases including PubMed, MEDLINE, JSTOR, and ScienceDirect, with 60 relevant references ultimately included. Data extraction focused on surgical approaches, tumor types, prevalence, and complications. ASBTs exhibit varying prevalence and associated complications depending on their type. Meningiomas account for nearly one-third of all cases, with an annual incidence of 2…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
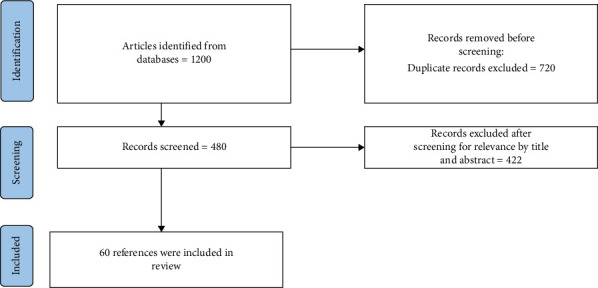 Figure 1
Figure 1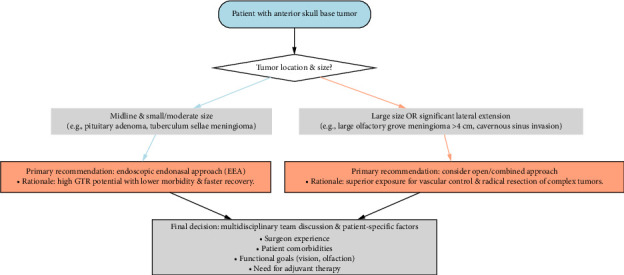 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMeningioma and schwannoma management · Pituitary Gland Disorders and Treatments · Head and Neck Surgical Oncology
1. Introduction
Anterior skull base tumors (ASBTs) include a wide range of neoplasms [1] that originate anatomically in the area between the skull base and facial structures. These tumors present considerable surgical challenges owing to their proximity to eloquent neurovascular structures, such as the brain, optic nerves and chiasm, and the internal carotid arteries (ICAs). With time, significant breakthroughs in surgical procedures have brought about a revolutionary transformation in the treatment of malignant tumors. There are two main techniques often used for the resection of tumors, namely, endoscopic [2] and open procedures [3]. Each of these approaches has unique benefits and concerns.
Endoscopic procedures include the use of minimally invasive methodologies, which entail employing tiny incisions and specialized devices to access and extract the tumor. These methodologies frequently use endoscopes, providing exceptional viewing and magnification capabilities inside the surgical domain. Compared to conventional open techniques, they provide advantages such as decreased morbidity, shorter hospitalization durations, and expedited recovery periods. The use of endoscopic procedures has become more prevalent in the treatment of cancers situated inside the nasal cavity, paranasal sinuses, and suprasellar area [2].
Open surgical approaches often necessitate larger incisions and may involve the removal of bone to achieve adequate exposure of the tumor. These techniques allow for direct visualization and access to the tumor, facilitating complete resection while minimizing the risk of injury to adjacent critical structures. Open procedures are particularly indicated for larger tumors involving complex anatomical regions such as the anterior cranial fossa, cribriform plate, and ethmoid sinuses, where extensive exposure is required for safe and effective tumor removal [3].
Tumors of the anterior skull base encompass a wide variety of histological types, including meningiomas, esthesioneuroblastomas, chordomas, chondrosarcomas, and squamous cell carcinomas. Among these, meningiomas are the most frequently encountered, accounting for approximately 30% of all cases in this region. These tumors often present unique challenges due to their proximity to critical neurovascular structures, necessitating precise surgical approaches for effective management [4]. Meningiomas often originate from the dura mater and may exhibit either benign or malignant characteristics. Esthesioneuroblastomas are an infrequent kind of neoplasms that originate from the olfactory epithelium. These tumors represent a lesser but noteworthy proportion of cancers located in the anterior skull base.
The incidence of these cancers exhibits variability based on the particular histological subtype and geographical region. As an example, it is seen that meningiomas have a higher prevalence among females. Still, esthesioneuroblastomas display a bimodal age distribution characterized by two distinct peaks occurring throughout infancy and middle life. The prevalence of ASBTs is generally modest, with estimated rates ranging from 1 to 5 instances per 100,000 individuals [1].
The surgical resection of ASBTs is inherently associated with significant risks and potential complications. These include injury to critical neurovascular structures such as the optic nerves, carotid arteries, and frontal lobes, which can lead to visual impairment, cerebrospinal fluid (CSF) leakage, hemorrhage, infection, and neurological deficits [4]. The severity of these complications is influenced by factors such as tumor size, location, invasiveness, and the specific surgical approach employed. While advancements in preoperative imaging, intraoperative monitoring, and surgical technique have been crucial in reducing morbidity and improving outcomes, a definitive consensus on the optimal surgical strategy remains elusive.
Despite these advancements, the choice between endoscopic and open approaches for ASBTs is often debated, centering on the balance between achieving maximal safe resection and minimizing postoperative morbidity. A clear, evidence-based synthesis that compares the outcomes, risks, and specific indications for these approaches across the spectrum of ASBTs is lacking. Therefore, this systematic review aims to critically synthesize the existing literature to address a central clinical question: For which ASBTs and under what conditions does the endoscopic approach provide a superior risk-benefit profile, and when does the traditional open approach remain the gold standard? To answer this, we first posed the following research question: ‘How do endoscopic and open surgical approaches compare in terms of tumor classification, prevalence, and associated surgical complications?' The ultimate goal is to distill the current evidence into a practical framework to aid in preoperative surgical planning and decision-making.
2. Materials and Methods
2.1. Research Question
How do endoscopic and open surgical approaches compare in terms of tumor classification, prevalence, and associated surgical complications in the management of ASBTs?
2.2. Search Strategy
We conducted an extensive search across a multitude of scholarly databases, including PubMed MEDLINE, JSTOR, ScienceDirect, the Cochrane Library, and Google Scholar, in order to comprehensively review articles pertaining to the chosen subject matter and its associated MeSH terms, such as “endoscopic and open approach,” “ASBTs,” and “surgical complications.” Search strategies of the databases are mentioned in Supporting File 1.
2.3. Study Selection and Eligibility Criteria
Our initial database search yielded 1200 records from 1981 through 2022. After compiling the search results, 720 duplicate entries were removed, resulting in 480 unique articles for screening. The titles and abstracts of these 480 articles were screened for relevance, which led to the exclusion of 422 records. A total of 60 studies were included in the final qualitative synthesis. The eligibility of each potentially relevant study was then independently assessed by two reviewers based on the predefined inclusion criteria. Discrepancies between reviewers were resolved through discussion and consensus with a third author. Eligible studies for this systematic review met the following criteria: (1) Study type: Review articles, case studies, retrospective studies, and clinical trials; studies published between 1981 and 2022; and articles following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines or similar methodological frameworks. (2) Population: Patients diagnosed with ASBTs, including meningiomas, esthesioneuroblastomas, pituitary adenomas, craniopharyngiomas, and chordomas. (3) Interventions: Studies comparing endoscopic and open surgical approaches and studies addressing surgical management, including tumor resection and complications. (4) Outcomes: Tumor prevalence and classification. Postsurgical complications, including CSF leaks, carotid injuries, anosmia, meningitis, and infection and clinical presentations, diagnostic findings, and recurrence rates. (5) Language and accessibility: Articles published in English and full-text articles accessible through databases such as PubMed, JSTOR, and ScienceDirect. (6) Date range: Studies published between 1981 and 2022. Exclusion criteria were as follows: (1) Nonsystematic reviews, editorials, commentaries, and opinion pieces and studies not adhering to robust methodological standards (e.g., incomplete or poorly documented data). (2) Studies involving tumors outside the boundary of the anterior skull base. (3) Studies exclusively focusing on radiation therapy, chemotherapy, or other nonsurgical treatments. (4) Articles lacking data on complications, tumor classification, or prevalence rates and studies with insufficient statistical analysis or unclear conclusions. (5) Non-English articles or those without available translations. Abstract-only articles or those requiring subscription access if full-text is unavailable. (6) Studies published before 1981 or after 2022.
The PRISMA flow sheet for the search is given in Figure 1.
2.4. Data Extraction and Outcomes
Data extraction was conducted independently by two of the authors using a predefined abstraction form. Extracted variables included study identifiers (author names and publication year), study design, sample size, tumor types, and surgical approaches (endoscopic, open craniofacial, transcranial, or hybrid techniques) (Table 1). Additionally, data on reported outcomes (tumor resection rates, recurrence, and functional outcomes), complications (CSF leaks, infection rates, vascular injury, and morbidity), and study limitations (sample size, single-center bias, and methodological constraints) were systematically collected. Given the heterogeneity in study designs and outcome reporting, a meta-analysis was not conducted. Instead, a qualitative synthesis was performed to evaluate the comparative efficacy and feasibility of different surgical techniques in skull-based tumor management.
2.5. Study Design and Protocol Registration
This systematic review followed the recommendations of the Cochrane collaboration [5] and the PRISMA guidelines [6]. The study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD42025635109. The title of this manuscript has been refined from the original PROSPERO protocol registration to better reflect the novel decision-making framework developed as a key outcome. The core research question and methodology remain unchanged from the registered protocol.
2.6. Ethical Considerations
No ethical issues were encountered during the study. The study was approved by the Institutional Research and Ethical Review Board (IREB) of Khyber Medical College/Khyber Teaching Hospital, Peshawar, Khyber Pakhtunkhwa, Pakistan, under approval number 548/DME/KMC, dated 08/09/2023.
3. Results
3.1. Overview of Included Studies
A total of 60 studies were included in this review, encompassing a diverse range of methodologies, sample sizes, and objectives. Study types varied widely, including retrospective analyses, prospective trials, meta-analyses, anatomical and technical reports, comparative studies, case series, and systematic reviews. Sample sizes ranged from single-patient case reports [7, 8] to large retrospective cohorts exceeding 1000 participants [9].
Among the included studies, a significant number focused on the efficacy and safety of endoscopic endonasal approaches (EEAs). These studies consistently reported CSF leak as a major complication, with rates ranging from 4% to 20% depending on surgical technique and experience level [2, 4, 10–14]. Other commonly reported complications included cranial nerve (CN) deficits—especially in transcranial approaches—ranging from 10% to as high as 60% in certain tumor resections [15–19].
Quality of life (QoL) outcomes were less frequently addressed, with only a few studies explicitly measuring patient-reported symptoms or functional outcomes postsurgery [19, 20]. Hormonal deficits and endocrine complications, including diabetes insipidus (DI), were common postoperatively in transsphenoidal pituitary surgeries, occurring in up to 20% of cases [9, 12, 21, 22]. Hyponatremia, both transient and delayed, was another concern, with rates peaking on postoperative Days 5–7 [23–25].
Several studies were notable for their comparative insights. Komotar et al. and Shahar et al., for example, highlighted lower morbidity and comparable gross total resection (GTR) rates when using endoscopic approaches compared to traditional transcranial methods [4, 26]. Likewise, Ganly et al. emphasized that high-volume centers achieved reduced complication rates, underscoring the importance of surgical experience [27].
Geographically, the literature included contributions from leading neurosurgical centers globally, reflecting evolving practices and innovations in skull base surgery. A significant body of anatomical and technical studies further complemented the clinical literature, providing foundational knowledge for safe surgical navigation of complex skull base regions [28–32].
Table 1 provides a comprehensive summary of the included studies, detailing surgical approaches, study types, sample sizes, key outcomes, complication rates, and risk of bias. It serves as the primary source of extracted data, offering an overview of the evidence base evaluated in this review.
3.2. Risk of Bias Assessment
The methodological quality of studies comparing endoscopic and open approaches for ASBTs was systematically evaluated using the Newcastle–Ottawa Scale (NOS), which assessed four domains: (1) selection bias (cohort representativeness and diagnostic confirmation), (2) comparability (confounder control), (3) outcome assessment (blinded evaluation), and (4) follow-up adequacy (> 80% retention). Based on these criteria, studies were categorized as low (e.g., Trooboff et al. [33] with PRISMA-compliant methods), moderate, serious (e.g., Schreckinger et al. [12] with missing data), or critical risk of bias. Notably, only Greenberg et al. [19] and Laigle-Donadey et al. [20] evaluated QoL outcomes, revealing a significant evidence gap. Two reviewers independently conducted assessments, resolving discrepancies through consensus.
Analysis revealed substantial variability in risk of bias across the literature. Low-risk studies—including systematic reviews, meta-analyses, and prospective cohorts—employed rigorous methodologies with controlled confounders (tumor size/location and surgeon experience) and standardized outcomes, providing reliable anatomical and procedural data. Moderate-risk retrospective studies offered clinically useful insights into complications (CSF leaks and CN deficits) despite lacking randomization. High-risk studies (single-center retrospectives and case reports) were compromised by selection bias, small samples, and unadjusted confounders, particularly affecting GTR and morbidity outcomes. Given that > 70% of evidence comes from retrospective designs, clinicians should prioritize low-risk studies when comparing surgical approaches. Risk of bias assessment is mentioned in Supporting File 2.
3.3. Comparative Outcomes of Endoscopic vs. Open Approaches by Tumor Type
To directly address the central aim of this review, we synthesized the extracted data to compare the outcomes and risk profiles of endoscopic and open approaches for the most commonly encountered ASBTs. This synthesis, presented in Table 2, moves beyond a generic comparison by stratifying the evidence based on specific tumor pathology and location. The table summarizes the preferred surgical contexts, key advantages, disadvantages, and the relative strength of evidence for each approach, providing a concise, evidence-based guide for preoperative planning.
3.4. QoL Comparison Between Endoscopic and Open Surgical Approaches for ASBTs
Table 3 consolidates evidence on patient-centered outcomes from the included studies. However, a critical finding of this review is the significant lack of dedicated, patient-reported QoL data in the comparative literature. Therefore, this table presents available metrics—such as recovery time, cosmetic results, and complication profiles—that indirectly influence QoL, rather than direct QoL measurements, which were rarely reported.
As summarized in Table 3, the endoscopic approach generally offers advantages in patient recovery, cosmetic outcome, and hospital stay. However, a critical finding of this review is that robust, patient-reported QoL data are severely lacking in the comparative literature. Our analysis confirms that QoL outcomes are significantly under-represented. This finding is corroborated by a recent systematic review dedicated specifically to QoL in anterior skull base surgery, which, despite its publication after our search period, underscores that this remains a critical and unresolved area requiring more standardized and prospective research [38]. The existing evidence gap makes it difficult to draw definitive conclusions about the long-term impact of these surgical approaches on patients' overall well-being.
3.5. The Paradigm of Midline Access: Where Endoscopy Excels
The literature delineates the EEA as a multistep procedure reliant on precise anatomical navigation [28, 29, 39]. Key technical steps, as consistently reported across studies, include preoperative imaging with CT angiography, the establishment of a binostril nasal corridor, and the creation of a nasoseptal flap for reconstruction. The approach is modular, with the specific surgical corridor (e.g., transsellar, transplanum, and transcribriform) determined by the tumor's location in the median sagittal plane, as detailed in Table 4. These modules provide access from the frontal sinus to the cervicomedullary junction, each with distinct anatomical boundaries and risk profiles.
3.6. The Enduring Role of Open Surgery: Managing Complexity and Lateral Extension
Complementing the endoscopic corridors, a spectrum of open approaches provides the extensive exposure necessary for managing large, lateralized, or highly vascularized ASBTs. These approaches, summarized in Table 5, form the foundational repertoire for scenarios where the endoscopic view is insufficient, underscoring the continued critical role of open techniques in the skull base surgeon's armamentarium.
3.7. Classification of Tumors and Epidemiology
Our analysis of the included literature identified a wide spectrum of tumors affecting the anterior skull base, each with distinct histological characteristics, epidemiological patterns, and associated complication profiles. The classification, incidence, and key surgical considerations for the most prevalent tumor types are systematically summarized in Table 6. Meningiomas and pituitary adenomas were the most frequently reported neoplasms in this region, while rarer entities such as esthesioneuroblastomas and chordomas presented unique management challenges and characteristically different risk profiles.
3.8. Complications
The reported complication rates for anterior skull base surgery varied considerably across the included studies, influenced by pathology, tumor size, and surgical approach. For open craniofacial resection, a large multicenter study of 1193 patients reported an overall morbidity rate of 36.3% and a mortality rate of 4.7% [27]. Predictors of complications included comorbid medical conditions, previous radiotherapy, and dural or brain invasion [27].
In contrast, analysis of endoscopic endonasal skull base surgery (ESBS) revealed a distinct complication profile. A large series of 800 procedures reported an aggregate complication rate of 19.4%, which decreased to 9.3% when CSF leaks are excluded [10]. CSF leak was the most prevalent complication, with a cumulative rate of 15.9%; however, the adoption of pedicled nasoseptal flaps reduced this rate to below 5% [1]. The major complications associated with ESBS and corresponding perioperative considerations are detailed in Table 7.
4. Discussion
The primary finding of this systematic review is that the choice between endoscopic and open approaches for ASBTs is not a matter of superiority of one technique over the other, but rather a nuanced decision based on a tumor's anatomical location, size, and histology, balanced against surgical goals and patient-specific factors. Our synthesis allows for the proposal of a practical framework to guide this decision.
4.1. Principal Findings
This systematic review synthesized evidence from 60 studies to compare endoscopic and open surgical approaches for ASBTs. The analysis reveals that the EEA is associated with favorable outcomes for midline tumors, including shorter hospital stays, faster recovery, and superior cosmetic results [1, 28, 34]. Conversely, open approaches provide critical advantages in exposure for large, lateralized, or highly vascularized tumors, facilitating radical resection at the cost of higher overall morbidity [16, 27]. Complication profiles were distinct, with EEA being characterized by a higher incidence of CSF leaks, now substantially mitigated by vascularized flaps [1, 10], while open surgery carried greater risks of significant CN deficits and soft tissue complications [16, 19].
4.2. Interpretation of Comparative Efficacy by Tumor Type
Our synthesis demonstrates that the optimal surgical strategy is not universal but is instead dictated by specific tumor pathology and anatomy. For pituitary adenomas and tuberculum sellae meningiomas, the EEA provides GTR rates comparable to open transcranial surgery while minimizing brain retraction and offering direct access to the sella and suprasellar cistern [4, 28]. This has established EEA as the first-line modality for these midline pathologies [2, 4]. In contrast, for large olfactory groove meningiomas or tumors with extensive invasion into the orbit or cavernous sinus, open approaches remain indispensable. The wider exposure allows for early devascularization and superior control of neurovascular structures, which is crucial for achieving GTR in these complex scenarios [16, 43]. For esthesioneuroblastomas and clival chordomas, a multimodal, often combined, approach is frequently necessary, with EEA providing excellent intranasal visualization and open approaches managing significant intracranial extension [10, 11, 44].
4.3. The Trade-Off: Morbidity, QoL, and Functional Outcomes
A central theme emerging from this review is the critical trade-off between the extent of resection and postoperative morbidity. While open approaches can facilitate more extensive resection for aggressive tumors, this often comes at the cost of longer recovery and higher rates of complications such as anosmia, which is nearly universal after open resection of olfactory groove meningiomas [43]. The EEA, while minimizing these issues, introduces a distinct challenge, primarily CSF leakage, though the adoption of pedicled nasoseptal flaps has reduced this rate to below 5% in many series [1, 10]. Despite the clear impact on patient experience, QoL remains significantly under-reported in the comparative literature. Our finding of this evidence gap is corroborated by a recent systematic review dedicated to QoL outcomes following skull base tumor resection, which found wide variability in methodologies and QoL instruments, limiting analyses to descriptive comparisons rather than robust, quantitative synthesis. Notably, this review revealed that the impact of surgery on QoL is often underestimated by caregivers and is more profound for patients than surgeons anticipate, with a transient decline in QoL observed across almost all studies, regardless of tumor location or surgical approach. Furthermore, the predominance of anterior skull base studies using sinonasal-specific tools such as SNOT-22 and ASBQ introduces measurement bias, as other anatomical regions and functional domains remain underexamined [38]. These findings underscore the urgent need for future prospective research employing standardized, multidimensional, disease-specific QoL instruments to fully quantify and compare the functional trade-offs between open and endoscopic approaches, thereby informing evidence-based surgical decision-making. Future studies must prioritize patient-reported outcomes to fully quantify the functional trade-offs between these surgical corridors.
4.4. Complication Profiles and Management Strategies
The distinct complication profiles of each approach necessitate tailored preventive strategies. In EEA, the most common complication is CSF leakage, with reported rates ranging from 4% to 20% [2, 10, 54]. The evolution of reconstruction techniques, particularly the use of vascularized pedicled flaps, has been the single most important advancement in reducing this risk [1]. ICA injury, though rare (0.2%–1%), is a dreaded complication that requires meticulous preoperative planning and emergency preparedness [53]. Open approaches, while largely avoiding postoperative CSF leaks, are associated with a higher burden of infectious complications, hematomas, and CN deficits, which can be as high as 60% in surgeries involving the cavernous sinus or petroclival region [15, 17, 19]. This underscores the importance of approach selection based on a tumor's specific risk profile.
4.5. A Proposed Framework for Surgical Decision-Making
Based on our comprehensive analysis of the evidence, we propose a structured decision-making framework to guide surgical approach selection for ASBTs. This framework, summarized in Figure 2, integrates tumor characteristics with surgical goals to optimize individual patient outcomes. The algorithm begins with assessment of two critical parameters: tumor location in the midline corridor and size/lateral extension, which serve as the primary determinants for initial approach selection.
As illustrated in Figure 2, the algorithm begins with an assessment of whether a tumor is primarily midline and small-to-moderate in size. If so, an endoscopic approach is recommended to leverage its benefits of reduced morbidity and comparable oncological efficacy. If the tumor is large or exhibits significant lateral extension beyond the paranasal sinuses, an open or combined approach should be strongly considered to ensure adequate exposure for safe dissection and vascular control. It is crucial to emphasize that this framework is designed not as a rigid algorithm but as a foundational guide. The final surgical plan must be determined through a multidisciplinary team discussion, incorporating critical factors such as surgeon experience, patient comorbidities and functional goals, and the need for adjunctive therapies [27, 59].
The synthesis of evidence from the included studies reveals consistent patterns in outcomes, complications, and indications for endoscopic and open approaches. To provide a clear, evidence-based overview of these comparative findings and their clinical implications, the key data are consolidated in Table 8. This summary serves as the foundational evidence for the decision-making framework proposed herein, highlighting the critical trade-offs between oncological efficacy and postoperative morbidity that must be considered during surgical planning.
5. Limitations
This review has some limitations. The included studies exhibited heterogeneity in design, patient populations, and outcome measures, limiting direct comparisons. Most were retrospective, single-center, and had small sample sizes, reducing generalizability. Variations in surgical techniques and inconsistent complication reporting further affected reliability. Additionally, the lack of randomized controlled trials introduced selection bias. Due to these factors, a meta-analysis was not feasible, and findings were synthesized qualitatively.
6. Future Directions
Future research in anterior skull base surgery should prioritize prospective, multi-institutional studies designed with standardized outcome measures. These studies must specifically integrate patient-reported QoL metrics to quantitatively assess the functional trade-offs between endoscopic and open approaches. Furthermore, high-quality comparative studies are needed to validate and refine the proposed decision-making framework, ultimately establishing more precise, evidence-based surgical indications to improve patient care in this challenging field.
7. Conclusion
This systematic review synthesizes 4 decades of evidence to clarify the comparative roles of endoscopic and open approaches in managing ASBTs. The analysis conclusively demonstrates that neither approach is universally superior; rather, their efficacy and safety profiles are intrinsically linked to specific tumor characteristics. The EEA has established itself as the cornerstone for midline pathologies, providing patients with the significant benefits of reduced morbidity, faster recovery, and improved QoL while maintaining high rates of GTR. Conversely, open transcranial approaches retain an indispensable role in the armamentarium, offering the extensive exposure necessary for the safe resection of large, vascular, or laterally invasive tumors.
The principal outcome of this review is a practical, evidence-based decision-making framework that empowers clinicians to navigate this complex choice. By prioritizing tumor location and size as primary selection criteria, the framework provides a clear, logical starting point for surgical planning. Ultimately, this structured approach must be integrated with a multidisciplinary team discussion, considering critical factors such as surgeon expertise, patient-specific comorbidities, and functional goals. It is through this synthesis of robust evidence and personalized clinical judgment that optimal outcomes can be achieved for patients facing these challenging diagnoses.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Patel M. R. Stadler M. E. Snyderman C. H. How to Choose? Endoscopic Skull Base Reconstructive Options and Limitations Skull Base 2010200639740410.1055/s-0030-12535732-s 2.0-7795811603021772795 PMC 3134819 · doi ↗ · pubmed ↗
- 2Nicolai P. Battaglia P. Bignami M. Endoscopic Surgery for Malignant Tumors of the Sinonasal Tract and Adjacent Skull Base: A 10-Year Experience American Journal of Rhinology 200822330831610.2500/ajr.2008.22.31702-s 2.0-4534908637318588765 · doi ↗ · pubmed ↗
- 3Ilie M. D. Jouanneau E. Raverot G. Aggressive Pituitary Adenomas and Carcinomas Endocrinology and Metabolism Clinics of North America 202049350551510.1016/j.ecl.2020.05.00832741485 · doi ↗ · pubmed ↗
- 4Komotar R. J. Starke R. M. Raper D. M. Anand V. K. Schwartz T. H. Endoscopic Endonasal Versus Open Transcranial Resection of Anterior Midline Skull Base Meningiomas World Neurosurgery 2012775-671372410.1016/j.wneu.2011.08.0252-s 2.0-8486131510122120296 · doi ↗ · pubmed ↗
- 5Cochrane Handbook for Systematic Reviews of Interventions Cochrane Training 2025
- 6Page M. J. Mc Kenzie J. E. Bossuyt P. M. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews BMJ 2021372 p. n 7110.1136/BMJ.N 71PMC 800592433782057 · doi ↗ · pubmed ↗
- 7Shields C. B. Valdes-Rodriguez A. G. Tension Pneumocephalus After Trans-Sphenoidal Hypophysectomy: Case Report Neurosurgery 198211568768910.1227/00006123-198211000-000132-s 2.0-00203736756185876 · doi ↗ · pubmed ↗
- 8Solomiichuk V. O. Lebed V. O. Drizhdov K. I. Posttraumatic Delayed Subdural Tension Pneumocephalus Surgical Neurology International 201341 p. 3710.4103/2152-7806.109537 PMC 362239023607059 · doi ↗ · pubmed ↗